
Abstract
Background:
Metabolic syndrome is a cluster of risk factors leading to cardiometabolic diseases. The association between metabolic syndrome and cardiovascular disease (CVD) has been evaluated previously, but none of those studies looked at cardiac autonomic functions in these patients. The aim of the present study was to investigate the effect of metabolic syndrome on heart rate turbulence, which plays an important role in the development of CVD.
Methods:
Thirty-seven patients (17 females and 20 males) were included in the metabolic syndrome group and 37 subjects (19 females and 18 males) were included in the control group. Heart rate turbulence (HRT) indices [turbulence onset (TO) and turbulence slope (TS)] were calculated from 24-hr ambulatory electocardiographic recordings.
Results:
At least one of the TO or TS values were within the abnormal range in 62% of the patients within the metabolic syndrome group. In the control group, at least one of the TO or TS values were within the abnormal range in 27% of the subjects.
Conclusions:
Our study results indicate that cardiac autonomic function is impaired even in the absence of overt cardiac disease in patients with metabolic syndrome. Further studies are needed to elucidate the prognostic significance and clinical implications of impaired autonomic functions in patients with metabolic syndrome.
Introduction
Heart rate turbulence (HRT) is defined as a physiologic alteration in the sinus rate after a ventricular premature beat and is considered to be an indicator of baroreflex sensitivity. 4 The European Heart Society has accepted HRT as a marker of cardiac autonomic regulation and represents a measure of vagal activity. 5 The relationship between metabolic syndrome and HRT indices has not been evaluated yet. Therefore, the aim of the present study was to investigate the effect of metabolic syndrome on HRT, which plays an important role in the development of CVD.
Materials and Methods
Study population
Thirty-seven patients (mean age, 47±9 years; 17 females and 20 males) were included in the metabolic syndrome group and 37 subjects (mean age, 49±7 years; 19 females and 18 males) were included in the control group. Detailed clinical histories were obtained from all the subjects. The age, gender, height, body weight, and waist circumference measurements of all the subjects, as well as the presence of cardiovascular risk factors (hypertension, hyperlipidemia, obesity, and smoking anamnesis), were recorded. In addition, fasting blood glucose, total cholesterol, triglycerides, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), blood urine nitrogen, creatinine, and thyroid-stimulating hormone (TSH) levels were measured. According to the criteria of 2001National Cholesterol Education Program Adult Treatment Panel (NCEP ATP III), the presence of any three of the following five traits—low levels of HDL-C (<40 mg/dL in men and <50 mg/dL in women), elevated blood pressure (≥130/85 mmHg or drug treatment for hypertension), abdominal obesity (waist circumference in men ≥102 cm, in women ≥88 cm), high levels of triglycerides (≥150 mg/dL or drug treatment for elevated triglycerides), and high levels of fasting blood glucose (≥100 mg/dL or drug treatment for elevated blood glucose)—was considered to be metabolic syndrome. One point was given for the presence of each metabolic syndrome criterion, and the total score was calculated as the metabolic syndrome score. Twelve-lead electrocardiographies of the all patients were obtained. The control group was composed of healthy volunteers. All of the subjects had echocardiography via the transthoracic approach (Vingmed Vivid 7 pro device, 3.5 MHz probe) and a treadmill exercise test (Quinton model Q4500).
Patients who had a history of myocardial infarction or ischemic electrocardiogram (ECG) changes, as well as patients with heart failure, significant hemodynamic valvular disease, and regional wall motion impairment were excluded from the study. Additionally, patients who had the following conditions were excluded from the study: Patients with a permanent cardiac pacemaker, patients with a rhythm different from sinus rhythm, patients who had a treadmill test for detecting silent ischemia and were evaluated as positive or suspicious, patients under medication that may affect autonomic balance, and patients with a systemic disease, such as renal failure, thyroid function impairment, and overt diabetes mellitus.
Calculation of heart rate turbulence
All of the subjects were monitored for 24 hr via an ECG Holter system (ELA Spiderview Digital Recorder). Records were transferred to the computer and first analyzed by the Holter program (ELA system), and the calculated mean heart rates were recorded. Because the reliability of the measurements obtained from a single ventricular ectopic beat (VEB) is questionable due to sinus arrhythmia and the artifacts, the mean of an at least five VEB measurements was taken to obtain an accurate measurement of HRT. Recordings were examined visually, and the regions with artifact were excluded from the analysis. The two HRT parameters, turbulence onset (TO), and turbulence slope (TS) were calculated automatically from the Holter records via the HRT View Version 0.60-0.1 software program. TO was calculated according to the following formula: TO (%)=(RR1+RR2)−(RR-2+RR-1)/(RR-2+RR-1)×100. TO was defined as “the percentage of the expression of the ratio of the difference between the first two sinus RR intervals subsequent to VEB (RR1+RR2) and the last two sinus RR intervals prior to VEB (RR-1+RR-2) to the last two sinus RR intervals prior to VEB (RR-1+RR-2)”. TS was defined as “the highest positive value among the regression slopes of the consequent five RR intervals within the first 20 sinus RR intervals following VEB.” The normal values accepted were the values lower than 0% for TO and values higher than 2.5 msec/RR for TS. Turbulence loss was accepted as the enhancement in turbulence onset and the reduction in turbulence slope. 4,6,7
Statistical analyses
SPSS (Statistical Package for the Social Sciences, v. 16.0; SPSS Inc, Chicago, IL) was used for statistical analyses of the cases. Numeric variables were expressed as the mean±standard deviation. For comparison of the means between the groups and for the variables with a normal distribution, the Student t-test was used, and the Mann–Whitney U test was used for the variables without a normal distribution. The categorical variables were compared via a chi-squared test. Pearson correlation analysis was used for the evaluation of the relationship between the variables. A P value <0.05 was considered as statistically significant in all of the statistical analyses.
Results
There was no statistically significant difference between the metabolic syndrome and control groups regarding age, gender, and the mean heart rates. Although left ventricular hypertrophy was high in the metabolic syndrome group, the difference was not statistically significant. The demographic characteristics of both groups and the distribution of parameters according to the groups are presented in (Table 1).
BMI, body mass index; HDL, high-density lipoprotein; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, fasting blood glucose; LVDD, left ventricular diastolic dysfunction; LVH, left ventricular hypertrophy; mean HR, mean heart rate.
Body mass index (BMI), hypertension, HDL, triglycerides, systolic and diastolic arterial blood pressures, fasting blood glucose levels, left ventricular diastolic dysfunction, and the metabolic syndrome score were significantly higher in the metabolic syndrome group as expected (Table 1).
At least one of the TO or TS values were within the abnormal range in 62% of the patients within the metabolic syndrome group. In the control group, at least one of the TO or TS values were within the abnormal range in 27% of the subjects.
When the metabolic syndrome and control groups were divided into subgroups according to the HRT parameters being normal or abnormal, a significant difference was determined between the subgroups (Fig. 1). When the onset of turbulence and the turbulence slope parameters were considered separately; the TO was determined to have more abnormal values in the metabolic syndrome group, which was statistically significant (P<0.05).
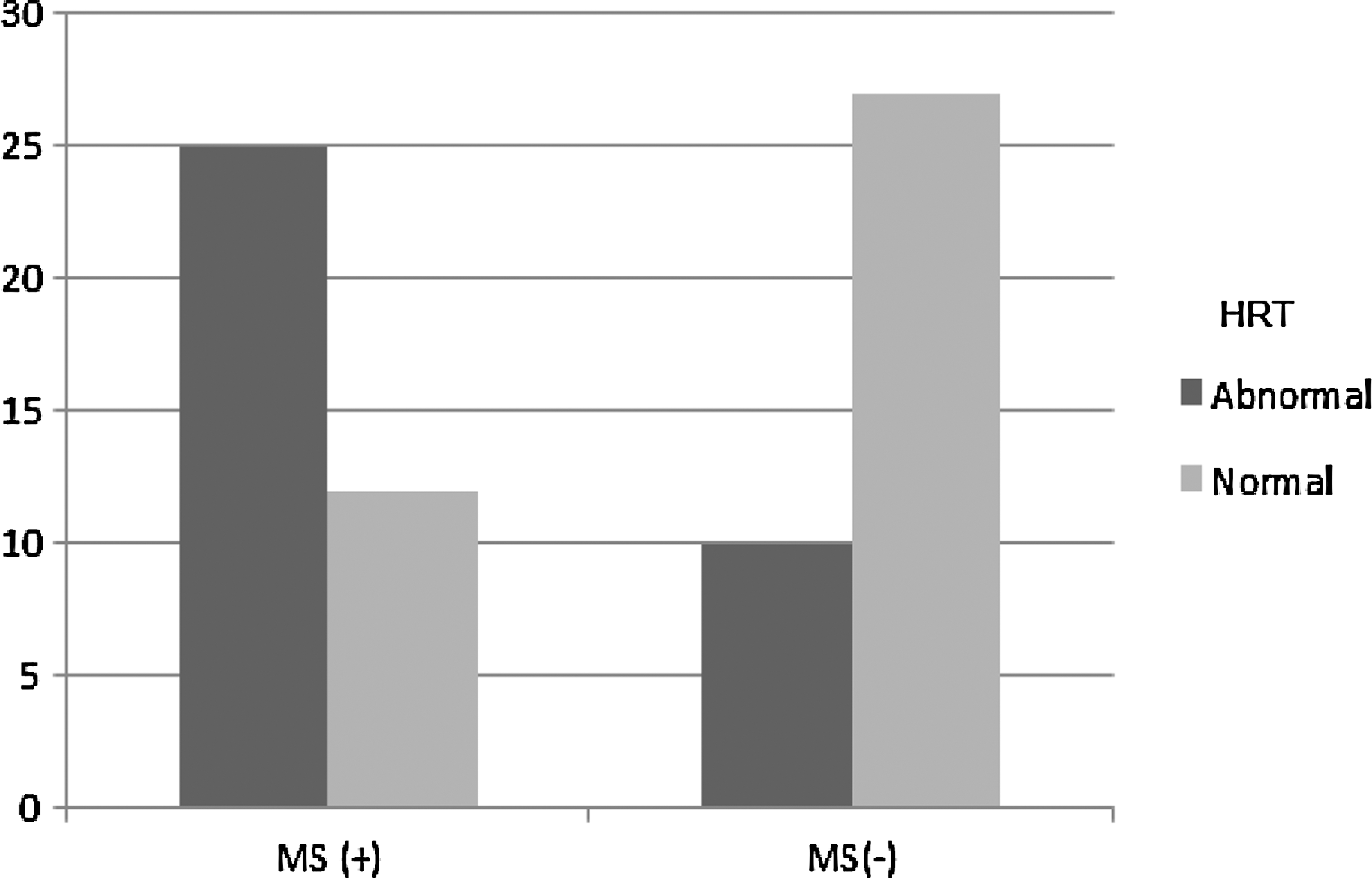
The distribution of the heart rate turbulence parameters in patients with and without metabolic syndrome. HRT, heart rate turbulence; MS, metabolic syndrome.
When the mean of the HRT parameters was examined, the TS value was significantly lower and the TO value was significantly higher in the metabolic syndrome group (Table 2). In subgroup analyses, no statistically significant correlation was determined between hypertension, left ventricular hypertrophy, and the TO and TS values (Table 3). When the relationship between age and HRT parameters was examined in the metabolic syndrome group, no significant correlation was determined. Additionally, no significant correlation was determined between the BMI and the HRT parameters.
TO, turbulence onset; TS, turbulence slope; LVH, left ventricular hypertrophy; HT, hypertension.
Discussion
To the best of our knowledge, our study is the first to evaluate the relationship between metabolic syndrome and HRT indices. We have found that there was a significant reduction in the TS values and a significant enhancement in the TO values in the metabolic syndrome group.
People with metabolic syndrome are faced with an increased risk of CVD and mortality due to all causes. In the clinical studies, it has been shown that, the early and effective control of these risk factors reduces the risk of CVD. 3,8 –10
HRT is considered to be a good indicator for vagal activity 5 and also appears to be sensitive to autonomic dysfunction, especially to impaired baroreflex function. 11,12 HRT reveals the alterations in the cardiac autonomic functions in diseases such as diabetes mellitus and hypothyroidism 13,14 and predicts a higher risk of fatal or near-fatal arrhythmic events after acute myocardial infarction. 5,15
There are studies in the literature investigating the relationship between each component of the metabolic syndrome and HRT 13,16 –18 ; however, there is no study in the literature investigating how metabolic syndrome affects HRT and related factors during the interaction. The present study gains importance because it is the first such study in this field.
In a study performed on patients with essential hypertension, the TO value was shown to be significantly higher and the TS value was shown to be significantly lower in hypertensive patients with left ventricular hypertrophy compared to those without left ventricular hypertrophy. This study has demonstrated that HRT, and consequently the baroreflex sensitivity, was impaired in hypertension which developed left ventricular hypertrophy. 16
In the present study, no significant difference was shown regarding the mean values of the HRT parameters in the subgroup analysis of patients with and without hypertension. The reason for this may be the development of left ventricular hypertrophy in only 5 (13.5%) of the hypertensive patients and no development of target organ damage in the majority of the patient population.
In a study in which the effect of obesity on HRT parameters was investigated, no change in HRT parameters was observed in obese patients without co-morbidities.
17
In addition, in a subgroup analysis of another study, in which HRT after myocardial infarction was investigated, it was demonstrated that obesity did not affect the change in HRT parameters.
18
In agreement with the above-mentioned studies, in the present study no significant correlation was shown among BMI, waist circumference, and the change in HRT parameters. Independent from the separate effects of the metabolic syndrome components, it was shown that the cumulative effect of metabolic syndrome significantly decreased the TS and significantly increased the TO, which then caused a distinct impairment in HRT. Therefore
It is known that HRT is affected by factors such as ischemia, age, and the mean heart rate. Patients with ischemic symptoms were not included in the present study. It has been reported that HRT decreases with age. 12 Because the patient population in our study was comprised of young patients, an impairment in HRT in the metabolic syndrome group corroborated the cumulative effect of metabolic syndrome, independent of the age factor. In addition, in several studies, it has been reported that there is an association between the elevated heart rate independent of CVD and both HRT parameters and sudden cardiac death. 12,19 –22 The mean heart rate values determined by Holter monitoring in our study were within the normal range and similar in patients with metabolic syndrome and the control group. This supports the findings presented herein, suggesting that impairment in HRT is independent from an increase in the heart rate and is a result of metabolic syndrome.
In conclusion, in metabolic syndrome patients with no cardiovascular target organ damage, such as coronary artery disease and left ventricular hypertrophy, impairment in HRT was observed. This result gave rise to the notion that in metabolic syndrome, which plays a role in the pathophysiology of the complex endocrine and inflammatory multifactorial mechanisms, cardiac autonomic function is impaired. Thus, baroreflex sensitivity was impaired and this impairment developed prior to cardiovascular target organ damage. Risk factors should be carefully reduced to prevent metabolic syndrome, which has been remarkably increasing worldwide.
Footnotes
Author Disclosure Statement
The authors had no conflicts of interest to declare in relation to this article.