
Abstract
Background:
Metabolic syndrome affects 1 in 3 U.S. adults. The primary target of treatment of patients with metabolic syndrome is therapeutic lifestyle change. Numerous animal trials have reported positive effects of Aloe vera in in vivo models of diabetes, but there is a paucity of controlled clinical trials in patients with prediabetes. Thus, the objective of this pilot study was to examine the effect of aloe compared to placebo on fasting blood glucose, lipid profile, and oxidative stress in subjects with prediabetes/metabolic syndrome.
Methods:
This was a double-blind, placebo-controlled Institutional Review Board (IRB)–approved pilot study of two aloe products (UP780 and AC952) in patients with prediabetes over an 8-week period. A total of 45 subjects with impaired fasting glucose or impaired glucose tolerance and having two other features of metabolic syndrome were recruited (n=15/group). Parameters of glycemia [fasting glucose, insulin, homeostasis model assessment (HOMA), glycosylated hemoglobin (HbA1c), fructosamine, and oral glucose tolerance test (OGTT)] and oxidative stress (urinary F2-isoprostanes) were measured along with lipid profile and high-sensitivity C-reactive protein (hsCRP) levels before and after supplementation.
Results:
There were no significant baseline differences between groups. Compared to placebo, only the AC952 Aloe vera inner leaf gel powder resulted in significant reduction in total and low-density lipoprotein cholesterol (LDL-C) levels, glucose, and fructosamine. In the UP780 Aloe vera inner leaf gel powder standardized with 2% aloesin group, there were significant reductions in HbA1c, fructosamine, fasting glucose, insulin, and HOMA. Only the UP780 aloe group had a significant reduction in the F2-isoprostanes compared to placebo.
Conclusions:
Standardized aloe preparations offer an attractive adjunctive strategy to revert the impaired fasting glucose and impaired glucose tolerance observed in conditions of prediabetes/metabolic syndrome.
Introduction
Numerous animal trials have reported positive effects of Aloe vera in in vivo models of diabetes, including lower fasting blood glucose levels in alloxan-induced diabetic mice 4 ; enhanced glucose tolerance in glucose-loaded rats compared to normals 5 ; decreased glucose levels in streptozotocin-induced diabetic rats 6 ; improved liver gluconeogenesis in streptozotocin-induced diabetic rats 7 ; decreased oxidative damage in the brains of streptozotocin-induced diabetic mice 8 ; decreased lipid peroxidation in diabetic rat kidney 9 and liver 10 ; and, in streptozotocin-induced diabetic rats, decreased fasting glucose, normalized lipids and fatty acid compositions in liver and kidney with reduced liver transaminases, and improved plasma insulin levels. 11
In contrast to animal studies, very few human clinical trials have been reported in the literature. The two studies most frequently cited to support the use of aloe in human diabetes 12,13 have methodological flaws, which unfortunately brings the significance of the results into question (nonrandomized and nonblinded, apparently the same population enrolled in both trials, the same decreases in both blood glucose and serum triglycerides in the active groups reported for both trials). A third study, evaluating the effects of bread prepared with aloe gel consumed twice daily for 3 months in subjects with heart disease reported an incidental finding of decreased fasting and postprandial blood glucose levels in the subjects who also had a diagnosis of diabetes. 14 Additionally, anecdotal reports of beneficial effects of aloe in clinical diabetes also exist.
Recently, Huseini et al. examined the effect of Aloe vera gel in hyperlipidemic type 2 diabetic patients who were already on antiglycemic medications and reported that aloe gel (300 mg twice a day for 2 months compared to placebo) significantly lowered fasting blood glucose, glycosylated hemoglobin (HbA1c), total and low-density lipoprotein cholesterol (LDL-C) levels with no other side effects. 15 However, there are no reports of Aloe vera supplementation in patients with prediabetes/metabolic syndrome. Thus, the overall objective of this pilot study is to examine the effect of two aloe products compared to placebo on fasting blood glucose, lipid profile, and biomarkers of oxidative stress in an 8-week study.
Subjects and Methods
This was a double-blind, placebo-controlled study. The test products used were supplied by Unigen Inc., and investigators and volunteers were blinded to treatment assignment. The study received Institutional Review Board (IRB) approval, and all subjects provided informed consent. The products used were: Aloe product 1, UP780, an Aloe vera inner leaf gel powder standardized with 2% aloesin, 500-mg capsules, 1 capsule twice a day (b.i.d.); aloe product 2, QMatrix or AC952, an Aloe vera inner leaf gel powder, 500-mg capsules, 1 capsule b.i.d; placebo capsules, 1 capsule b.i.d. All products were dispensed to the subjects by the Investigational Drug Services.
Study subjects
All study subjects had three features of the metabolic syndrome, of which at least one feature was abnormal fasting glucose (100–126 mg/dL) or abnormal glucose tolerance [2-h oral glucose tolerance test (OGTT) >140–199 mg/dL] but no history or current clinical evidence of diabetes (type I or II). The selection criteria were as follows. Inclusion criteria were: Females and males >18 years of age to 70 years of age; prediabetes, defined as fasting plasma glucose (FPG) 90–125 mg/dL, or 2-h OGTT 149–199 mg/dL plus any two of the following criteria—waist >35 inches for women and >40 inches for men, triglycerides (TG) >150 mg/dL, HDL-C <40 mg/dL in men and <50 mg/dL in women, and systolic (SBP) or diastolic blood pressure (DBP) >130/85 mmHg. Exclusion criteria were: Prior diagnosis of diabetes, pregnancy/lactation, history of gestational diabetes, currently on any diabetes medication for any indication, history of any other chronic disease, and known allergy to Aloe vera or any products containing Aloe vera.
Only subjects who were willing to maintain a normal diet and exercise at least 100 min per week were included in the study. The subjects also abstained from any other dietary supplements or weight loss programs during the study. All subjects were at least 95% compliant throughout the study as monitored by pill counts. Fasting blood was obtained at baseline and following 8 weeks of supplementation. All subjects underwent a 75-g OGTT and fasting glucose levels at 0, 1, and 2 h was obtained and area under the curve (AUC) was computed.
Routine laboratory tests were performed in the Clinical Pathology laboratory, which is Clinical Laboratory Improvement Amendments (CLIA)–certified and included complete blood counts, lipid profile, glucose, HbA1c, liver function tests, creatinine, and insulin. Fructosamine levels were measured by an enzymatic assay from Diazyme. Briefly, the Diazyme Glycated Serum Protein (GSP) uses proteinase K to digest GSP into low-molecular-weight glycated protein fragments (GPF), and uses Diazyme's specific fructosaminase™, a microorganism-originated amadoriase to catalyze the oxidative degradation of Amadori product GPF to yield PF or amino acids, glucosone, and hydrogen peroxide (H2O2). The H2O2 released is measured by a colorimetric Trinder end-point reaction. The absorbance at 600 nm is proportional to the concentration of fructosamine in the sample.
Urine was collected at baseline and following 8 weeks supplementation (24-h urine) for assessment of urinary microalbumin:creatinine ratio in the Clinical Pathology laboratory and for assessment of urinary F2-isoprostanes. Urinary F2-isoprostanes were measured in urine using the Cayman enzyme immunoassay as described previously. 16
Statistics
All data were analyzed using SAS. Kruskal–Wallis analysis of variance (ANOVA) was computed followed by Wilcoxon tests to assess statistical significance.
Results
A total of 45 subjects with impaired fasting glucose or impaired glucose tolerance and having two other features of the metabolic syndrome were recruited. A total of 14 subjects in placebo, 14 subjects in UP780, and 15 subjects in AC952 groups completed the study, and results are reported. No side effects were reported. Table 1 gives the subject characteristics of all subjects in the study. There were no significant baseline differences between groups. There were no significant changes in complete blood count, aspartate aminotransferase (AST), alanine aminotransferase (ALT), creatinine, before and after supplementation (data not shown). Compliance was very high (95%).
Data are provided as mean±standard deviation (SD).
BMI, body mass index; M/F, male/female; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; HbA1c, glycosylated hemoglobin; AUC, area under the curve; Glu-OGTT, glucose tolerance.
Table 2 provides the effect of Aloe vera supplementation versus placebo on the lipid profile and high-sensitivity C-reactive protein (hsCRP) levels. As seen, compared to placebo, only the AC952 regular Aloe vera inner leaf gel powder preparation resulted in significant reduction on total cholesterol and LDL-C levels. None of the other parameters changed significantly.
Data are provided as mean±standard deviation (SD) except hsCRP, for which the median is provided.
P<0.05 compared to placebo and baseline.
hsCRP, high-sensitivity C-reactive protein; HDL-C, high-density lipoprotein; LDL-C, low-density lipoprotein.
With regard to parameters of insulin resistance and dysglycemia, which are reported in Table 3, in the UP780 Aloe vera inner leaf gel powder standardized with 2% aloesin group, there were significant reductions in HbA1c as well as in fructosamine levels, indicators of glycemic control. While fasting blood glucose was significantly reduced, there were no changes in the AUC of glucose values obtained from the 2-h OGTT. Also, insulin levels were significantly decreased. Thus, in the UP780 group, there was significant reduction in homeostasis model assessment (HOMA), a marker of insulin sensitivity (Fig. 1). In the AC952 aloe group, in addition to a decrease in fructosamine, there were significant reductions in glucose values after supplementation. There were no changes in the urinary microalbumin:creatinine ratios in any of the groups.
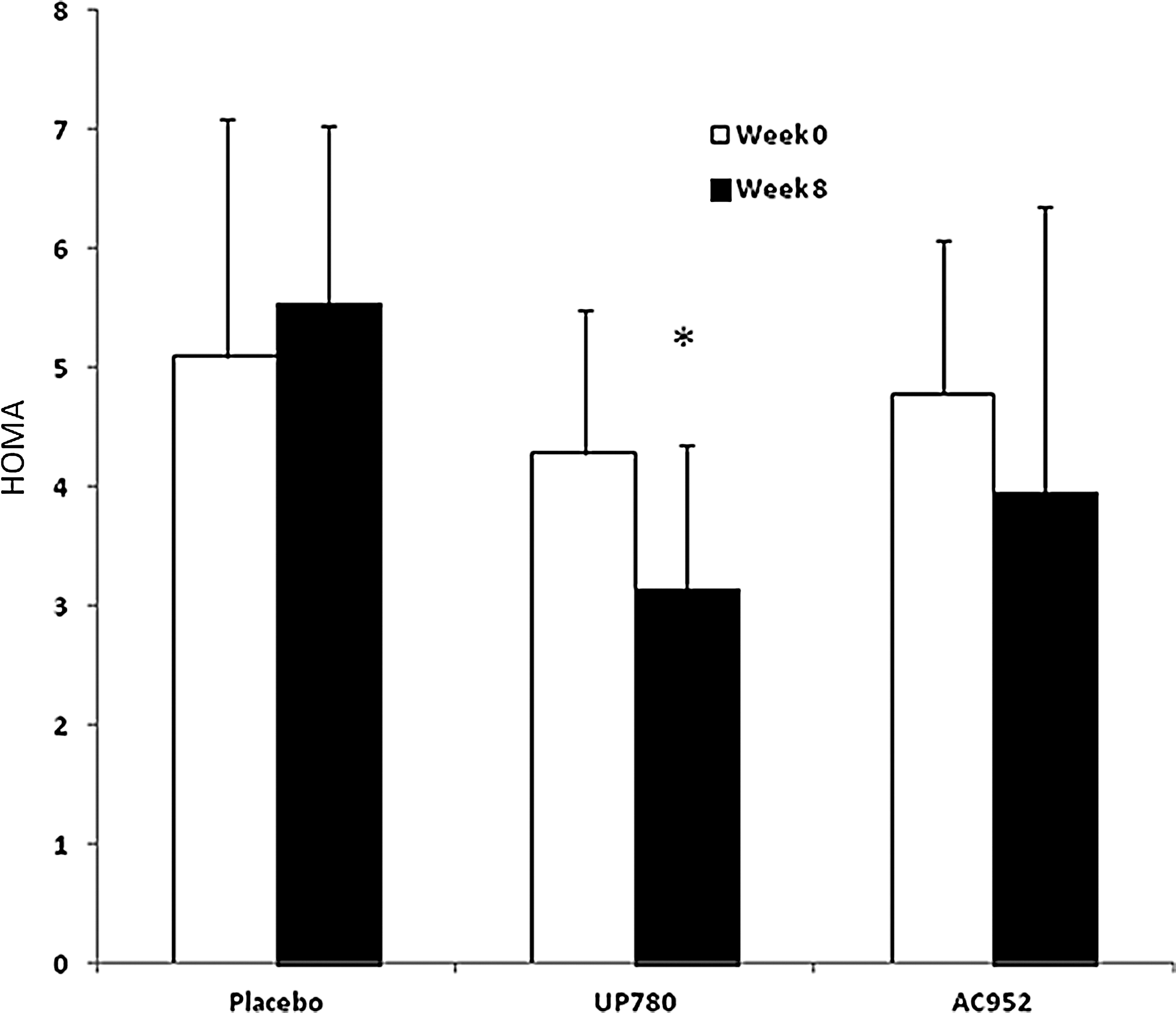
Effect of Aloe vera supplementation on homeostasis model assessment (HOMA). Fasting glucose and insulin levels were measured and HOMA calculated in patients before and after placebo, UP780, or AC952 supplementation. (*) P<0.05 compared to placebo and baseline.
Data are provided as mean±standard deviation (SD).
p<0.02 and ** p<0.05 compared to placebo and baseline.
HbA1c, glycosylated hemoglobin; AUC, area under the curve; Glu-OGTT, glucose tolerance.
Because aloe has been shown to improve oxidative stress in diabetic rats and because oxidative stress can contribute to diabetic complications, we tested the effect of two Aloe vera supplementations on a prototypic biomarker of lipid oxidation, urinary F2-isoprostanes. As seen in Fig. 2, only the UP780 aloe group showed a significant reduction in the F2-isoprostanes; the reduction in the AC952 group was not significantly different compared to placebo.
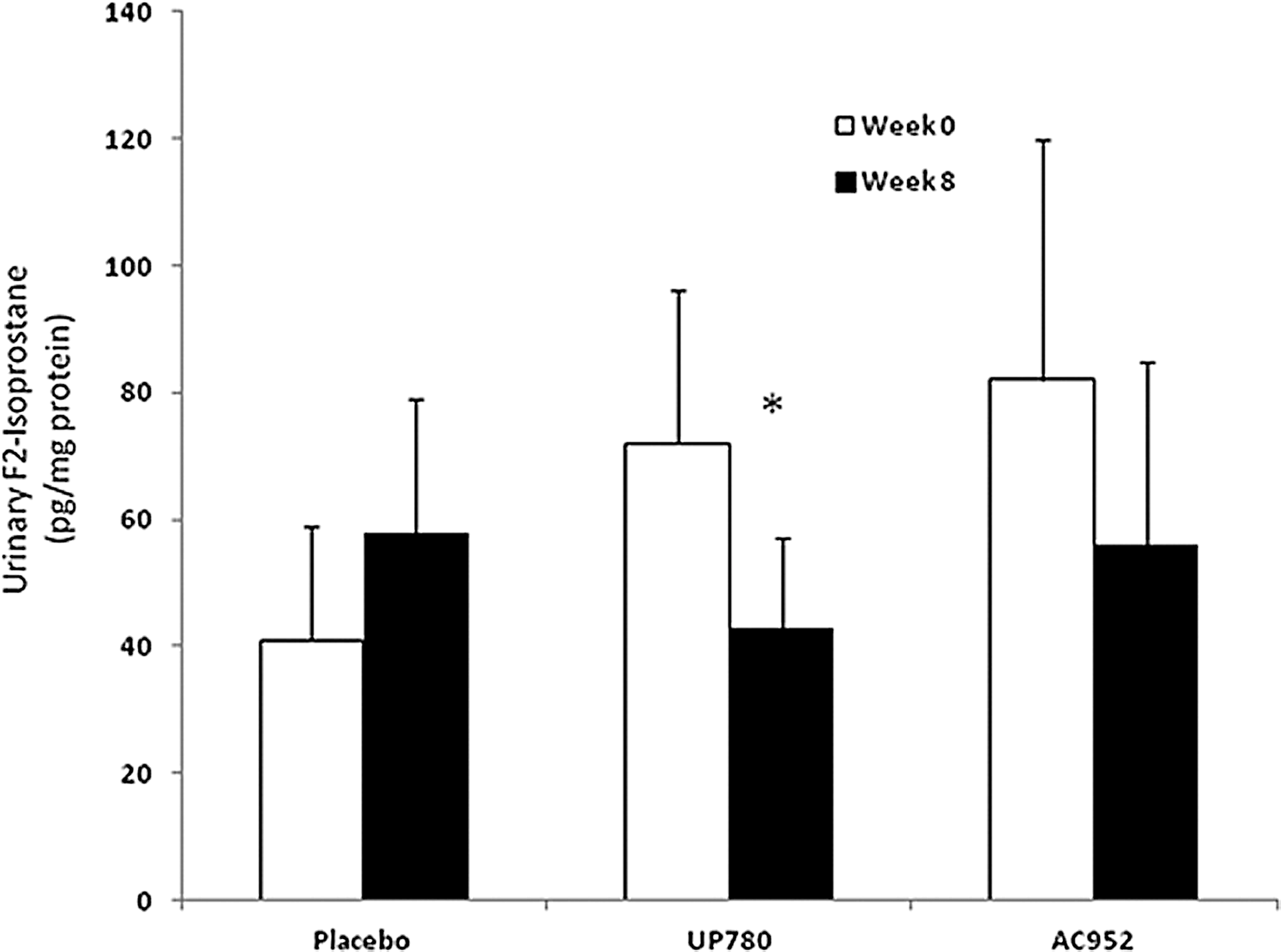
Effect of Aloe vera supplementation on urinary F2-isoprostanes. Urinary F2-isoprstane levels were assessed and normalized to urinary creatinine in patients before and after placebo, UP780, or AC952 supplementation. (*) P<0.05 compared to placebo and baseline.
Discussion
The metabolic syndrome is highly prevalent worldwide and is associated with a greater risk of atherosclerotic cardiovascular disease than any of its individual components and leads to a five-fold increase in diabetes and a two-fold increase in cardiovascular disease. 1 –3 The primary target of treatment of patients with metabolic syndrome is therapeutic lifestyle changes, which are difficult to achieve and, thus, any adjunctive measures to reduce the burden of diabetes and cardiovascular disease in this population are welcome. 1 –3
Numerous animal trials have reported positive effects of Aloe vera in rat models of diabetes; however, there are very few clinical trials in humans. 4 –11 There are several anecdotal reports of antidiabetic activity of aloe in humans, 12,13 but there is a paucity of controlled clinical trials. Thus, in this pilot study, we wished to test the effect of two aloe products in a double-blind, randomized, placebo-controlled study. The results from our pilot study show that among the two aloe supplements, UP780 was more effective in affecting parameters of insulin sensitivity, such as the fasting glucose, fructosamine, HbA1c, HOMA, and insulin. AC952 was effective in lowering LDL-C, fasting blood glucose, and fructosamine. Also, UP780 reduced a marker of whole body oxidation, urinary F2-isoprostanes.
UP780 (aloe product 1) consists of aloe gel fillet powder (the inner gel fillet that remains after removal of the outer rind of the leaf), standardized with 2% aloesin by weight, using aloe chromones and other biologically active components that may be important in maintenance of normal blood glucose levels. Qmatrix or AC 952 (aloe product 2) is aloe gel fillet powder (without aloesin) standardized to a minimum of 10% polysaccharide by weight. It is currently on the market and in use in the finished products of approximately 100 companies, including dietary supplements and other ingestible products; however, its effects have not been previously tested with regard to its antiglycemic effects in a placebo-controlled study.
With regard to hypoglycemic effects, several reports agree with ours with regard to effects in diabetic mice and rat models. 4 –11 There is a single placebo-controlled study in the literature in hyperlipidemic type 2 diabetic patients 14 that showed the benefit of aloe in reducing the burden of diabetes; however, all of the subjects were already on one or two diabetic medications and aloe was given in conjunction with these. Thus, this is the first study showing that even in patients with impaired fasting glucose or impaired glucose tolerance, an 8-week supplementation with Aloe vera gel powder with 2% aloe chromone (UP780) is effective in reducing fasting glucose, fructosamine, HbA1c, and HOMA, a marker of insulin resistance. It is not surprising that UP780 did not lower cholesterol levels, because previous reports regarding hypolipidemic effects of aloe are contradictory. In fact, while acemannan, an active ingredient in the Aloe vera gel, is thought to be responsible for the hypoglycemic effect of aloe, no active ingredient has previously been isolated to explain its hypolipidemic effects.
Oxidative stress plays a critical role in metabolic syndrome and diabetes. 15,16 F2-isoprostanes are biomarkers of whole-body lipid oxidation, which have been shown to be increased in diabetes. 17 We show that UP780 aloe supplementation significantly decreased F2-isoprostanes. In support of our observations, Rajasekaran et al. have previously reported that oral administration of an alcoholic extract of Aloe vera leaf gel at a concentration of 300 mg/kg to diabetic rats, in addition to improving glycemic control, significantly decreased the levels of lipid peroxidation and hydroperoxides in tissues of diabetic rats and also resulted in a significant increase in reduced glutathione, superoxide dismutase, catalase, glutathione peroxidase, and glutathione S-transferase in the liver and kidney of diabetic rats. 18
Because UP780 is a standardized Aloe vera gel preparation, these exciting effects of its hypoglycemic activity as well as lowering of lipid oxidation are promising, especially due to the excellent safety profile and compliance. Thus, such standardized aloe preparations offer an attractive adjunctive strategy to revert the impaired fasting glucose and impaired glucose tolerance observed in conditions of prediabetes/metabolic syndrome and need to be tested in multicenter clinical trials. Future studies will also examine the active ingredient in aloe that is responsible for these effects and examine mechanisms to elucidate these findings.
Footnotes
Acknowledgment
Unigen Inc., AloeCorp., for financial support and aloe products and placebo.
Author Disclosure Statement
S.D received a grant from Unigen and MY, LAB, QJ are employed at Unigen.