
Abstract
Background:
Studies investigating the effects of dipeptidyl peptidase-4 inhibitors on hepatic steatosis are lacking. We aimed to determine the effects of sitagliptin on nonalcoholic fatty liver disease (NAFLD) in rats with diet-induced obesity.
Methods:
A total of 24 adult female Sprague-Dawley rats, which were 24 weeks old and weighed 199–240 grams, were used. The rats were randomly separated into two groups. The control group (n=6) was fed with standard rat diet; the remaining rats (n=18) were fed with a high-fat diet (HFD) to induce NAFLD. After 12 weeks, rats that were fed with a HFD were randomly separated into two groups: (1) HFD-only group (n=8) was fed with a HFD for an additional 4 weeks, (2) HFD-sitagliptin group (n=10) received sitagliptin (3 mg/kg) for 4 weeks in addition to HFD. At the end of the study (16th week), blood samples were drawn from all rats to determine serum glucose, triglyceride, cholesterol, alanine aminotransferase (ALT), and plasma insulin levels. Insulin resistance was determined using the homeostasis model assessment of insulin resistance (HOMA-IR) index. Histopathologic evaluation of liver samples was undertaken.
Results:
The HFD-sitagliptin group had significantly lower serum glucose (140.8±18.8 vs. 224.7±20.6 mg/dL, P<0.001), plasma insulin (15.8±4.4 vs. 28.0±5.9 μIU/L, P<0.001), HOMA-IR index (4.9±1.8 vs. 15.9±2.3, P<0.001), serum triglycerides (199.0±108.7 vs. 468.0±370.7 mg/dL, P<0.001), and cholesterol (82.0±26.7 vs. 90.5±7.0, P<0.001) values compared to the HFD-only group. Hepatic steatosis was significantly less (mean score, 1 vs. 2; P<0.001) in the HFD-sitagliptin group compared to the HFD-only group, whereas there was no difference in hepatic inflammation (P=0.057), liver weight (P=0.068), and ALT levels (P=0.232).
Conclusion:
Sitagliptin may improve hepatic steatosis by increasing insulin sensitivity and improving lipid profiles in rats.
Introduction
Glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) are incretin hormones that are released from the intestine following oral ingestion of nutrients. 5 They promote insulin secretion from pancreatic β-cells. GLP-1 regulates postprandial glucose disposal by inhibiting glucose-dependent glucagon secretion from α-cells and delaying gastric emptying. 5 Dipeptidyl peptidase-4 (DPP-4) is an enzyme involved in degradation of the intact (active) incretin hormones to inactive metabolites. 6 DPP-4 inhibitors enhance levels of these gut-derived active incretin hormones that are released into the circulation after ingestion of a meal, 7 thereby decreasing the postmeal rise in glucose concentrations and reducing fasting glucose concentrations in a glucose-dependent manner 8,9 with a modest efficacy in lowering glycosylated hemoglobin (HbA1c) compared to other antihyperglycemic agents and a low potential for hypoglycemia and weight change. 10 Incretin-based therapies (GLP-1 analogs and DPP-4 inhibitors) are new classes of antidiabetic agents used in the treatment of T2DM.
The effect of incretin-based therapies on liver steatosis and NASH has become an interesting field of research. Previous studies suggested that GLP-1 activation influences the liver through regulating insulin sensitivity and expression of transcription factors and enzymes involved in the hepatic metabolism of lipids. 11,12 GLP-1 agonists exerted favorable effects on body and liver weight, liver lipid content, and plasma transaminases. 11,13,14 A clinical study showed that patients with NAFLD have increased serum DPP-4 activity, which correlated positively with the grade and degree of hepatosteatosis. 15 On the basis of these findings, we propose that inhibition of DPP-4 may help to improve both hepatic and peripheral insulin sensitivity, and DPP-4 inhibitors may be a new therapeutic approach for slowing the progression of NAFLD.
In this study, we analyzed the effect of sitagliptin, an orally active, potent, and highly selective DPP-4 inhibitor, 7 on histological improvement of NAFLD in diet-induced obese rats. We hypothesized that sitagliptin may decrease insulin resistance and associated hepatosteatosis and contribute to reducing liver fat content.
Materials and Methods
Animals and experimental protocol
Adult female Sprague Dawley rats that were 24 weeks old and weighed between 199 and 240 grams were used. All animals were obtained from Gazi University Animal Experiments Research Center. The rats were maintained in the laboratory under controlled environmental conditions (12-hr light, 12-hr dark cycle and room temperature 21°C). Rats were housed in plastic cages (2 animals per cage) and given food and water ad libitum. All animals were weighed every 10 days to determine any change in weight. The animals were cared for in accordance with protocols approved by Gazi University Animal Experiments Local Ethics Committee regulations.
All rats were randomly assigned to two groups: A control group (n=6) and a high-fat diet (HFD) group (n=18), with similar body weights (211.2±8.4 grams vs. 228.7±9.3 grams, respectively). Rats in the control group were maintained on standard rat diet (20% protein, 4% fat, 70% carbohydrates, 3% fiber, 1% vitamins, 2% mineral salt; 2,6 kcal/gram) for 16 weeks. We used a high-fat, high-calorie solid diet (HFD) for 12 weeks to create a model of insulin resistance and NAFLD. The HFD (17% protein, 34% fat, 48% carbohydrates, 0.5% choline, 0.5% mineral salt; 3.3 kcal/gram) was prepared by mixing 2 grams cholesterol and 88 grams of standard rat diet and 10 gram lard oil. 16 After 12 weeks, among rats receiving the HFD, the one with the lowest weight was sacrificed for examination of liver for hepatosteatosis. Grade 1 hepatosteatosis was observed in the lowest-weight rat receiving the HFD. Subsequently, the HFD group was randomly separated into two groups: (1) HFD-only group (n=8) was given only the HFD for another 4 weeks (fed with the HFD for a total of 16 weeks); (2) HFD-sitagliptin group (n=10) was given sitagliptin (3 mg/kg per day) via gavage for 4 weeks in addition to the HFD. The hypoglycemic dose of sitagliptin was compatible with the literature. 17
At the completion of the study, all rats were sacrificed for histopathological evaluation of liver samples at 16 weeks. Rats were anesthetized with intraperitoneal injection of xylaxine hydrochloride and ketamine hydochloride in accordance with sacrificing schedules reported in the literature. Blood samples were collected for biochemical assays. The liver was removed and weighed after rinsing with ice-cold saline and sampled for histological study.
Biochemical analyses
Blood samples were drawn from all rats to determine blood biochemical parameters (Erbil's Laboratories, Turkey), including the levels of serum glucose, triglyceride, cholesterol, and alanine aminotransferase (ALT). Plasma insulin levels were measured twice by enzyme immunoassay kit (SPI-Bio, Société de Pharmacologie et d'Immunologie-Bio, France). Fasting glucose levels were measured twice by glucometer (One Touch Horizon, Life Scan Inc. Milpitas USA, Johnson & Johnson Company). Homeostasis model assessment-insulin resistance index (HOMA-IR) was calculated as glucose (mmol/L)×insulin (μIU/L)/22.5. 18
Histological studies
At least three liver sections were examined blindly from different lobes of each rat (Gazi University, Faculty of Medicine, Department of Pathology). Liver tissues were fixed in 10% buffered formaldehyde, and then embedded in paraffin. A 4-μm-thick section cut from a paraffin-embedded block was stained with Hematoxylin & Eosin (H&E) and Masson's Trichrome. To visualize the accumulation of fat droplets, frozen liver tissue sections were stained with Oil Red O. To define fibrosis, Masson's Trichrome Technique was applied. Steatosis, necroinflammatory grade, and stage of fibrosis were assessed as previously described. All slides were viewed under the light microscope with a camera attachment. For hepatic steatosis: grade 0=no fat; grade 1=steatosis occupying less than 33% of hepatic parenchyma; grade 2=33%–66% of the hepatic parenchyma; grade 3=more than 66% of the hepatic parenchyma. For inflammatory cell infiltration: grade 0=none; grade 1=1–2 foci/field; grade 2=3–4 foci/field; grade 3=more than 4 foci/field. For ballooning degeneration of the hepatocytes: grade 0=absent; grade 1=very mild inflammation; grade 2=mild-to-moderate portal inflammation; grade 3=intraacinar inflammation and moderate portal inflammation. For hepatic fibrosis: stage 0=none; stage 1, mild=perisinusoidal; stage 2=moderate, perisinusoidal fibrosis; stage 3=periportal fibrosis; stage 4=bridging fibrosis. 19
Statistical analyses
Analyses were performed primarily by using SPSS 11.5. Data were expressed as means±standard deviation (SD). Continuous variables were tested by the Shapiro–Wilk test for normal distribution. The statistical significance was tested by one-way analysis of variance (ANOVA), with a Tukey multiple comparison posttest Student test for pairwise comparisons. Groups were compared using parametric tests (paired Student t-test or one-way ANOVA), and the Kruskal–Wallis test was used for nonparametric variables. The Student test for unpaired data was used to compare groups when normally distributed. Analysis of covariance (ANCOVA) using general linear models was used to correct for the end-of-treatment body weight modifier among groups. P values of less than 0.05 were considered statistically significant.
Results
The effect of control and high-fat diet
The rats receiving the HFD consumed significantly more calories than controls, and this was associated with a progressive increase in rat body weight compared to the control group (P<0.001) (Table 1). Serum glucose (P<0.001), plasma insulin (P<0.001) values, HOMA-IR index (P<0.001), serum triglycerides (P<0.001), and cholesterol (P<0.001) levels were significantly lower in the control group compared to the HFD-only and HFD-sitagliptin groups (Table 1). Liver weight was significantly higher in the HFD-only and HFD-sitagliptin groups compared to the control group (9.5±1.3 and 8.2±0.9 vs 6.7±1.1; P=0.001), meanwhile serum ALT levels were not different among the three groups (Table 1).
Analysis of variance.
One-way ANOVA.
Kruskal–Wallis tests, P<0.001.
HFD, high-fat diet; HOMA-IR, homeostasis model assessment of insulin resistance; ALT, alanine aminotransferase; ANOVA, analysis of variance.
Effects of sitagliptin on insulin resistance and metabolic parameters
Sitagliptin-receiving rats had a lower end-of-study body weight compared to the HFD-only group (247.9±17.0 vs. 291.3±40.7 grams, respectively; P=0.012). The HFD-sitagliptin group had significantly lower serum glucose (140.8±18.8 vs. 224.7±20.6 mg/dL, P<0.001), plasma insulin (15.8±4.4 vs. 28.0±5.9 μIU/L, P<0.001), HOMA-IR index (4.9±1.8 vs. 15.9±2.3, P<0.001), serum triglycerides (199.0±108.7 vs. 468.0±370.7 mg/dL, P<0.001), and cholesterol (82.0±26.7 vs. 90.5±7.0, P<0.001) values compared to the HFD-only group (Table 1, Fig. 1). None of the sitagliptin-receiving rats developed hypoglycemia. After adjustment for end-of-study body weight, the differences in aforementioned parameters between the two groups remained significant (serum glucose adjusted P<0.001; plasma insulin adjusted P<0.001; HOMA-IR index adjusted P<0.001; serum triglyceride adjusted P=0.02; cholesterol adjusted P=0.006).
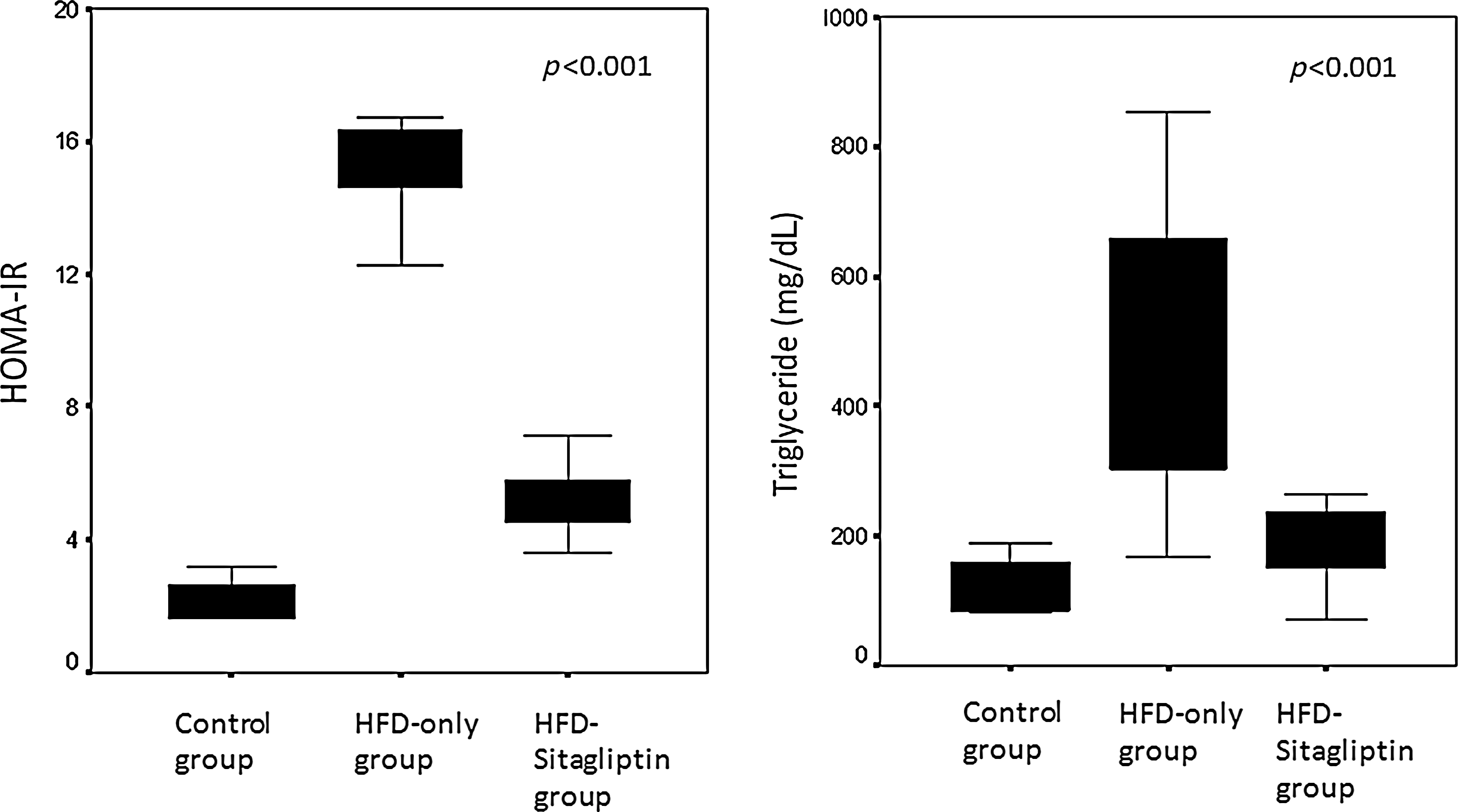
Effects of sitagliptin administration on the homeostasis model assessment of insulin resistance (HOMA-IR) index and serum triglyceride levels. HFD, high-fat diet.
Effects of sitagliptin on liver weight and biochemistry
Liver weight was similar between the HFD-only and HFD-sitagliptin groups (P=0.068). Moreover, serum ALT levels were not different in the HFD-sitagliptin group from the HFD-only group (P=0.370) (Table 1).
Effects of sitagliptin on hepatic histology
In contrast to the control group, hepatic parenchyma in the HFD group (HFD-only and HFD-sitagliptin groups) showed diffusely mixed hepatic steatosis, which was typically either macrovesicular or microvesicular, mainly involving the zone-3 hepatocytes (Fig. 2). Fat droplet accumulation was observed in sections stained with Oil Red O in the HFD-only and HFD-sitagliptin groups, but not in the control group (Fig. 2). These findings suggest that the animal model of NAFLD was successfully established. Hepatosteatosis was seen in all rats in both the HFD-only and HFD-sitagliptin groups, but the mean grade of steatosis in the sitagliptin-receiving group was significantly lower than the HFD-only group (mean score, 1 vs. 2; P<0.001) (Table 2). In the HFD-sitagliptin group, the degree of steatosis accumulated in grade-1 and no grade-3 steatosis was observed, whereas in the HFD-only group most of the rats had grade-2 steatosis and there were 2 rats with grade-3 steatosis (Table 2). After adjustment for end-of-study body weight, the difference in the degree of steatosis between groups remained significant (adjusted P<0.001).

The numbers are expressed as number of subjects.
The numbers are expressed as number of subjects and percentage.
Mild hepatic lobular inflammation was observed in the periportal field of the hepatic parenchyma in both the HFD-only and HFD-sitagliptin groups, but not in the control group (Table 2, Fig. 2). In the HFD-sitagliptin group, the rate of necroinflammation was lower compared to the HFD-only group, but that was not statistically significant (40.0% vs. 62.5%; P=0.057). Ballooning degeneration and fibrosis were not observed in any of rats (Fig. 2).
Discussion
In this study, we analyzed the effects of sitagliptin on metabolic and histological improvement of NAFLD in diet-induced obese rats. This experimental study demonstrated that sitagliptin protects the liver against steatosis by increasing insulin sensitivity and by modulating lipid profiles.
The data on the effect of DPP-4 inhibitors on NAFLD in the literature is very scarce. Mu et al. demonstrated that sitagliptin effectively ameliorates hyperglycemia and hyperlipidemia and causes dose-dependent reductions in liver weight and hepatic triglyceride content in the nongenetic rodent model on a high-fat diet. 20 In another recent study, sitagliptin decreased liver steatosis, β-cell apoptosis, and insulin resistance in fructose-fed rats with insulin resistance and metabolic syndrome. 21 Shirakawa et al. showed that in wild-type mice and a murine model of hyperglycemia due to impaired β-cell glukokinase, liver steatosis induced by diet improved, along with a reduction in hepatic triglyceride content, after sitagliptin therapy. In this study, DPP-4 inhibition decreased expressions of sterol regulatory element-binding protein-1c (SREBP-1c), stearoyl-CoA desaturase-1 (SCD1), and fatty acid synthase as well as the expressions of key gluconeogenetic enzymes as phosphoenolpyruvate carboxykinase (PEPCK) or glucose-6-phosphatase (G6Pase) in the liver while the expression of peroxisome proliferator-activated receptor-α (PPARα) was increased. 22 Since insulin resistance induces hepatic steatosis by increasing hepatic lipogenesis and gluconeogenesis, sitagliptin may lead to decreased liver fat and hepatic insulin resistance through suppression of lipogenetic and gluconeogenetic pathways.
Clinical observations on the effect of DPP-4 activity and inhibition on fatty liver is even more limited. In patients with NASH, the serum DPP-4 activity was higher than controls and correlated with the histopathological grade and hepatosteatosis. 15 Furthermore, DPP-4 immunostaining on hepatocytes correlated positively with the grade and degree of hepatosteatosis in this study. In NAFLD patients with T2DM, significant decreases in plasma glucose and serum HbA1c, aspartate transaminase (AST), ALT, and γ-glutamyl transpeptidase (γ-GTP) levels were observed after 4 months of treatment with sitagliptin. 23 These results suggest that sitagliptin may promote clinically beneficial effects on hepatic steatosis, along with improving glycemic control.
Sitagliptin, as a DPP-4 inhibitor, inhibits the breakdown of endogenous incretin hormones, 10 and the favorable outcomes on liver obtained with sitagliptin might be through increased GLP-1 levels. Experimental data suggest that GLP-1 agonists have an effect on the major pathways taking part in the generation of fatty liver. A study indicated that the GLP-1 agonist exenatide effectively stimulated insulin secretion and reduced insulin resistance and hepatic steatosis in ob/ob mice. In this study, GLP-1–exposed hepatocytes showed improved mRNA expression of PPARα genes associated with fatty acid oxidation and decreased expression of SREBP-1c and SCD1 genes associated with fatty acid synthesis. 13 Svegliati-Baroni et al. found that total fatty acid amount in hepatocytes of rats with NASH was reduced by 30% after GLP-1r activation by exenatide. 12 They also showed that in the HFD rats, PPARγ expression regulating the lipid homeostasis and insulin sensitivity and PPARα downstream genes acyl-coenzyme A oxidase 1-palmitoyl (ACOX1) and carnitine palmitoyltransferase 1A (CPT1A) expression acting on free fatty acid oxidation were decreased. Moreover, after incubation of HFD rat hepatocytes with exenatide, PPARγ, PPARα, ACOX1, and CPT1A expression increased in a dose-dependent manner. Exenatide also reduced the level of Ser307 JNK phosphorylation in hepatocytes, which normally inhibits the insulin receptor signaling. 12 Increased GLP-1 levels after adenoviral vector injection in a DIO mouse model have been associated with reduction in the expression of gluconeogenetic genes such as PEPCK or G6Pase. Additionally, some lipogenic and lipid transport genes and fatty acid–binding protein 1 mRNA were downregulated, but there was no significant effect on triglyceride synthesis enzymes and SREBP-1c. PPARγ transcripts were downregulated, whereas PPARα was not significantly affected. In this study, the pancreatic insulin content and islet cell area on histology were not affected by vector injection. Thus, the authors discuss that the improvement on glucose homeostasis cannot be attributed to increased insulin secretion alone, pointing to suppressed lipogenic gene expression as a potential mechanism. 24 Samson et al. showed that GLP-1 agonist treatment decreased FGF21 [a peptide-regulating lipid and glucose metabolism in liver and adipose tissue, potentially through the adenosine monophosphate (AMP)-activated protein kinase (AMPK) pathway] levels and reduced hepatic fat content in humans with T2DM and in a DIO mouse model. In this study, there was also a significant increase in AMPK phosphorylation in the liver, suggesting that GLP-1 analogs protect against the “hepatic FGF21 resistance” encountered in NAFLD. 25 These studies suggest that exenatide has a role in lowering the liver fat content by promoting beneficial effects on hepatic fat trafficking and gluconeogenesis. Whether these effects are mediated through the GLP-1 receptor (GLP-1r) is not clear because GLP-1r expression in liver is a controversial issue. Although several studies have reported GLP-1r expression on rat and human hepatocytes, 11 –13 there are also studies reporting no GLP-1r expression in liver. 26 –28 Receptor-independent mechanisms are suggested for the effects of GLP-1 on liver. 29
Few clinical observations support these experimental results observed with GLP-1 agonists. In a randomized controlled trial, exenatide therapy was reported to promote improvements in insulin resistance, cardiovascular risk factors such as lipid profiles and blood pressure, and liver biomarkers associated with weight reduction. 30 A case report indicated that 44 weeks of exenatide therapy decreased hepatic fat accumulation significantly, improved levels of liver enzymes, and led to significant beneficial changes in cardiovascular disease risk factors in the patient. 31 Another study showed that combined pioglitazone-exenatide therapy led to greater reduction in hepatic fat content than pioglitazone alone in patients with T2DM. 32
In the present study, sitagliptin provided significant reductions in serum glucose and plasma insulin levels and the HOMA-IR index. Therefore, improvement of hepatic steatosis by sitagliptin might be through increasing insulin sensitivity. Whether this is through increased insulin secretion due to the insulinotrophic effects of GLP-1 or insulinomimetic action of GLP-1 on insulin-sensitive tissues, as suggested by Tomas et al., or through other potential mechanisms such as glucagon suppression or antiinflammatory action of those agents is not clear. Recently, antiinflammatory effects with a significant reduction in reactive oxygen species generation and the mRNA expression of several inflammatory mediators [tumor necrosis factor-α(TNF-α), JNK-1, Toll-like receptor-2 (TLR-2), TLR-4, interleukin-1β (IL-1β), and suppressor of cytokine signaling-3 (SOCS-3)] of both sitagliptin and exenatide has been demonstrated. 33,34 Those proinflammatory mediators that are suppressed by sitagliptin or exenatide also play important roles in insulin signal transduction; thus, such an observation may uncover a potential insulin-sensitizing effect of these agents. Rizzo et al. showed that treatment with sitagliptin or vildagliptin, which is another DDP4 inhibitor, was associated with reductions in plasma IL-6, IL-18, TNF-α, and nitrotyrosine levels in association with a decrease in mean amplitude of glycemic excursions. 35 Thus, it is yet not clear if these agents have a direct antiinflammatory effect or if it is through glucose regulation.
Another explanation for improved hepatic steatosis might be through regulation of lipid profiles, because sitagliptin led to a significant reduction in serum triglycerides and cholesterol levels and caused significant weight loss in rats in our study. In clinical studies, however, sitagliptin demonstrated a neutral effect on body weight and lipid profiles. 36,37 We suggest that this conflict might be due to a species difference, and this effect might be observed only in rat models of NAFLD. In our study, the favorable effect of sitagliptin on hepatic steatosis and metabolic parameters was independent of weight change. However, taking into consideration that the body weight has a tight relationship with hepatic steatosis and the metabolic parameters studied, it is difficult to speculate that those beneficial effects are caused by sitagliptin only. There is evidence in the literature in favor of a weight-independent action. Vildagliptin, which is another DPP-4 inhibitor, was associated with a significant reduction in levels of plasma cholesterol in the HFD mice without changing body weight. 38 In the study of Shirakawa et al., the protective effects of sitagliptin on adipose tissue and liver were observed before a significant difference in body weight occurred, suggesting that these effects may not be fully explained the decreased body weight alone. 22 In this study, although sitagliptin led to a reduction in body weight, it did not affect liver weight, which is similar to our findings. We would have expected proportionate lower liver weight in the sitagliptin-treated group in our study. We suppose that the HFD-sitagliptin group had a trend toward a lower liver weight, but possibly due to the short duration of intervention or small sample size that was not statistically significant.
In the current study, sitagliptin had no effect on improvement of hepatomegaly and liver transaminase levels. These results might be due to the small sample size and insufficient time for evaluation of sitagliptin effect on hepatomegaly, because it was limited to only 4 weeks. Although sitagliptin was shown to improve hepatic steatosis in the present study, it did not significantly reduce hepatic necroinflammation. Because ballooning degeneration and fibrosis were not observed in any of the rats, we did not examine these parameters in this study. The issue is complicated by not only the short duration of the study but also by the small number of subjects. Larger clinical long-term trials are needed to determine effects of sitagliptin on hepatic necroinflammation, ballooning degeneration, and fibrosis.
In conclusion, we propose that sitagliptin protects against hepatic steatosis by increasing insulin sensitivity and by promoting favorable lipid profiles in a rat model of NAFLD and metabolic syndrome. Therefore, sitagliptin might be a novel therapeutic option for slowing the progression of NAFLD. Clinical studies have reported that DPP-4 inhibitors can be used safely without hypoglycemia, even in nondiabetic patients, 39 which is in accordance with the findings of our study. Thus, sitagliptin could be used without significant adverse effects in diabetic and even in nondiabetic patients with NAFLD. Before using sitagliptin in clinical treatment of NAFLD, randomized controlled trials based on hepatic histology should be undertaken.
Footnotes
Acknowledgments
This research was funded by the researchers, who did not receive any specific grant from any funding agency in the public, commercial, or not-for-profit sector.
Author Disclosure Statement
No competing financial interests exist.