
Abstract
Background:
The aim of this study was to determine the ability of glycated hemoglobin (GHb) to predict metabolic syndrome in an Iranian population with normal glucose tolerance (NGT).
Methods:
A cross-sectional study of first-degree relatives (FDRs) of patients with type 2 diabetes was conducted from 2003 to 2005. A total of 1386 FDRs of consecutive patients with type 2 diabetes 30–60 years old (355 men and 1031 women) with NGT were examined. All subjects underwent a standard 75-gram 2-h oral glucose tolerance test and GHb measurement. Consensus criteria in 2009 were used to identify metabolic syndrome. Unadjusted and adjusted multivariate logistic regression analysis was performed to assess the risk of metabolic syndrome. The mean [standard deviation (SD)] age of participants was 42.4 (6.3) years.
Results:
The prevalence of metabolic syndrome was 17.5% in men and 21.5% in women. The multivariate-adjusted odds ratio (95% CI) of metabolic syndrome was 2.01 (1.03, 3.93) for the highest quintile of GHb compared with lowest quintile. These data indicate that GHb was associated with metabolic syndrome, independently of gender among FDRs of patients with type 2 diabetes with NGT.
Conclusions:
These data indicate that GHb below the level for prediabetes might be a predictive measure of metabolic syndrome in FDRs of patients with type 2 diabetes with NGT.
Introduction
While association between GHb level in the nondiabetic persons and metabolic syndrome has been described in a few studies from developed countries, 6 –9 to our knowledge, only one study reported relationship between GHb and metabolic syndrome in the normal glucose tolerance (NGT) range. 10 However, the role of GHb in identifying persons with NGT at risk of metabolic syndrome remains unsettled. The objectives of this study, therefore, were to determine whether higher GHb levels independently predict metabolic syndrome in an Iranian relatives of patients with type 2 diabetes with NGT.
Racial disparities in GHb values and metabolic syndrome exist. 11 –14 The reason for ethnic differences are not clear but can be ascribed to differences in rates of obesity, hypertension, glucose intolerance, and body fat distribution patterns. Comprehensive data for developing countries have not been reported. Therefore, at an ethnological level, the study contributes by characterizing the occurrence of metabolic syndrome in a specific population from central Iran.
Subjects and Methods
Our sample comprised 3176 (818 men and 2358 women) first-degree relatives (FDRs) of a consecutive sample of patients with type 2 diabetes attending clinics in Isfahan Endocrine and Metabolism Research Center affiliated to Isfahan University of Medical Sciences, Iran, between 2003 and 2005. Participants with diabetes mellitus (n=292), impaired glucose tolerance (n=655), impaired fasting glucose (n=581), and those with no GHb measured (n=262) were excluded from the study; 1386 subjects were included in analysis of the distribution of GHb and its association with metabolic syndrome. Pregnant women were excluded (Fig. 1). We used individuals with NGT because prediabetes is one of the risk factors used for the diagnosis of the metabolic syndrome. The study protocol was approved by the Institutional Review Board of Isfahan University of Medical Sciences, Iran, and an informed consent form was signed by each participant.
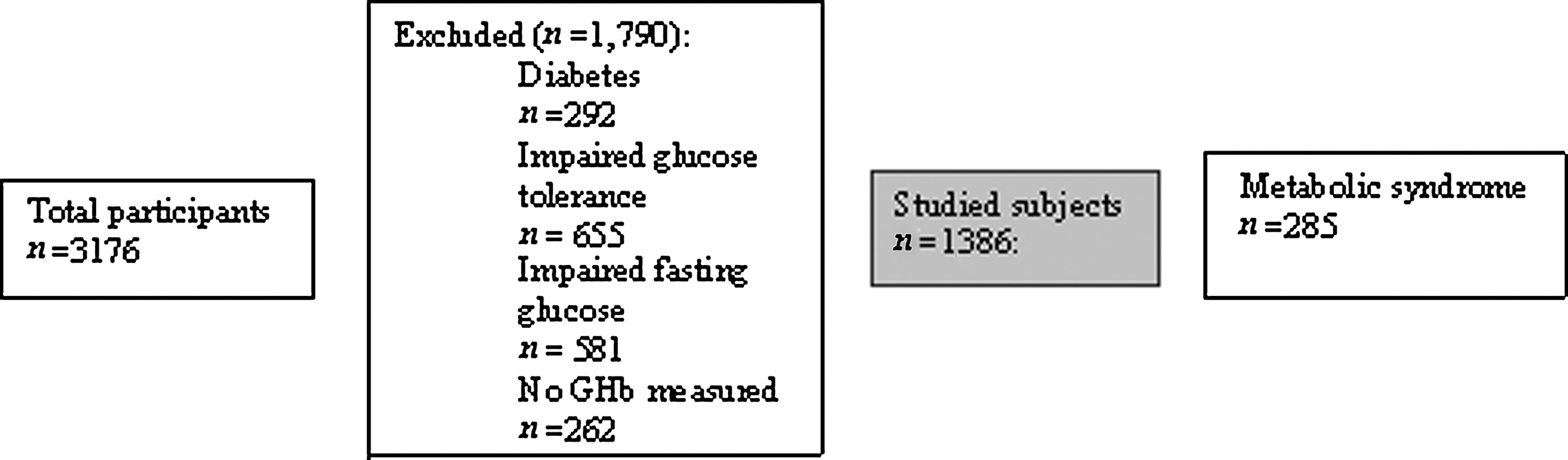
Schematic diagram of the study population.
Procedures
The FDRs of patients with type 2 diabetes included siblings or children 30–60 years old and reported to clinics in the morning after an overnight fast. Subjects were asked to abstain from vigorous exercise in the evening before and in the morning of the investigations. Smokers were encouraged to abstain from smoking in the morning of the investigations. On arrival in the clinic, the information given by the FDRs in the questionnaire on family history was first verified. Then height and weight were measured with subjects in light clothes and without shoes using standard apparatus. Weight was measured to the nearest 0.1 kg on a calibrated beam scale. Height, waist, and hip circumference were measured to the nearest 0.5 cm with a measuring tape. The waist measurement was midway between the lower rib margin and the iliac crest at the end of a gentle expiration. Hip circumference was measured over the greater trochanters directly over the underwear. Body mass index (BMI) (weight/height 2 [kg/m2]) is recognized as the measure of overall obesity. Resting blood pressure (BP) was measured after subjects had been seated for 10 min by using a mercury sphygmomanometer and appropriately sized cuffs, using standard techniques. Those FDRs with fasting plasma glucose (FPG) ≥200 mg/dL were considered as diabetic. If FPG was ≥126 and <200 mg/dL, a second FPG was measured on another day. If the second FPG was also ≥126 mg/dL, participants were considered to be diabetic. Subjects with FPG <126 mg/dL underwent a standard oral glucose tolerance test [OGTT (75 grams of glucose for 2 h)] according to the American Diabetes Association criteria. 15 Venous blood was sampled 0, 30, 60, and 120 min after oral glucose administration. Plasma samples obtained after centrifugation were analyzed the same day.
GHb was measured by ion-exchange high-performance liquid chromatography. The methodology was certified by the National Glycohemoglobin Standardization Program (NGSP). Total cholesterol, triglyceride, high-density lipoprotein cholesterol (HDL-C) (measured using standardized procedures), and low-density lipoprotein cholesterol (LDL-C) (calculated by the Friedewald equation 16 : LDL=(total cholesterol − HDL− triglyceride)/5, for total triglycerides less than 400 mg/dL) were assessed. All the blood-sampling procedures were performed in the central laboratory of the Isfahan Endocrine and Metabolism Research Center using an enzyme-linked method.
Definitions
NGT was defined as having FPG <100 mg/dL and 2-h plasma glucose <140 mg/dL. 15 Cases of metabolic syndrome were identified according to the consensus criteria in 2009, 1 which were the same as the third report of the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III). 14 Metabolic syndrome was considered present when at least three of the following characteristics were observed: Central obesity, defined using ethnic-specific cut points of waist [waist circumference (WC) ≥102 cm in men and ≥88 cm in women]; triglycerides ≥150 mg/dL; HDL <40 mg/dL in men and <50 mg/dL in women; BP ≥130/85 mmHg or on antihypertensive medication, or raised plasma glucose, defined as FPG ≥100 mg/dL or on antidiabetic medication.
Statistical analysis
Analyses were performed using SPSS version 13 for Windows (SPSS Inc., Chicago, IL). Statistical methods used included the Student t-test, chi-squared test, analysis of variance, or Kruskal–Wallis test for normally or nonnormally distributed continuous variables, respectively, and stepwise binary logistic regression. Multiple logistic regressions were carried out to obtain the odds ratio (OR), accompanied by 95% confidence intervals (CI). We considered the following covariates in the multivariate-adjusted analyses: Age, gender, BMI, WC, triglycerides, LDL-C, HDL-C, total cholesterol, and systolic BP (SBP). Adjustment for age and gender were examined in separate models. Multiple linear regression analysis was also done using GHb as the dependent variable. Age-adjusted means were calculated and compared using general linear models. Pearson correlation analysis was carried out to determine the correlation of GHb with cardiovascular risk factors. The ability of GHb to predict the metabolic syndrome was examined by a receiver operating characteristic (ROC) curve and the respective areas under the curve, in which sensitivity was plotted as a function of 1-specificity. An optimal cutoff is the one providing maximum sums of sensitivity and specificity for a given test value from the ROC curve. Analyses were initially stratified by gender, but because the findings were similar, the results are presented for both genders combined to increase statistical power. Study individuals were categorized into quintiles of GHb, and unequal numbers were found in the quintiles because of decimals. All tests for statistical significance were two-tailed; CIs were set at 95%, and P<0.05 was considered significant.
Results
The characteristics of the study participants by quintile of GHb are shown in Table 1. In age-adjusted comparisons of variables, age, plasma glucose at 30 min and 60 min, GHb, LDL-C, BP, and proportion of metabolic syndrome were more likely to increase and HDL-C more likely to decrease across the quintiles of GHb. The mean [standard deviation (SD)] age of participants was 42.0 (6.2) years and 74.0% were women. The mean (range) GHb quintiles were as follows: Quintile 1, 4.0% (<4.4%); quintile 2, 4.6% (4.4%–4.8%); quintile 3, 4.9% (4.8%–5.1%); quintile 4, 5.3% (5.1%–5.6%); and quintile 5, 6.1% (≥5.6%).
Age-adjusted means were calculated using general linear models. Data are express as mean [standard error (SE)] or number (%). P value comparison across all five groups.
LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Characteristics of the 1101 (79.4%) participants without and 285 (20.6%) with metabolic syndrome are shown in Table 2. As expected, those who had metabolic syndrome were older and had higher age-adjusted mean weight, BMI, WC, waist-to-hip ratio, hip circumference, plasma glucose (PG) at 30, 60, and 120 min, triglycerides, and cholesterol, and had lower mean HDL-C and had a higher proportion of obesity. Those who had metabolic syndrome had higher GHb. The age-adjusted mean (SD) GHb was 5.1% (7.8) for those with and 5.0% (8.0.) for those without metabolic syndrome (P<0.01).
Age-adjusted means were calculated using general linear models. The difference in the mean or percentage of the variables between metabolic syndrome and no metabolic syndrome.
P<0.01.
P<0.001.
SE, standard error; CI, confidence interval; SBP, systolic blood pressure; DBP, diastolic blood pressure; GHb, glycated hemoglobin; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol.
Table 3 shows the prevalence of metabolic syndrome by GHb levels. Of the 1386 participants, (355 men and 1031 women), 285 had metabolic syndrome. Overall prevalence of metabolic syndrome was 20.6% (95% CI 18.4, 22.7). Prevalence of metabolic syndrome was higher in women (21.5%; 95% CI 19.2, 23.8) than men (17.5%; 95% CI 13.9, 21.2), but its difference was not statistically significant.
Odds ratios (with 95% CI) calculated by multiple logistic regression. Adjusted for age, gender, body mass index, waist circumference, triglyceride, LDL-C, HDL-C, total cholesterol, and blood pressure.
P<0.05.
P<0.001.
CI, confidence interval; GHb, glycated haemoglobin; OR, odds ratio.
The prevalence of metabolic syndrome increased across the five subject groups. It was 27.3% (95% CI 21.9, 32.6) for participants in the highest quintile of GHb and 16.1% (95% CI 11.6, 20.7) for the lowest quintile. Compared with participants with GHb <4.4% (bottom quintile), the risk of metabolic syndrome was 1.95 times higher in those with GHb ≥5.6% (top quintile) (OR 1.95; 95% CI 1.27, 3.00) in unadjusted models. Controlling for age slightly reduced the OR compared to the unadjusted model. Controlling for age and gender did not alter the relationship between metabolic syndrome compared to the model adjusted for age alone. In a multivariate model, the additional adjustment for other time-dependent covariates increased the relationship between metabolic syndrome compared to the model adjusted for age and gender. In this model, the prevalence of metabolic syndrome was over two times higher among subjects with a GHb ≥5.6% (top quintile) compared to those with GHb <4.4 (bottom quintile).
Compared with individuals with GHb levels less than 4.4% those in the 5.1%–5.6% category were not at significantly greater risk of metabolic syndrome after adjustment for other risk factors. However, those in the 5.1%–5.6% group had a 13% greater risk of metabolic syndrome relative to the individuals in the less than 4.4% group (OR 1.13; 95% CI 0.56, 2.29).
A GHb of ≥5.6% predicted the presence of metabolic syndrome with a sensitivity of 25.3% and specificity of 82.6%. The area under the ROC curves for metabolic syndrome was 0.560 (95% CI 0.523, 0.597) for the GHb (Fig. 2). GHb was a significant predictor for metabolic syndrome (P<0.01).
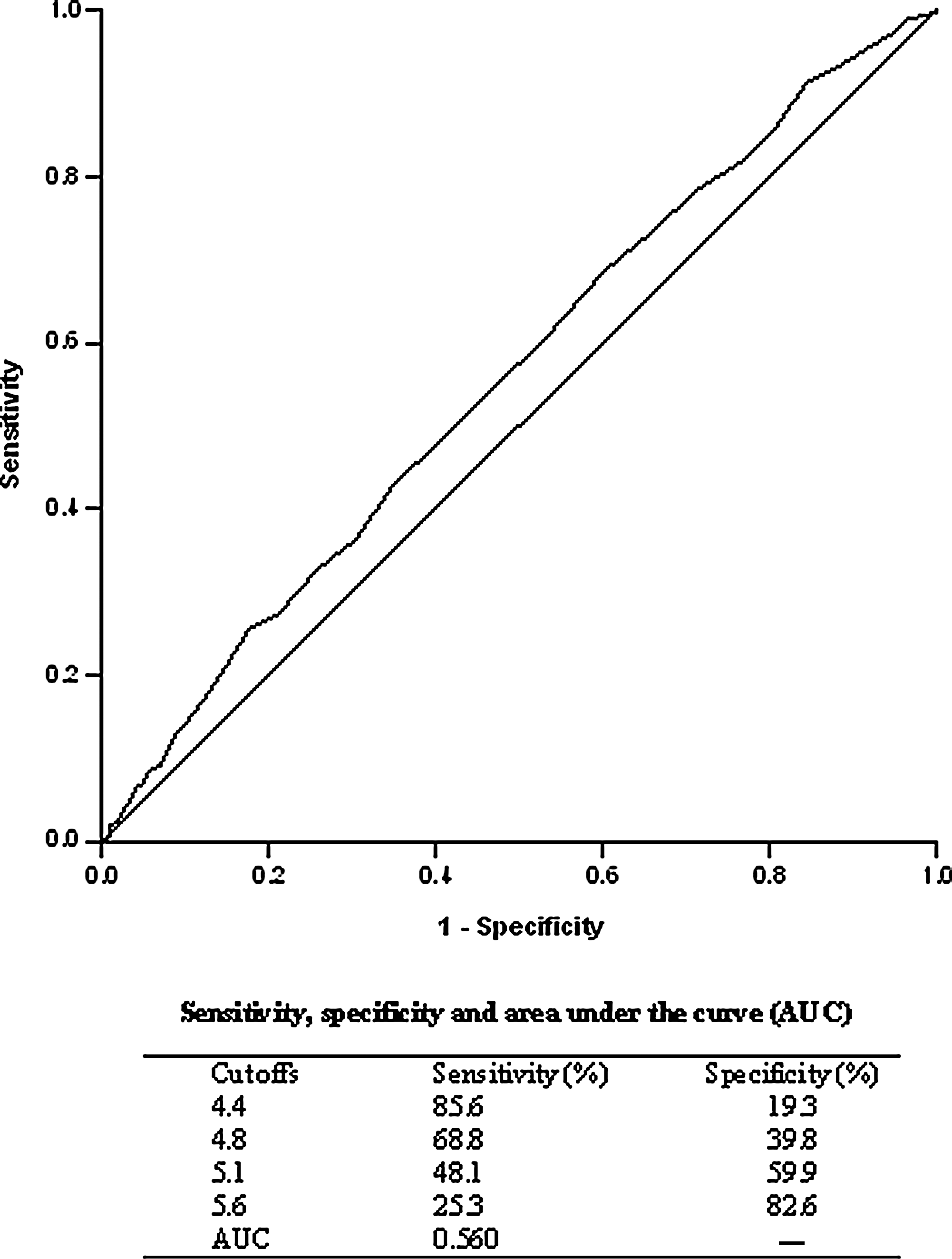
Receiver operating characteristic (ROC) curves for glycated haemoglobin (GHb) for prediction of metabolic syndrome in first-degree relatives of patients with type 2 diabetes with normal glucose tolerance. The estimates of the sensitivity, specificity and area under the ROC curves (AUC) are shown.
GHb was correlated with age (r=0.147, P<0.001), weight (r=0.059, P<0.05), waist circumference (r=0.056, P<0.05), FPG (0.078, P<0.01), PG at 30 min (r=0.105, P<0.001), PG at 60 min (r=0.127, P<0.001), SBP (r=0.107, P<0.001), and diastolic blood pressure (DBP) (r=0.112, P<0.001) and inversely correlated with HDL-C (r=−0.065, P<0.05).
Multiple linear regression analysis revealed that age (β=0.121, P<0.001), FPG (β=0.74, P<0.01), and SBP (β=0.071, P<0.05) had a significant association with GHb.
Discussion
In this cross-sectional study of FDRs of patients with type 2 diabetes with NGT, prevalence of excess (top quintile) GHb level within NGT range was significantly associated with metabolic syndrome. These associations remained significant even after adjusting for a wide range of patient characteristics. A trend in prevalence of metabolic syndrome with an increase in quintile of GHb was observed; however, the difference in prevalence between quintiles did not reach statistical significance, probably because of small number of individuals with metabolic syndrome. Although GHb is not considered to be a diagnostic criterion for metabolic syndrome, it might provide a simple method of predicting metabolic syndrome in a screening program. Furthermore, GHb values ≥5.6% were found to represent an optimal cutoff point for predicting metabolic syndrome in this population.
Although there are many studies that report the utility of GHb in predicting cardiovascular disease and diabetes, there are few that investigate the usefulness of GHb as a predictor of metabolic syndrome, and the present study adds valuable information to the existing literature. In a study by Nguyen et al., 8 prevalence of GHb levels between 6.0 and 6.9 was significantly higher among nondiabetic adults with metabolic syndrome. Sung et al. 9 in a large cross-sectional study of nondiabetic Korean population reported that a GHb of 5.45% was the closest value to the point with ideal sensitivity and specificity for the diagnosis of metabolic syndrome. Osei et al. 7 reported that in 219 healthy nondiabetic, obese, FDRs of African-American patients with type 2 diabetes, the upper tertile of GHb (5.7%–6.4%) reflected some components of metabolic syndrome. Their results suggest that GHb may be a surrogate marker not only of future diabetes, but also of cardiovascular disease. Similarly, Veeranna et al. 6 in nondiabetic participants of the National Health and Nutrition Examination Survey, 1999–2008, reported that a GHb level of ≥5.2% predicted the presence of metabolic syndrome in the population with normal glucose levels. Dilley et al. 10 in a cross-sectional study of Asian Indians population with NGT reported that GHb had a strong association with metabolic syndrome.
Our study results support the conclusion made by Dilley et al. 10 that a GHb level of ≥5.6% had the highest accuracy for predicting metabolic syndrome. Our study reveals that in a population with NGT, GHb levels of ≥5.6% predicted the presence of metabolic syndrome after adjusting for known confounders and effect modifiers, indicating the possibility that identification of metabolic syndrome by GHb is not entirely due to FPG. GHb and FPG may each represent the measurement of a different physiological process, with an elevated GHb representing an increased glycation rate or elevated postprandial glucose levels, whereas FPG levels are dependent on hepatic glucose production. 15 Our findings support the conclusion made by a few other studies 6,7,9 that an elevated GHb level of ≥5.6% can be considered as a marker for metabolic syndrome. This cutoff level is slightly lower than the recommended level used for classification of a person as prediabetic (GHb level of 5.7%–6.4%), indicating that an active search for screening metabolic syndrome should be performed, even at GHb levels below 5.7%.
Our study sample was addressed to individuals at increased risk of metabolic syndrome, cardiovascular disease, and type 2 diabetes, because they had FDRs with the disease and this might be explained by the differences in levels of other risk factors. This group of individuals will only increase further over time because the prevalence of diabetes and metabolic syndrome is expected to increase worldwide. Different studies have found that the incidence and prevalence of metabolic syndrome, cardiovascular disease, and type 2 diabetes are greater in those persons who have a family history of the disease. 17 –23
Our study has strengths and limitations. The strengths include a sample consisting of both men and women of a wide age range, simultaneous assessment of plasma glucose during a standard OGTT and GHb, and information on cardiometabolic risk factors. More importantly, to the best of our knowledge, the present study is the first in high-risk NGT individuals to examine the relationship between GHb as a predictor of metabolic syndrome in the Middle East. The present study also has some limitations. Most notably, the cross-sectional and observational nature of our study did not provide insight into the time course of the development of metabolic syndrome; therefore, no conclusions regarding the cause–effect relation or pathophysiological mechanisms can be made. In addition, the present findings were derived only from a specific population from central Iran, and the results could vary as a function of ethnic group. Previous studies have shown that racial disparities in GHb values and metabolic syndrome exist. 11 –14
Whether our findings could be extrapolated to NGT subjects who are not genetically predisposed to diabetes or to other racial and ethnic populations remains to be elucidated. Even though the study included 1386 participants who were thoroughly examined and the study was sufficiently powered to give statistically significant results, the sample size of quintiles with metabolic syndrome was comparatively small. Due to the still-conflicting results in assessing metabolic syndrome prediction, a long-term follow-up in a large cohort could therefore contribute further to a clarification of the question. Furthermore, the advantages of the GHb test are that it can be measured at any time of the day. The disadvantages are that GHb cannot be measured in the presence of hemoglobin variants by several methods and the difficulty in standardization. 24 Finally, the study included only individuals with NGT, thus excluding from the analysis those at high risk of the metabolic syndrome.
In conclusion, these data provides further evidence that GHb might be a predictive measure of metabolic syndrome in FDRs of patients with type 2 diabetes, even among individuals with NGT. Our study results support the conclusions made by others 6,7,9 that, apart from serving as a screening tool for prediabetes and diabetes, GHb level can be considered as a screening tool for metabolic syndrome. Further cohort studies are needed to better understand the role of GHb on metabolic syndrome.
Footnotes
Acknowledgments
This work was supported by grants from the Isfahan Endocrine and Metabolism Research Center, Iran. The authors are grateful to Mr. Majid Abyar for computer technical assistance.
Author Disclosure Statement
No competing financial interests exist. M. Janghorbani conceived and designed the study, analyzed the data, and wrote the manuscript. M. Amini recruited samples and contributed to discussion and revision of the manuscript, and obtained funding for the Isfahan Diabetes Prevention Study.