
Abstract
Background:
Hispanics are the fastest growing segment of the U.S. population and have a higher prevalence of cardiometabolic risk factors as compared with non-Hispanic whites. Further data suggests that Hispanics have undiagnosed complications of metabolic syndrome, namely diabetes mellitus, at an earlier age. We sought to better understand the epidemiology of metabolic syndrome in Hispanic women using data from a large, community-based health screening program.
Methods:
Using data from the Sister to Sister: The Women's Heart Health Foundation community health fairs from 2008 to 2009 held in 17 U.S. cities, we sought to characterize how cardiometabolic risk profiles vary across age for women by race and ethnicity. Metabolic syndrome was defined using the updated National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) guidelines, which included three or more of the following: Waist circumference ≥35 inches, triglycerides ≥150 mg/dL, high-density lipoprotein (HDL) <50 mg/dL, systolic blood pressure ≥130 mmHg or diastolic blood pressure ≥85 mmHg, or a fasting glucose ≥100 mg/dL.
Results:
A total of 6843 community women were included in the analyses. Metabolic syndrome had a prevalence of 35%. The risk-adjusted odds ratio for metabolic syndrome in Hispanic women versus white women was 1.7 (95% confidence interval, 1.4, 2.0). Dyslipidemia was the strongest predictor of metabolic syndrome among Hispanic women. This disparity appeared most pronounced for younger women. Additional predictors of metabolic syndrome included black race, increasing age, and smoking.
Conclusions:
In a large, nationally representative sample of women, we found that metabolic syndrome was highly prevalent among young Hispanic women. Efforts specifically targeted to identifying these high-risk women are necessary to prevent the cardiovascular morbidity and mortality associated with metabolic syndrome.
Introduction
Although there are limited studies primarily focusing on the socioeconomic and biological factors that may influence these noted disparities, studies have indicated that issues related to health care and access to care may be contributing to the greater prevalence of metabolic syndrome among Hispanic women. 6 Hispanics have the youngest average age of those with undiagnosed type II diabetes mellitus (T2DM) and the highest levels of glycosylated hemoglobin of any racial or ethnic group. 7 Additionally, metabolic syndrome may pose significantly higher risks of vascular events, including stroke, among Hispanic women. 8 These limited data highlight the importance of specifically targeting the Hispanic population, particularly Hispanic women, in studies to better understand metabolic syndrome.
We sought to better understand the epidemiology of metabolic syndrome among Hispanic women within the community using health data gathered through Sister to Sister (STS), a community-based health screening program of The Women's Heart Health Foundation.
Methods
Study population
Sister to Sister (STS): The Women's Heart Health Foundation Registry is a national grass-roots organization that provides free public health screenings for women annually in 17 U.S. cities. 9,10 STS was established in 2000 with an aim of preventing heart disease by identifying cardiometabolic risk factors in community women across the country. STS oversamples members of racial and ethnic minority groups, in order to obtain a sample representative of the U.S. population.
Screening events were advertised on the STS website and through local community advertisements. Screenings consisted of a standardized questionnaire, cardiometabolic risk factor measurement by trained personnel, physical screening, and individualized counseling about identified risk factors. Bilingual screeners were available to participants in most cities. All participants signed a consent form prior to participation in the screening events. This study was approved by Quorum Institutional Review Board (Seattle, Washington).
Metabolic syndrome was defined using the updated National Cholesterol Education Program Adult Treatment Program (NCEP ATP III) guidelines, which included three or more of the following: Waist circumference ≥35 inches, triglycerides ≥150 mg/dL, HDL <50 mg/dL, systolic blood pressure (SBP) ≥130 mmHg or diastolic blood pressure (DBP) ≥85 mmHg, or a fasting glucose ≥100 mg/dL. 11,12 Blood pressure was taken while women were in a seated position after several minutes of rest. BMI was calculated using participants' height in meters squared and measured weight in kilograms. Waist circumference was measured with the measuring tape around the superior-most part of the iliac crest. Blood glucose and cholesterol levels were measured using the previously validated Cholestech System Fingerstick test. 13 Participants were categorized as non-Hispanic white, black, Hispanic, or other based on race (white, black, Asian, other) and ethnicity (Hispanic, non-Hispanic) variables within the STS data. Additional demographic data included annual household income and insurance status (Medicare, Medicaid, private, or uninsured). Participants with missing age, race/ethnicity, or any component of the metabolic syndrome screening were excluded from the analysis.
Statistical analysis
We conducted descriptive and bivariate analyses to illustrate baseline demographics, vital signs, and laboratory test data by race/ethnicity groups. Chi-squared and t-tests were used for bivariate comparisons as appropriate. We constructed a hierarchical generalized linear model (HGLM) to access the relationship between race/ethnicity and metabolic syndrome. This was fitted with a random city-specific effect to account for within-city correlation of the metabolic syndrome and separate within-city variation from between-city variation. The 95% confidence interval (CI) was calculated for each estimate obtained from the model. All statistical testing was two-sided, at a significance level of 0.05, and all analyses were conducted using SAS version 9.3 64-bit Windows version (SAS Institute Inc., Cary, NC).
Results
A total of 18,892 women were screened in 2008–2009 across 17 U.S. cities. After excluding women with missing age (n=1564), race/ethnicity (n=2081), or any component of metabolic syndrome (n=9268), our final sample size consisted of 6843 women. After excluding women with missing age (n=1564), race/ethnicity (n=2081), or any component of metabolic syndrome (n=9268), our final sample size consisted of 6843 women. There were no differences in metabolic syndrome scores between women with missing age and women without missing age (median scores 2.0 vs. 2.0) and between women with missing race/ethnicity and women without missing race/ethnicity (median scores 2.0 vs. 2.0). There were differences in the metabolic syndrome scores among race/ethnicity groups. Black women had more missing data (40.9% missing vs. 35.6% nonmissing), whereas Hispanic (12.1% vs. 16.7%), other race (6.8% vs. 6.9%), and non-Hispanic white women (34.7% vs. 40.9%) had less missing data.
Of these women in the final study sample, 863 (12.6%) were Hispanic, 2544 (37.2%) were black, 2921 (42.7%) were non-Hispanic white, and 515 (7.5%) self-identified as other. As compared with other racial and ethnic groups, Hispanic women were younger with a mean age of 44.6 (Table 1). Hispanic women had the highest triglyceride and lowest HDL cholesterol (HDL-C) levels as compared with both blacks and non-Hispanic whites (p<0.001). Almost two-thirds of Hispanic participants reported being uninsured and 29% reported a mean household income of less than $20,000.
All p values account for multiple comparisons between groups.
SD, standard deviation; HDL-C, high-density lipoprotein cholesterol; TGs, triglycerides; WC, waist circumference; BMI, body mass index; SD, standard deviation; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Table 2 describes the prevalence of metabolic syndrome and its components among our study sample. Overall, 35% of all participants met the criteria for metabolic syndrome. The prevalence was significantly higher in Hispanic and black women. Hispanic women had higher rates of dyslipidemia with high triglycerides and low HDL-C levels, whereas black women had higher rates of elevated waist circumference and hypertension as compared with non-Hispanic whites (p<0.001).
Defined as systolic blood pressure ≥130 or diastolic blood pressure ≥85 or pharmacologic treatment for hypertension.
WC, waist circumference; TGs, triglycerides; HDL, high-density lipoprotein; HTN, hypertension.
Overall, Hispanic women had higher rates of metabolic syndrome across all ages. Young Hispanic women under the age of 35 had a significantly higher prevalence of metabolic syndrome, although the rate of increase by age appeared to be linear (Fig. 1). Although the prevalence of metabolic syndrome declined for other racial/ethnic groups with increasing age, the rate of increase remained constant for older Hispanic women. Similarly, few community women had optimal levels lipid levels as defined by triglycerides <150 mg/dL and HDL-C>50 mg/dL. This disparity was most pronounced for young Hispanic women (Fig. 2). Only 18% of Hispanic women had optimal lipid levels as compared with 27% of black women and 25% of non-Hispanic white women.
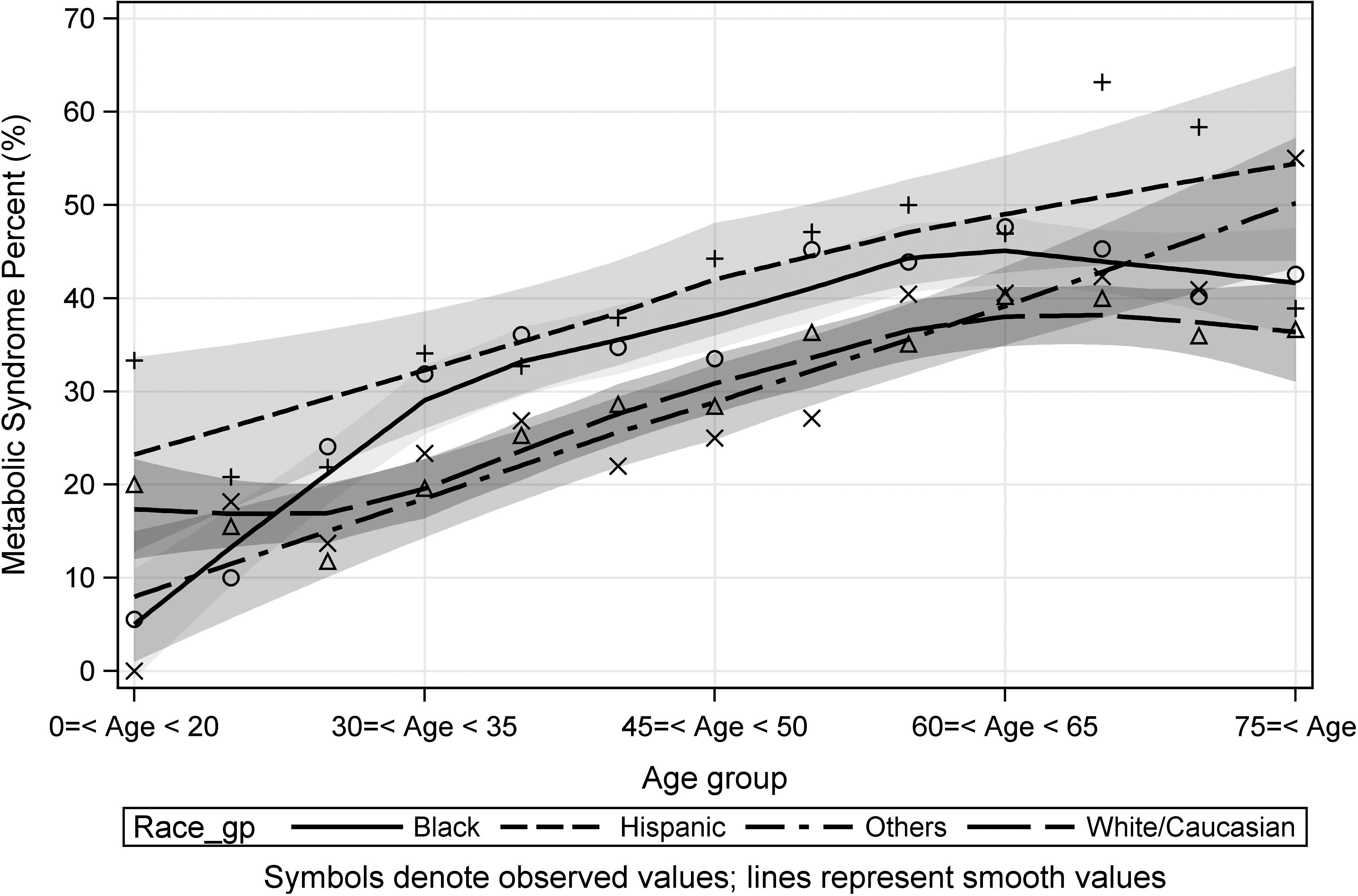
Prevalence of metabolic syndrome by race/ethnicity and age. The shaded regions represent the 95% confidence interval for each data point.
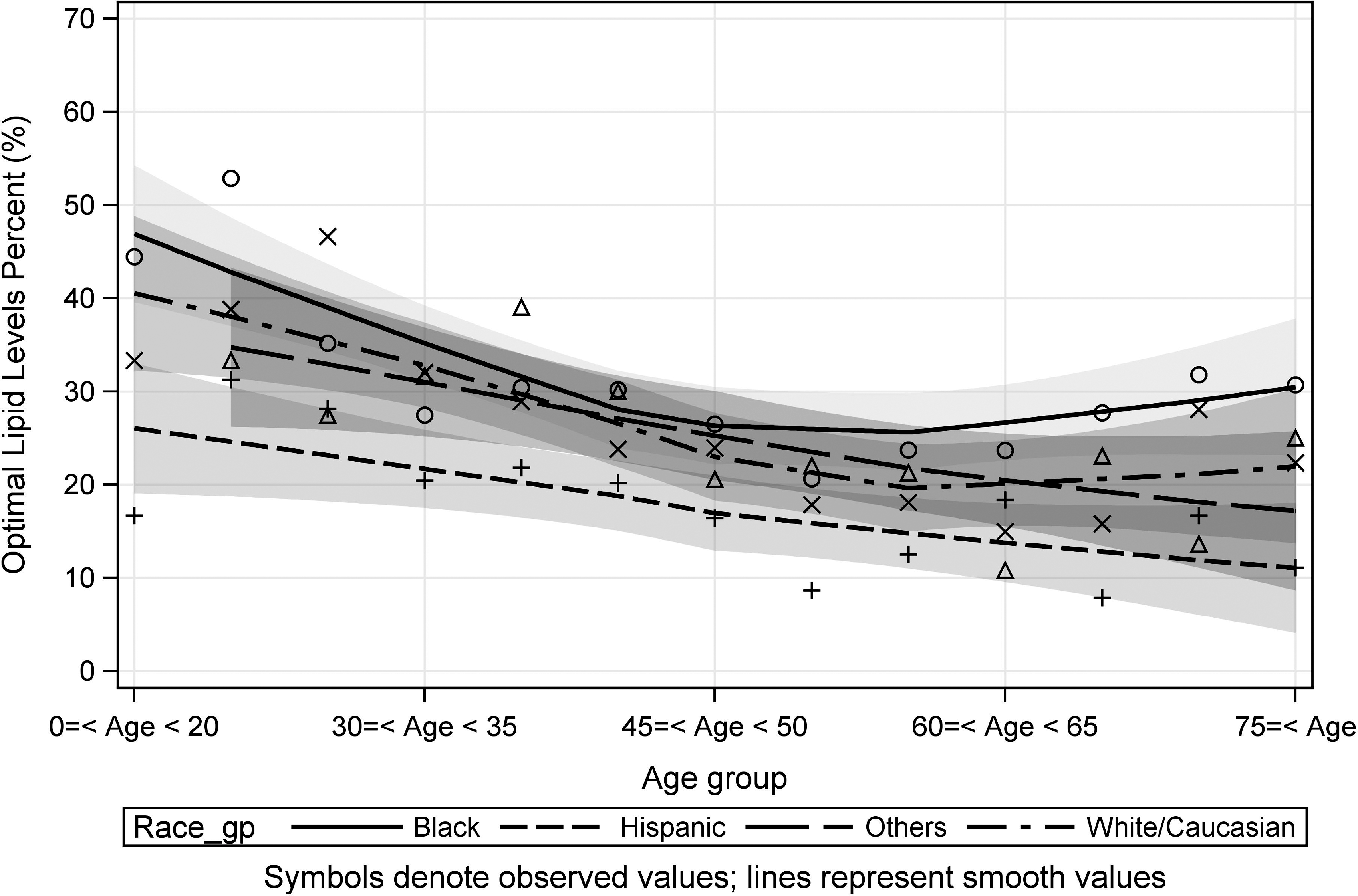
Optimal lipid levels by race/ethnicity and age. The shaded regions represents the 95% confidence interval for each data point. Optimal lipid levels defined by high-density lipoprotein cholesterol >50 mg/dL and triglycerides <150 mg/dL.
Table 3 shows the association between race/ethnicity and metabolic syndrome in our community cohort, adjusting for participants' age and smoking status. Hispanic ethnicity was associated with a 1.65 times higher odds of having metabolic syndrome compared with non-Hispanic white women. Similarly, black participants had a 1.4 times higher odds of having metabolic syndrome as compared with non-Hispanic whites. Smoking [odds ratio (OR)=1.3, 95% confidence interval (CI) 1.05,1.60] and increasing age at 5 year increments (OR=1.13, 95% CI 1.11,1.15) were also associated with a significant increase in the prevalence of metabolic syndrome.
Adjusted for age (per 5-year incremental increase in age) and smoking status.
Discussion
We found a high prevalence of metabolic syndrome among a large sample of community women with a prevalence of 35%, and even higher rates among members of racial and ethnic minority groups. Hispanic women were 65% more likely to have metabolic syndrome as compared with non-Hispanic whites. This disparity was largely driven by dyslipidemia, particularly among young and middle-aged Hispanic women. These findings highlight the importance of identifying these women early to prevent the known complications of metabolic syndrome in a growing segment of the U.S. population.
Our findings are consistent with and complementary to prior studies, which have documented the high burden of metabolic syndrome in Hispanics. 1,14 These findings are particularly alarming because of the high rates of metabolic syndrome in young women. One study showed that Hispanic adolescents had the highest prevalence of metabolic syndrome 15 and that, paralleling the obesity epidemic, rates of metabolic syndrome continue to rise disproportionately amongst members of racial and ethnic minority groups.
We also found that the rate of increase in metabolic syndrome with age persisted for older Hispanic women, while it appeared to decrease for non-Hispanic white and black women in the same age group. The overall prevalence of metabolic syndrome is known to increase with age, particularly in women. 16 However, it is not clear why elderly Hispanic women in our cohort were the key drivers of this pattern. Studies have shown that Hispanic women have higher insulin resistance as compared with other groups and this becomes even more evident with age. This propensity toward insulin resistance may explain the increase in the prevalence of metabolic syndrome in elderly Hispanic women. Additionally, Hispanic women in our study were, on average, younger than non-Hispanic white and black participants, which may result in a skewed distribution of our findings. Further studies are warranted to investigate patterns of insulin resistance and racial and ethnic disparities with increasing age.
Interestingly, dyslipidemia appeared to the primary driver of metabolic syndrome among Hispanic women in our sample. One possible explanation for this finding is that hepatic fat accumulation predisposes to dyslipidemia and is almost twice as common in Hispanics as compared with blacks and other ethnic groups. 17 Hypertriglyceridemia has been associated with insulin resistance in many large studies. 18 Early diagnosis of metabolic syndrome represents an important opportunity for early lifestyle interventions to help reduce health disparities, particularly among members of racial and ethnic minority groups who suffer from a disproportionate burden of cardiovascular disease (CVD) morbidity and mortality.
Awareness of CVD risk continues to lag behind in members of racial and ethnic minorities. 19,20 One possible explanation for our findings is that almost two-thirds of the Hispanic women in our sample were uninsured, suggesting that many of these women likely have no access to a regular source of preventive health care. Similarly, recent census data estimates that only 66.8% of Hispanic Americans have medical insurance as compared to 90% of non-Hispanic whites. 21 This may partly explain why Hispanics are much less likely to report routine medical care or the use of lipid and blood pressure–lowering drugs. 7 It is likely that many of the women in our study were unaware of their cardiac risk profiles. Alternatively, low socioeconomic position may be independently linked to higher rates of metabolic syndrome, particularly in women. 6,22,23 In our study, Hispanic participants had the lowest mean household income, with almost 30% reporting an income under $20,000 a year. Possible mechanisms linking lower socioeconomic status to metabolic syndrome include lack of neighborhood access to healthy food and exercise options, predisposing inhabitants of poorer neighborhoods to engage in unhealthy lifestyles. Similarly, low socioeconomic status is associated with lack of access to health care and lower access to high-quality care.
Several limitations warrant mention. Our data are cross-sectional, which limits our ability to infer causality. We were unable to disaggregate the Hispanic ethnic group into important subgroups. There is significant heterogeneity among Hispanics. However, we lacked data on important differences such as country of origin, English language proficiency, and other measures of acculturation that may be important contributors to our findings. To have full information on metabolic syndrome and other important risk factors in our statistical models, we excluded women who lacked any of the components of metabolic syndrome. This reduced our study sample population to 6843 women. Sensitivity analyses showed that these women were not significantly different from the remainder of the sample for our primary outcomes; however, it is possible that women with missing data were different from those with full data in ways that we cannot fully measure. Our analyses were restricted to women who participated in community health screenings, which limits our ability to generalize our findings to men or women who would otherwise not participate in such screening programs. However, STS overly represented members of racial and ethnic minority groups and young adults—an important strength of this study.
Conclusions
In summary, we found high rates of metabolic syndrome among young Hispanic women. Early identification of these high-risk individuals and aggressive lifestyle intervention is warranted to reduce the risk of T2DM and CVD in this growing population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.