
Abstract
Background:
High blood concentrations of inflammatory markers, including white blood cell (WBC) count, are closely related to the metabolic syndrome. Both conditions predict dismal survival. We determined prospective associations between mortality and factors derived by a factor analysis of WBC count and the basic components of the metabolic syndrome.
Methods and Results:
We performed a factor analysis of WBC count and the continuous components of the metabolic syndrome in 196 men and 200 women, comprising 64% of the originally invited 75 year olds from the Swedish city Västerås. The analysis revealed three factors in men and two in women. The first factor included fasting glucose, high-density lipoprotein cholesterol, triglycerides, and waist circumference in men and in addition WBC count in women. The second factor included diastolic blood pressure and systolic blood pressure in both sexes. In men, the third factor included fasting glucose and WBC count. These factors explained 66% (first factor, 28%; second factor, 23%; third factor, 15%) of the variation in men and 57% (first factor, 34%; second factor, 23%) in women. Prospective associations of the derived factors and all-cause mortality during 10-year follow-up were assessed by Cox regression [hazard ratio (HR)]. The first factor was significantly related to increased mortality in men: HR=1.22 [95% confidence interval (CI) 1.05–1.41; p=0.008] and women: HR=1.25 (95% CI 1.06–1.48; p=0.010). Pooling men and women adjusting for established cardiovascular risk factors gave HR=1.16 (95% CI 1.04–1.29; p=0.010). In men the third factor was significantly related to mortality; HR=1.29 (95% CI 1.07–1.57; p=0.009).
Conclusions:
A metabolic inflammatory factor and a blood pressure factor were identified. In men, the former was split into a metabolic and an inflammatory factor. Factors including metabolic and inflammatory components were significantly related to 10-year mortality and the relation remained after adjusting for established cardiovascular risk factors.
Introduction
Factor analysis has been used to understand the pattern of clustering of the basic variables of the metabolic syndrome. By definition, factor analysis implies a multivariate correlation method aiming to explain the relation between a set of variables (in this case the individual continuous components of the metabolic syndrome) and smaller sets of underlying variables (=factors) of potential etiological importance. By applying factor analysis to the individual components of the metabolic syndrome among 75 year olds in a community-based sample two factors were revealed. 3 These factors were: (1) A metabolic factor (FPG, HDL-C, TG, and WC) and (2) a blood pressure factor (SBP and DBP). The clustering between the component variables of the metabolic factor was stronger among women than among men. This sex disparity pattern was also evident by a stronger correlation among women between FPG and a set of components comprising HDL-C, TG, and WC. Furthermore, the metabolic factor was related to a decreased 10-year survival. 3
A close relation between markers of inflammatory processes and the metabolic syndrome has been demonstrated. 4 –14 Increased blood concentration of markers of inflammation, including the WBC count, indicates high mortality and cardiovascular morbidity. 8,15,16 High-sensitivity C-reactive protein (hsCRP) is the most commonly used marker of inflammatory processes: Concentrations in the top third of the population are associated with an increased risk of approximately 50% for a first future coronary and stroke events. 6,9 In postmenopausal women, the top quarter of the WBC count, another marker of the inflammatory process, is associated with an approximate 50% increase in the risk of myocardial infarction, stroke, and all-cause mortality. 16
Previously, we have reported 10 a strong relation among women between the WBC count and some component variables of the metabolic syndrome (FPG, HDL-C, TG, and WC) within 75 year olds in a community-based cohort. The purpose of the present study was to extend the factor analysis mentioned earlier by introducing the WBC count as an additional component and further to study the relation to 10-year mortality of the factors derived by the extended factor analysis.
Methods
Study population
The city of Västerås (130,000 inhabitants) situated in central Sweden has a population that is socioeconomically representative of the country. In 1997 a random sample of 618 of the 1100 inhabitants born in 1922 (i.e., 75 years old) were invited to a cardiovascular health survey. The final number of participants was 432 (70% of those invited; women=222; men=210). Reasons for nonparticipation were: Unknown (n=46), never reached (n=29), unwilling due to diseases under treatment (n=54), language or logistical problems (n=27), locomotive impairment (n=28), or died before examination (n=2).
Due to missing values in some of the clinical variables, the examined cohort finally comprised 196 men and 200 women (64% of the originally invited individuals). The study was approved by the research ethics committee at Uppsala University, Sweden.
Baseline examinations
WC was measured in the horizontal plane at the midpoint between the lowest rib and the iliac crest. Blood pressure was measured with a mercury sphygmomanometer and rounded to the nearest 5 mmHg, with the subjects in a supine position and having rested for 5 min, which was the clinical practice in Sweden at that time. Diagnosis of diabetes, previous myocardial infarction, and stroke was based on self-reported history of disease verified by medical records. Hypertension was defined as self-reported physician-diagnosed high blood pressure in combination with regular antihypertensive treatment.
Fasting (≥10 hr) blood samples were collected for biochemical analysis. The WBC was counted with an automated blood cell counter (Cell-Dyn 3500, Abbott). Serum TG and HDL-C were determined enzymatically using an automated analyzer system (Hitachi 717, Boehringer Mannheim, Mannheim, Germany). Low-density lipoprotein cholesterol (LDL-C) was calculated using the Friedewald formula: LDL-C=Total cholesterol − (TG/2.2+HDL-C) if TG ≤ 4.0 mmol/L, else LDL-C is undefined. The blood glucose samples were treated with a hemolytic reagent (Merck Diagnostica, Darmstadt, Germany), and glucose was determined enzymatically with glucose dehydrogenase using a Cobas Mira analyzer (Roche Diagnostics Ltd, Rotkreuz, Switzerland). Plasma glucose was computed from venous whole blood glucose using the formula: Plasma glucose=0.558+1.119 * Whole blood glucose. 17 Newly detected diabetes was defined as fasting plasma glucose≥7.0 mmol/L without known diabetes.
Body weight and height were measured and body mass index (BMI) calculated as (weight in kg)/(height in m) 2 . The metabolic syndrome was defined according to the NCEP Adult Treatment Panel III (ATP III) criteria. 18
Follow up
Follow up started at the date of the index examination in 1997. The participants were followed until death or to December 31, 2007. The follow-up survival status was based on the Swedish Death Register, and causes of death were taken from the Swedish Cause of Death Register. Assessment of follow-up survival status was complete in all participants.
Statistical methods
Continuous variables were summarized by median and quartiles and categorical variables by counts and proportions. For continuous variables the Wilcoxon Mann–Whitney rank sum test was used to compare groups. Categorical variables were compared using the Fisher exact test.
Associations between the WBC count and the individual components of metabolic syndrome (FPG, HDL-C, TG, WC, and SPB/DBP) were assessed by the Pearson product-moment correlation. Sex differences in the associations were analyzed by linear regressions using the WBC count as the dependent variable. The individual component under consideration, sex, and their interaction term comprised the independent variables. To make the positively skewed variables WBC count, FPG, and TG more symmetric, they were logarithmically transformed before the correlation and regression analyses
The factor analysis included the WBC count and the individual variables of metabolic syndrome (FPG, HDL-C, TG, WC, DBP, and SBP). Skewed variables (FPG, TG, and WBC count) were logarithmically transformed prior to the factor analysis. To simplify the interpretation, HDL-C was inverted (HDL-C−1) prior to the factor analysis because high levels are protective as opposed to the other variables of the metabolic syndrome.
Principal component analysis (PCA) within each sex strata was used to identify an initial set of uncorrelated factors. Because the variables were measured in different units, the PCA was run on the correlation matrix, thereby giving each individual variable the same weight. As a result the sum of the eigenvalues, λ i, equals the number of variables. We applied the Kaiser–Guttman method, which implies that factors with λ i >1 are retained because they summarize more information than any single variable. However, a PCA of randomly generated uncorrelated variables will produce λ i >1 due to random fluctuation. Therefore, we applied nonparametric bootstrap. Individuals were resampled with replacement to assess the variability of the eigenvalues and construct CI. The percentile method, which takes the central (1–2α) part of the bootstrap distribution as an approximate (1–2α)100% CI, was applied. The number of bootstrap replicates, B, was set to 10,000.
To facilitate the interpretation of the selected factors, the varimax (orthogonal) rotation was used. This has as its rationale the provision of uncorrelated factors with a few large loadings and as many near-zero loadings as possible. Cutoff for factor loadings was set at 0.3. The factor loadings are the correlations between the original variables and the factors.
Nonparametric bootstrap (resampling individuals) was used to assess the consistency and accuracy of the factor analysis. Complications in this context are: (1) Factor loadings are not uniquely defined because the sign of the loadings is arbitrary (i.e., the loadings for a factor can be multiplied by −1 without affecting the model estimates); (2) the order of the factors can change from one bootstrap sample to another, i.e., the factor connected to the largest eigenvalue will not be the same over all bootstrap replicates. As a consequence, the factor loading estimates will not be smooth functions of the sample. A small perturbation of the sample can lead to a large change in the factor-loading estimates. Instead of applying the traditional Procrustes rotation 19 to overcome this, we prefer to optimally reflect varimax-rotated factor loadings and use the number of times the factor order differs from the one in the original sample as a measure of the stability of the factor loadings. This means that for each bootstrap sample we perform a varimax rotation and then reflect the solution so that the factor loadings have the same sign as the loadings of the original sample. When constructing confidence intervals based on, e.g., the percentile method using the central (1–2α) part of the bootstrap distribution of the factor loading estimates, only bootstrap samples with the same factor order as the original sample will be used; otherwise, large jumps can severely influence the length of the CI. Factor scores for each subject were computed using median factor loadings above the cutoff 0.3, i.e., median factor loadings below 0.3 were set to 0.
Crude and adjusted prospective associations between all-cause mortality and the factors derived from the factor analysis were analyzed using Cox proportional hazards regression (PHREG) with and without stratification by sex. A best subset approach, using the Akaike information criterion defined as AIC=−2max
θ
{log[L(θ|
The predictive ability of the original component variables of the metabolic syndrome, WBC count, and the derived factors was assessed by AIC and the time-dependent area under the receiver operating characteristic (ROC) curve, AUC t =P[ Zi >Zj |Di (t)=1, Dj (t)=0 ], where Zi and Zj are independent predicted risk scores, under the Cox PHREG model, for subjects i and j and D.(t)=0/1 is an indicator variable indicating whether an event has occurred by a specific time t. 20
The proportional hazard assumption was assessed by visual inspection of the log[−log(cumulative survival)] for each variable, continuous variables being categorized into tertiles. Cumulative survival was estimated by the Kaplan–Meier estimator.
A two-sided p value<0.05 was regarded as statistically significant. The SPSS statistical package, version 18.0, was used for descriptive analyses including pairwise comparisons, correlation, and regression analyses. Minitab version 15.0 was used for the bootstrapped factor analyses and SAS version 9.2 was used for the Cox PHREG analyses and calculations of the time-dependent area under the ROC curve.
Results
Cross-sectional findings
Table 1 presents baseline characteristics of the study population stratified by sex. Notably, the metabolic syndrome was significantly more common in women. As expected, previous myocardial infarction and known cardiovascular disease were significantly more common in men. There were no differences in the prevalence of other metabolic syndrome–related diseases. Only 12 subjects, 6 men and 6 women, were on statin treatment.
Data are expressed as median (interquartile range) and counts (%).
The body mass index is the weight in kilograms divided by the square of the height in m. To convert the values for glucose to mg/dL divide by 0.0555. To convert the values for cholesterol to mg/dL divide by 0.0259. To convert the values for triglycerides to mg/dL, divide by 0.0113.
Data on LDL-C were missing in 11 men and 8 women.
High blood pressure is defined as SBP≥140 mmHg or DBP≥90 mmHg without known hypertension.
Newly detected diabetes is defined as fasting plasma glucose≥7.0 mmol/L without known diabetes.
HDL-C, high-density lipoprotein cholesterol; NA, not applicable; DBP, diastolic blood pressure; SBP, systolic blood pressure; WBC, white blood cells; LDL-C, low-density lipoprotein cholesterol; TIA, transient ischemic attack; NCEP ATP III, National Cholesterol Education Program Adult Treatment Panel III.
Pearson correlations of log(WBC) and the individual components of the metabolic syndrome stratified by sex are given in Table 2. The correlations between log(WBC) and log(FPG), HDL-C−1, log(TG), and WC were significant in women but not in men. A weak correlation between log(WBC) and SBP was found in men. Using regression analysis including interaction terms, we found a significant sex difference in the strength of the association between log(WBC) and log(FPG), and between log(WBC) and HDL-C−1.
Data are expressed as correlation; p value.
FPG, fasting plasma glucose; HDL, high-density lipoprotein; TG, triglycerides; WBC, white blood cell; DBP, diastolic blood pressure; SBP, systolic blood pressure.
Bootstrapped principal component analysis including the WBC count and the individual variables of the metabolic syndrome identified three factors in men and two in women applying the Kaiser–Guttman method (see Fig. 1). The three factors in men explained (95% CI within brackets) 66% (63%–70%) of the total variation [first factor 28% (25%–32%), second factor 23% (20%–25%), and third factor 15% (14%–17%)] and the two factors in women 57% (53%–61%) of the total variation [first factor 34% (30%–37%) and second factor 23% (21%–25%)].

Scree plot presented as box plots from 10,000 bootstrap samples.
After varimax rotation and optimal reflection (see Fig. 2 for bootstrap clouds of the factor loadings), the first, second, and third factors in men were interpreted as: (1) A metabolic factor with significant loadings for log(FPG), log(TG), HDL-C−1, and WC and near-zero loading for DBP, SBP, and log(WBC) in 9458 of the bootstrap samples; (2) a blood pressure factor with highly significant loadings for DBP and SBP and near-zero loadings for the other variables in 9430 bootstrap samples; and (3) an inflammatory factor in 9464 bootstrap samples with median loadings being clearly above the cutoff for log(FPG) and log(WBC), but with a CI for the factor loading of log(FPG) covering zero (Table 3). In a total of 9430 (94.3%) out of the 10,000 bootstrap samples, the order of the factors remained the same in men. In women the first and second factors were interpreted as: (1) A metabolic-inflammatory factor with significant loadings for log(FPG), log(TG), HDL-C−1, WC, and log(WBC) and near-zero loading for DBP and SBP and (2) a blood pressure factor with highly significant loadings for DBP and SBP and near-zero loadings for the other variables (see Table 3). These results remained the same over all 10,000 bootstrap replicates. The bootstrap clouds in Fig. 2 show that the components of the first factor are much tightly clustered in women than in men.
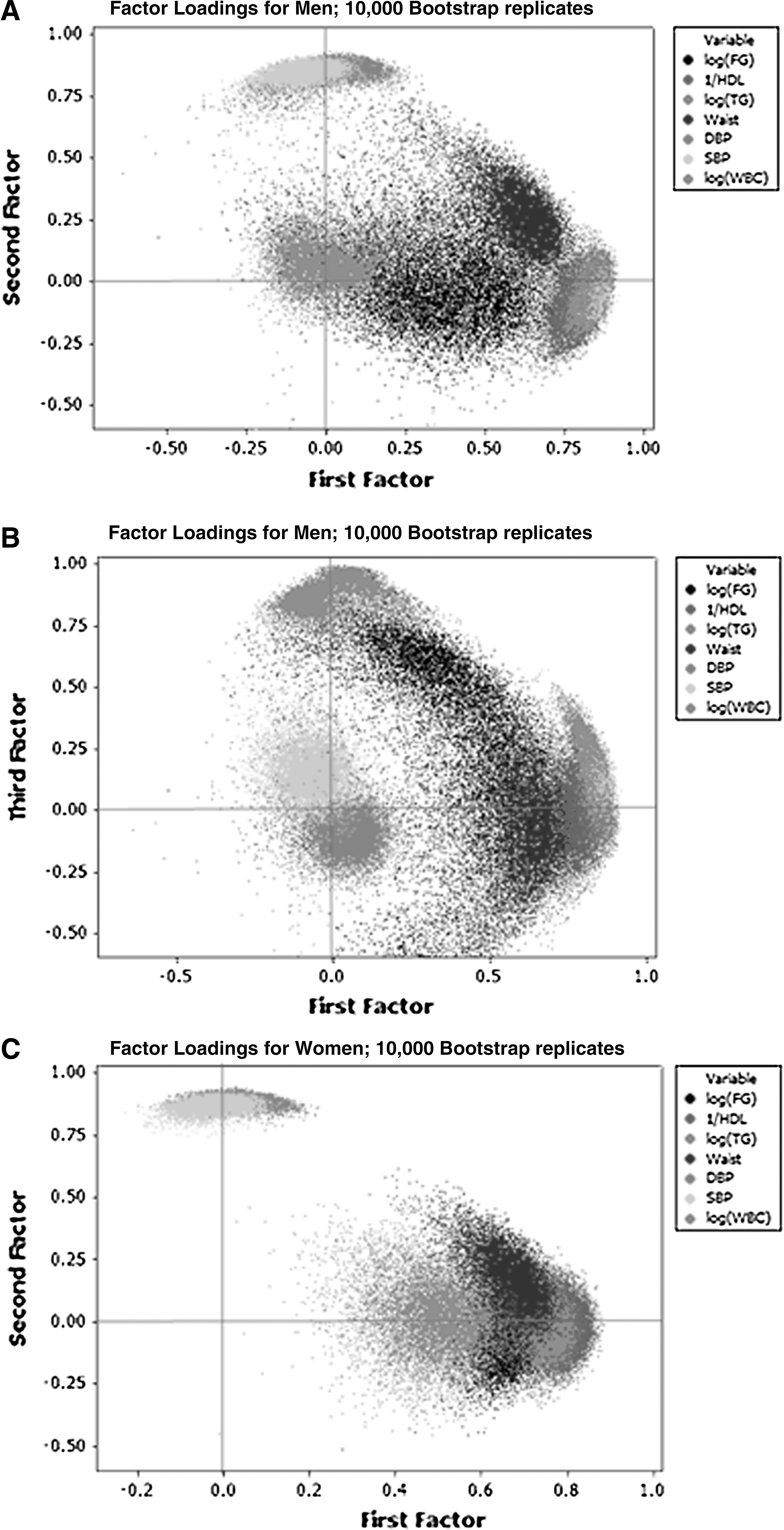
Bootstrap clouds (10,000 bootstrap samples) of the factor loadings for white blood cell count (WBC) and the individual components of the metabolic syndrome in optimally reflected varimax rotated space.
First factor, metabolic/metabolic-inflammatory; second factor, blood pressure; and third factor, inflammatory, men only. Loadings of the individual components included in the respective factor in bold (cutoff=0.30).
Only for the inflammatory factor did the sample loadings differ from the median of the bootstrap sample loadings with more than 2 units in the second decimal 0.49 vs 0.44 for log(FPG) and 0.90 vs 0.87 for log(WBC).
FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; TG, triglycerides; DBP, diastolic blood pressure; SBP, systolic blood pressure; WBC white blood cells.
Ten-year mortality
During a median follow-up of 10.6 years (range 0.2–10.9), 145 (37%) individuals died [90 (46%) men and 55 (28%) women]. The sex difference in mortality was highly significant (p<0.001); for men 5.4 deaths/100 person-years at risk and for women 2.8 deaths/100 person-years at risk. The main causes of death were cardiovascular (40 men; 27 women) and malignancy (27 men; 11 women). Ten-year mortality among the 185 invited individuals (89 men; 96 women) who did not participate in the study was considerably higher—66 (74%) among men and 44 (46%) among women.
The metabolic and the inflammatory factors in men and the metabolic-inflammatory factor in women were significantly related to 10-year mortality (Table 4). The blood pressure factor had opposite nonsignificant effects in men and women, being negatively related with mortality in women. The interaction between the blood pressure factor and sex was nearly significant (p=0.085). In a pooled analysis, the prognostic impact of the metabolic/metabolic-inflammatory factor was only little attenuated upon adjustment for known hypertension, previous myocardial infarction, and current smoking, the only significant confounders using AIC as performance measure in best subset approach (Table 5). The predictive ability, measured as AIC and AUC t =10 years, was almost equivalent for the metabolic/metabolic-inflammatory factor, HDL-C−1, log(WBC) and the models including two or more of the individual variables of the metabolic/metabolic-inflammatory factor adjusting for the above mentioned confounders (Table 5). If one were to select the model with the best prognostic ability, the choice would stand between the model including HDL-C−1 and log(WBC) (AIC=1500.5, AUC t=10 years=0.710) and the model including log(FPG), HDL-C−1, log(TG), and log(WBC) (AIC=1501.5, AUC t=10 years=0.713).
Akaike information criterion for the model including the metabolic and the inflammatory factor.
p value for Wald χ2 for the model including the metabolic and the inflammatory factor.
Akaike information criterion for the model including the blood pressure factor, sex, and the interaction.
AIC, akaike information criterion; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; TG, triglycerides; WBC, white blood cell; DBP, diastolic blood pressure; SBP, systolic blood pressure.
Adjusted for sex, known hypertension, previous myocardial infarction, and current smoking.
p value for the difference in Wald χ2 between the full model and the model only including the adjusting variables.
Adjusted for known hypertension, previous myocardial infarction, and current smoking.
p value for Wald χ2 for the model including only the adjusting variables.
AIC, akaike information criterion; AUC t =10 years, time-dependent area under the receiver operating characteristic (ROC) curve after 10 years; FPG. fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; TG, triglycerides; WBC, white blood cells.
The prognostic impact of the WBC count was only little attenuated upon further adjustment for statin treatment (data not shown). The reason for this adjustment was that statins have an anti-inflammatory effect as shown by lowering CRP. 21,22 This effect is independent of the cholesterol-lowering effect of statins.
Discussion
Cross-sectional findings
The present factor analysis of the individual components of the metabolic syndrome and WBC count in a community-based cohort of 75 year olds revealed two main factors in women—first, a metabolic-inflammatory factor comprising WBC count and all components of metabolic syndrome except blood pressure and, second, blood pressure alone. In men the metabolic-inflammatory factor was split into a metabolic and an inflammatory factor. The first key message of the present study is the close association between the WBC count and the metabolic components of metabolic syndrome in women. This association was not found in men, and the sex disparities were statistically significant for the associations between the WBC count and FPG and HDL-C. In the present elderly population, we found that women had a stronger relationship between the WBC count and insulin sensitivity 10 earlier. Furthermore, we have reported a significantly stronger association between WC and insulin resistance in women than in men, 23 indicating sex disparity between these two key variables of the metabolic syndrome. To our knowledge, this is the first report relating WBC count to the individual components of the metabolic syndrome. Likewise, we have found no report addressing sex differences in the clustering of component variables of the metabolic syndrome and the WBC count.
A close relation between markers of inflammatory processes and the metabolic syndrome has previously been reported. 4 –14,24 –26 For example, hs-CRP 7,25,26 and the WBC count 4,5,8,10 –13 are closely related to the metabolic syndrome. Obesity, especially visceral obesity, is characterized by a broad inflammatory response mediated by several inflammatory mediators, in particular the proinflammatory cytokines. 25 –27 The associations between the WBC count and the metabolic components of the metabolic syndrome in women, described in the present article, may be explained by cytokine effects on the production of WBC.
Ten-year mortality
The second key message of the present report is that the metabolic and the inflammatory factors in men and the metabolic-inflammatory factor in women, derived by a factor analysis of the individual components of the metabolic syndrome and the WBC count, have a considerable negative effect on 10-year survival, which remains after adjusting for established cardiovascular risk factors.
Lehto et al. 28 derived four factors in a factor analysis using conventional cardiovascular risk factors, not including the WBC count, among middle-aged patients with type 2 diabetes. One of the factors, derived from their factor analysis, was similar to the metabolic factor described by us. 3 This factor predicted coronary death in accordance with our findings in a community-based cohort of 75 year olds. We have not found any other investigation on the prognostic implications of a metabolic-inflammatory factor like ours. In men, the metabolic and inflammatory factors per se as well as their combination was significantly associated with dismal survival (p=0.008, p=0.009, and p=0.003), indicating that adding the inflammatory factor significantly improves the predictive ability. This is due to the weak association between the WBC count and the components of the metabolic factor in combination with an independent prognostic ability of the WBC count. In women, the metabolic-inflammatory factor was significantly associated with dismal survival (p=0.010), which was not the case for the metabolic factor described earlier (p=0.072), 3 indicating that while being strongly associated with the components of the metabolic factor, the WBC count per se confers a substantial contribution to the prognostic ability of the metabolic-inflammatory factor. The above unadjusted and adjusted prospective associations did not change noticeably when adjusting for statin treatment.
Notably the predictive effects on mortality of the metabolic-inflammatory factor/factors, derived in our analysis, were very little attenuated by adjustment for established cardiovascular risk factors. Thus, this prognostic effect is unlikely to be an effect solely of established atherosclerotic disease.
It has been clearly demonstrated that atherosclerotic disease is driven at a fundamental level by inflammatory processes.
29,30
Studies of inflammation status in relation to vascular outcomes are common and range from WBC count determination to assessment of CRP, interleukins, cellular adhesion molecules, and markers of plaque stability.
31
Most attention has been on CRP; concentrations in the top third of the population are associated with an increased risk of approximately 50% for first future coronary and stroke events.
6
Among middle-aged women from the Women's Health Initiative (WHI) study, Margolis et al.
16
found that WBC count in the top quarter of the population (>6.71×109 cells/L) was associated with an approximate 50% increase in the risk of cardiovascular disease and total mortality. This is in agreement with our findings. Similar findings concerning cardiovascular and total mortality have been reported from other populations of middle-aged men and women
32,33
and in the elderly.9
Strengths and limitations of the study
The restriction of our investigation to one age class enables us to leave out age as a confounding factor, creating the possibility of a meaningful analysis of the clustering of the metabolic syndrome components and the WBC count and their impact on all-cause mortality, despite the relatively small number of participants in the study. Furthermore, because of high participation rate, the participants are more representative for the population in a defined geographical area than described in most other studies on this topic. These advantages are, however, obtained at the cost of the difficulties of generalizing our findings to individuals not being 75 years old and to people from other geographical areas. However, it seems likely that our results are applicable to North Europeans and white North Americans of Caucasian origin in their seventies.
Factor analysis should only be regarded as an exploratory tool for studying lower dimensional structures in high dimensional data sets. Bearing in mind that it results in an idealized approximation of the truth, such an approximation may, however, prove a valuable starting point for better understanding of the etiology and pathogenesis behind low-grade inflammation and the metabolic syndrome.
A further limitation of the study is the fact that among invited individuals who did not participate the 10-year mortality was considerably higher (59%) than among those invited individuals who participated (37%), mainly reflecting a high prevalence of severe chronic diseases among nonparticipants. Consequently, the examined cohort represents the healthiest two-thirds of a general population.
Conclusions
By including WBC count in a factor analysis of the metabolic syndrome components, a metabolic-inflammatory factor/factors closely related to survival was identified. This finding adds to previous clinical evidence of a close relationship between the metabolic syndrome and low-grade inflammatory activity. Previously, hsCRP has been used as a marker of low-grade inflammatory activity, but the present study suggests that WBC may be of clinical value in this context.
Footnotes
Acknowledgments
This work was supported by grants from Västmanland's research foundation against cardiovascular disease and SparbanksstiftelsenNya. The corresponding author had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
No competing financial interests exist.