
Abstract
Background:
Studies about the relationship of apolipoproteins (apo) and metabolic syndrome in children are scarce. In this study, we analyze apo levels and determine the best cutoff point of the apoB/A-I ratio to diagnose dyslipidemia in prepubertal children with metabolic syndrome.
Methods:
A community-based, cross-sectional study that enrolled 337 children with Tanner stage 1 and average age and body mass index of 9.7±1.6 years and 19.2±3.8 kg/m2 was carried out. Diagnosis of acute or chronic illnesses constituted the exclusion criteria; in addition, children undergoing medical treatment or receiving vitamins and/or oral supplements were not included.
Results:
Metabolic syndrome was identified in 42 (12.5%) children (19 girls and 23 boys). The mean apoB/A-I ratio in the children with metabolic syndrome was 0.67±0.18. The best cutoff point of the apoB/A-I ratio for recognizing dyslipidemia was 0.60 (area under the receiver operating characteristic curve, 0.778; sensitivity 80%, specificity 55%). A total of 102 children exhibited apoB/A-I ratio ≥0.60. Diagnosis of metabolic syndrome was performed in 42 (41.2%) children. Among children with metabolic syndrome, 38 (90.5%) had hypertriglyceridemia, 34 (81.0%) low high-density lipoprotein cholesterol (HDL-C), 32 (76.2%) hypertriglyceridemia+low HDL-C, and 40 (95.2%) an apoB/A-I ratio ≥0.60.
Conclusion:
Our results show that the best cutoff point of the apoB/A-I ratio for recognizing dyslipidemia in prepubertal children is 0.60 and that among children with metabolic syndrome, an apoB/A-I ratio ≥0.60 is the marker of dyslipidemia with the highest frequency.
Introduction
In the pediatric population, the use of apolipoprotein (apo) levels as a diagnostic tool eliminates the confounder effect related with age variations of high-density lipoprotein (HDL-C) and low-density lipoprotein cholesterol (LDL-C) concentrations, minimizing the false negative results in the early identification of the atherogenic lipid profile. 5 In this regard, it has been reported that the amounts of LDL and HDL particles' major apoB and apoA-I could be better markers of dyslipidemia than their cholesterol concentration, 6,7 and that serum apoB and apoA-I are better indicators of atherogenic/antiatherogenic lipoprotein particles than the conventional measures of LDL-C and HDL-C. 5
Studies about the relationship of apo levels with the metabolic syndrome in children are scarce. 8,9 Although the results of these studies consistently show that the prevalence of metabolic syndrome is significantly associated with increasing tertiles of the apoB/A-I ratio, 9 and that the elevated apoB/A-I ratio may constitute an important feature of metabolic syndrome, 8,9 the need to define the cutoff values of apoB/A-I as an indicator of dyslipidemia in children has been emphasized. 10 The objective of this study was to analyze the apo levels and to determine the best cutoff point of the apoB/apoA-I ratio to diagnose dyslipidemia in prepubertal children with metabolic syndrome.
Materials and Methods
With the approval of protocol by the Ethics Committees of the Faculty of Medicine of the University of San Luis Potosi and the Mexican Social Security Institute at Durango, Mexico, and after obtaining informed assent from children and informed consent from their parents, a community based cross-sectional study was carried out.
The sampling strategy, based on two-stage random sample, has been described elsewhere. 11,12 In brief, students aged 6–12 years and Tanner stage 1, from elementary schools at San Luis Potosi and Durango, cities at middle and northern Mexico, were randomly selected and invited to participate. The number of schools by city and students included by schools was proportional to the required sample size, which was estimated on the basis of detecting a prevalence of dyslipidemia equal or greater than 10%. Diagnoses of acute or chronic illnesses were exclusion criteria; in addition, children undergoing medical treatment or receiving vitamins and/or oral supplements were not included.
According the standards for pediatric apo distribution from the National Health and Nutrition Examination Survey III for Mexico-American children aged 4–11 years, 13 the cutoff points for apoA-I were 139 and 132 mg/dL for girls and boys and 80 mg/dL for apoB in both sexes.
The metabolic syndrome was defined according the adapted criteria by Cook et al. 14 for children and adolescents. The presence of at least three of the following features characterized the presence of metabolic syndrome: Waist circumference ≥90th percentile according age and sex, fasting plasma glucose levels ≥110 mg/dL, blood pressure ≥90th percentile for height and sex, triglycerides levels ≥110 mg/dL, and HDL-C levels ≤40 mg/dL.
Measurements
The blood pressure was measured according recommendations by the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. 15 In brief, using a sphygmomanometer (Microlife AG, Heerbrugg, Switzerland) and stethoscope (3M Littman Classic II, Neuss, Germany), blood pressure measurements were taken with the children seated and their arms bared and supported at heart level, after at least 5 min of rest, and using an appropriate cuff size. The average of three readings separated by 2 min each was used.
Weight and height were measured using a fixed scale with stadiometer (Tanita TBF-215, Tokyo, Japan), with the children in standing position wearing light clothing and without shoes. The increment of weight and height measurements was 0.1 kg and 0.01 m. The body mass index (BMI) was calculated as weight (kilograms) divided by height (meters) squared.
Tanner stage 1 was determined by a trained clinician in accordance with genitalia in boys (testicular volume less than 1.5 mm3 and penis of 3 cm or less) and breast development in girls (breast without glandular tissue and areola that follows the skin contours of the chest). In addition, in both boys and girls, the absence of pubic hair was required.
Assays
A venous whole blood sample was collected after an overnight fast (8–10 h of fasting). apoB and apoA-I were determined with the radial immunodiffusion method. The interassay coefficients of variation were 4.1% and 3.4%, respectively. Triglycerides were measured using enzymatic methods, and the HDL-C fraction was obtained after precipitation by phosphotungstic reagent. The interassay coefficients of variation were 3.6% for triglycerides and 3.0% for HDL-C.
Plasma glucose concentrations were determined using the glucose-oxidase method (Sigma Diagnostics, St. Louis, MO), with an interassay variation coefficient of 3.6%. Samples were frozen and stored at −20°C until further analysis. All measurements were performed in a Data Pro Plus random access clinical analyzer (Arlington, TX).
Statistical analysis
For bivariate analysis, the Student t-test and chi-squared test were used to test differences for numerical and categorical data, respectively. Differences between more than two groups were analyzed by one-way analysis of variance (ANOVA) test with a Bonferroni post hoc test. Skewed numerical data were transformed by Logn, to obtain a symmetrical distribution.
To establish the cutoff point of the apoB/A-I ratio to diagnosis dyslipidemia (triglycerides+HDL-C levels), a receiver operating characteristics (ROC) curve was performed. Sensitivity was defined as the proportion of dyslipidemic children who had a positive test and specificity as the proportion of dyslipidemic-free children who had a negative test. A p value<0.05 defined statistical significance; data were analyzed by using the statistical package SPSS for Windows 15.0.
Results
A total of 1577 children were screened; of them, 178 (11.3%), 125 (7.9%), and 895 (56.7%) were not included because they had acute or chronic diseases, received vitamins, or had a Tanner stage greater than 1, respectively; in addition, 46 (2.7%) children did not agree to participate. Thus, 337 (21.4%) children who met the inclusion criteria were enrolled—169 (50.1%) girls and 168 (49.9%) boys, with average age and BMI of 9.7±1.6 years and 19.2±3.8 kg/m2, respectively.
Metabolic syndrome was identified in 42 (12.9%) children—19 girls and 23 boys (p=0.60). There were no significant differences in anthropometric and biochemical variables between girls and boys, with and without metabolic syndrome (Table 1). In girls and boys without metabolic syndrome, apoA-I was significantly higher and apoB significantly lower than in the girls and boys with metabolic syndrome.
Values are mean±standard deviation (SD).
P value between girls and boys.
P<0.001 between girls with and without metabolic syndrome.
P<0.001 between boys with and without metabolic syndrome.
HDL-C, high-density lipoprotein cholesterol; apo, apolipoprotein.
Triglycerides, apoB, and the apo-B/A-I ratio showed a significant positive association according BMI, whereas HDL-C showed a statistically significant decrease. Although without statistical significance, apoA-I showed a decreasing trend according BMI. In addition, as expected, the blood pressure and glucose levels exhibited a significant positive increase by weight class (Table 2).
Values are mean±standard deviation (SD).
P<0.05 between normal-weight and overweight groups.
P<0.05 between normal-weight and obese groups.
P< 0.05 between overweight and obese groups.
HDL-C, high-density lipoprotein cholesterol; apo, apolipoprotein.
The mean±standard deviation (SD) of the apoB/A-I ratio in the overall population was 0.54±0.16; the apoB levels and apoB/A-I ratio showed a significant increase and apoA-I levels a significant decrease according the number of the components of metabolic syndrome (Table 3).
Values are mean±standard deviation (SD).
apo, apolipoprotein.
The mean±SD of the apoB/A-I ratio in the children with metabolic syndrome was 0.67±0.18. The best cutoff point of the apoB/A-I ratio to recognize dyslipidemia (hypertriglyceridemia+low HDL-C) was 0.60 (sensitivity 80%, specificity 55%) (Fig. 1C). In addition, the ROCs for the apoB/A-I ratio to low HDL-C and hypertriglyceridemia are shown in Fig.1, A and B, respectively.
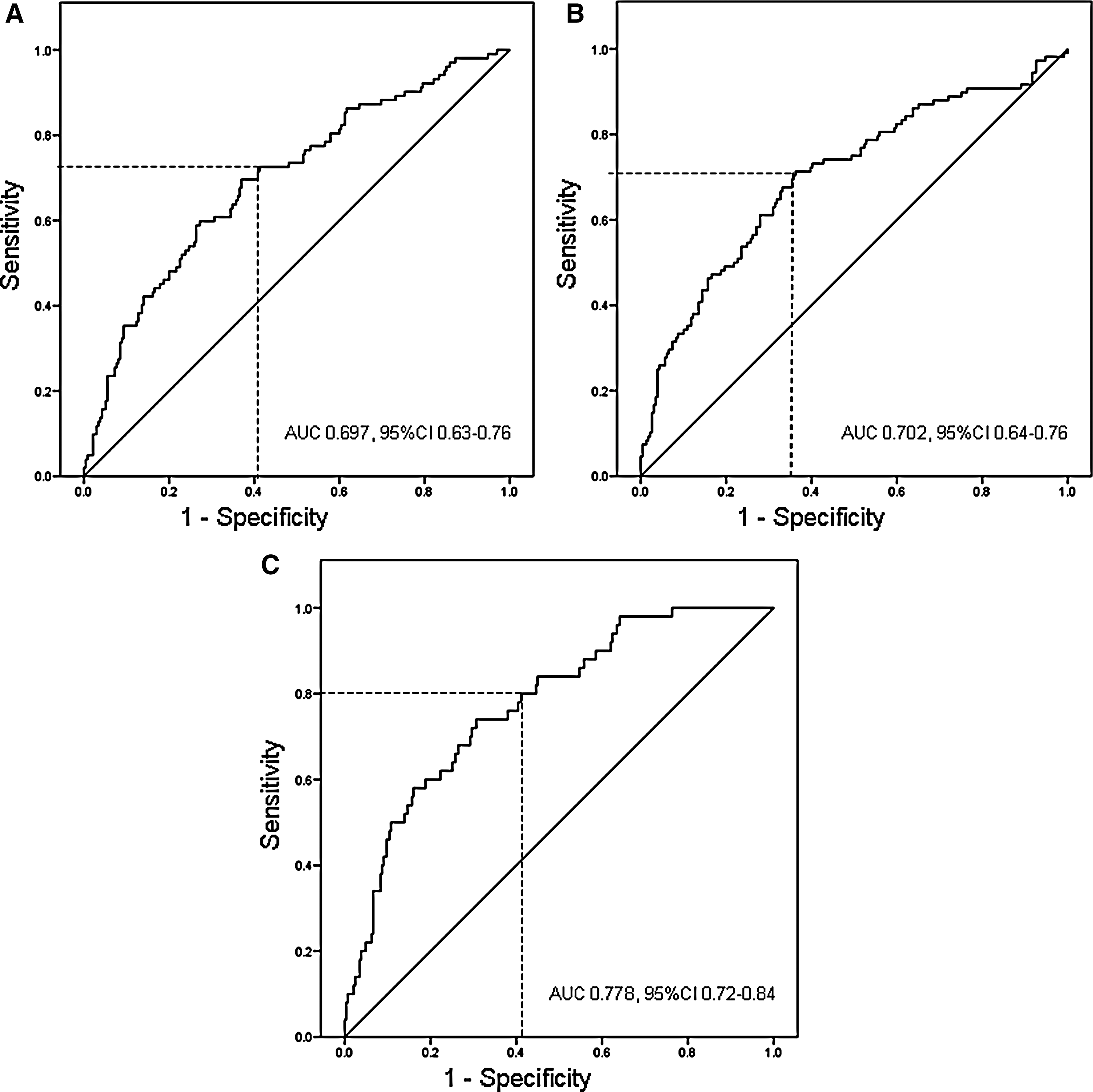
Receiver operating characteristics (ROC) curve for the apolipoprotein B/A-I (apoB/A-I) ratio to high-density lipoprotein cholesterol (HDL-C)
A total of 102 children exhibited an apoB/A-I ratio ≥0.60; a diagnosis of metabolic syndrome was performed in 42 (41.2%) children. Among children with metabolic syndrome, 39 (92.9%) had obesity, 22 (52.4%) elevated blood pressure, 3 (7.1%) hyperglycemia, 38 (90.5%) hypertriglyceridemia, 34 (81.0%) low HDL-C, 32 (76.2%) hypertriglyceridemia+low HDL-C, and 40 (95.2%) an apoB/A-I ratio ≥0.60.
Interestingly, children with an apoB/A-I ratio ≥0.60 exhibited higher, denser LDL than children below the cutoff (91.7±20.8 mg/dL versus 73.6±18.5 mg/dL, p<0.0005).
Discussion
Our results show that among children aged 6–12 years, the best cutoff point of the apoB/A-I ratio for recognizing dyslipidemia is 0.60, and that in children with metabolic syndrome, an apoB/A-I ratio equal or greater than 0.60 has a higher frequency as compared with the triglycerides, HDL-C, or triglycerides+HDL-C levels. In this regard, in the study population, the absolute levels of apoB and apoA-I that are related to the presence of dyslipidemia (triglycerides+HDL-C levels) were 80 and 132 mg/dL, respectively.
Recently, Sellers et al., 16 who studied Aboriginal Australian children with an average age of 11.4 years (range 8.9–13.8 years), suggested that expanding screening strategies using apoB/A-I ratio early in life might be useful for identifying children at risk. Our results show that the cutoff point of the apoB/A-I ratio that indicates dyslipidemia in the prepubertal children is equal or greater than 0.60.
In the Aboriginal Australian Study, 16 the Bogalusa Heart population Study, 5 and the Taipei Children Heart Study, 17 girls showed significantly higher values of apoB and apoA-I levels as compared with boys; in our population, the apoB and apoA-I levels were similar in girls and boys. Differences between our results and others could be related to the age and hormonal status of the targeted populations; in this regard, in our study only girls and boys with Tanner stage 1 were enrolled, as compared with other studies 5,16,17 that included children and adolescents. Therefore, it is possible that sexual hormonal activity plays an important role in apo levels. Given that there are no previous reports regarding the apoB/A-I ratio in prepubertal population, further research is needed in the field.
In Native Canadian young, 18 the increased apoB/A-I ratio resulted primarily from an increase in the apoB levels, whereas in the Australian Aboriginal children 16 from the decrease in apoA-I. In contrast, in our population the balance between apoB and apoA-I was disrupted by both the increase in apoB and decrease of apoA-I levels, differences that could be related to ethnic background.
It has been reported that an elevated apoB/A-I ratio may constitute an important feature of metabolic syndrome in the children 8,9 ; our results strongly support this statement. In addition, to the best of our knowledge, there are no previous reports that had evaluated the cutoff point of the apoB/A-I ratio for recognizing dyslipidemia in children. Our results show that an apoB/A-I ratio equal or greater than 0.60 is the marker of dyslipidemia with the highest frequency in prepubertal children with metabolic syndrome. However, it is necessary to keep in mind that measurements of apoB and apoA-I are not well standardized and are not available in all laboratories; in addition, as triglycerides levels increase, measurement of apoB is more difficult These issues that could limit the use of apoB/A-I ratio in the clinical practice.
The main limitation of our study is that we did not measure the customary diet of the targeted population, a variable that exerts an important role on the lipid profile. However, the sampling strategy of our study minimizes the impact of this limitation.
In conclusion, our results show that in prepubertal children, the best cutoff point of the apoB/A-I ratio for recognizing dyslipidemia is 0.60 and that an apoB/A-I ratio equal or greater than 0.60 is the marker of dyslipidemia with the highest frequency.
Footnotes
Acknowledgments
This work was supported by grants from SHIGO-CONACYT 2002020201, the FAI-UASLP CO2-10-13.53, and the Mexican Social Security Institute Foundation, Civil Association.
Author Disclosure Statement
No competing financial interests exist.