
Abstract
Background:
Prader-Willi syndrome (PWS) is a genetic disorder characterized by morbid obesity resulting from insatiable appetite. Complications like diabetes mellitus or other cardiovascular diseases typically occur during lifetime. Lifestyle advice and education as well as limited caloric intake are the major concepts in assistance of PWS patients.
Methods:
A 12.9-month follow-up study, which included 8 formerly genetically diagnosed PWS patients, was conducted. Physical and laboratory examinations were done at the beginning and at the end of the follow-up. Improved medical care and lifestyle advice were given. The participants lived in an assisted living environment with a fixed daily schedule and limited caloric intake.
Results:
The group of patients consisted of manifest diabetics (n=6) as well as nondiabetics (n=2). Therapeutic concepts were simplified in 2 patients by switching from insulin to oral antidiabetics. The reduction in body weight was moderate, but attributable to a loss of fat mass. A significant reduction in blood cholesterol and triglyceride content was achieved along the observational period as well as a significant reduction of glycosylated hemoglobin (HbA1c) in the group of diabetic PWS patients. Systolic blood pressure improved during the study.
Conclusion:
A combination of an assisted living environment following conservative treatments as well as consistent patient care improved the daily and medical situation of PWS patients. Weight loss and, as a consequence, improvements in terms of metabolic condition and blood pressure were observed. A combination of medical and daily routine management should be established in PWS patients to improve their quality of life.
Introduction
The aim of this survey was to show the effect of the nutritional, medical, psychological, and pedagogical concepts on the development of body weight and cardiovascular risk factors in this population.
Methods
Eight adults (31.4±6.4 years, 5 males, 3 females) with a PWS diagnosis confirmed by genetic testing who live in an assisted living environment took part in this follow-up observation. At study entry, the nutritional concept consisted of a 1500 kcal/day diet; the patients were advised to do sports at least twice a week for 60 min and to take part in a structured intensive pedagogic care. The subjects were living for 7.6±2.2 years before study entry in the assisted living environment. There were 5 regularly working days per week with a scheduled time plan. On these days, residents worked in a sheltered workshop for at least 35 h per week. The patients had spare time on the weekend (Saturday and Sunday).
Two medical surveys, in which body mass index (BMI), blood pressure (RR), and laboratory values for glycosylated hemoglobin (HbA1c), metabolic parameters like low-density lipoprotein (LDL), high-density lipoprotein (HDL), and triglycerides were determined, took place. As markers for the underlying atherosclerotic situation, carotid duplex was performed and intima media thickness (IMT) was determined (LOGIC7Pro, 7L, GE Healthcare, Buckinghamshire, UK). Longitudinal and transversal scanning of the aorta carotis communa, aorta carotis externa, and aorta carotis interna was performed to evaluate atherosclerotic risk in terms of plaques or stenosis. In a second measurement, IMT of the aorta carotis communis was determined ∼1 cm proximal of the carotid bifurcation. In a third measurement, the aorta vertebralis was examined to determine flow disturbances. The visits took place within 12.9±1.5 months at the endocrinology service of the Diabetes Center at the Heart and Diabetes Center NRW in Bad Oeynhausen.
For patients in whom diabetes was not diagnosed, an additional oral glucose tolerance test (OGTT) was performed to exactly evaluate the metabolic state. BMI and drug history at the entry in the specialized residential group and during this evaluation period were available. By using bioelectrical impedance analysis (TANITA TBF410M, Tokyo, Japan), the basal metabolism, the body lean mass, and body fat were determined at the beginning and at the end of the evaluation period.
The study was reviewed by the ethics committee of the Ruhr-University Bochum in Bad Oeynhausen and conducted in accordance with the Declaration of Helsinki. The supervisors and the patients were informed about the scope and significance of the observation and agreed in writing (informed consent).
All values are presented as means±standard deviation (SD). Statistical analysis was done using paired t-tests, and p values <0.05 were regarded as statistically significant.
Results
Eight persons whose characteristics are listed in Table 1a and 1b took part in the study. They had been living in the residential group for about 7.6±2.2 years at the beginning of the survey (=study entry). Their basal metabolism was 1.692±171 kcal. Six people of the study population had suffered from diabetes since the beginning of the first survey; diabetes treatments are listed in Table 2.
BMI, body mass index; M, male; F, female; HbA1c, glycosylated hemoglobin; TSH, thyrotropin; RR, blood pressure; IMT, intima media thickness.
q.d., once daily; b.i.d., twice daily; t.i.d., three times a day.
Two residents were taking antihypertensive medications; none of them had taken lipid-lowering medication (Table 2). Of the male subjects, 2 persons received testosterone supplementation and 2 of 3 female participants received estrogen supplementation.
Body mass index
Weight reduction could be shown within the time interval of the survey. BMI decreased by more than one unit from 29.9±4.8 kg/m2 to 28.7±4.1 kg/m2 (P=0.10). On average the patients lost 1.8±4.0 kg weight from the first to the second survey (time elapse 12.9 months). A significant weight reduction was detected from the time of the entry in the residential group until the time of the first examination, which is described as first survey in this manuscript. BMI was lowered from 38.1±7.4 kg/m2 to 29.9±4.8 kg/m2 (P<0.05) (Fig. 1).
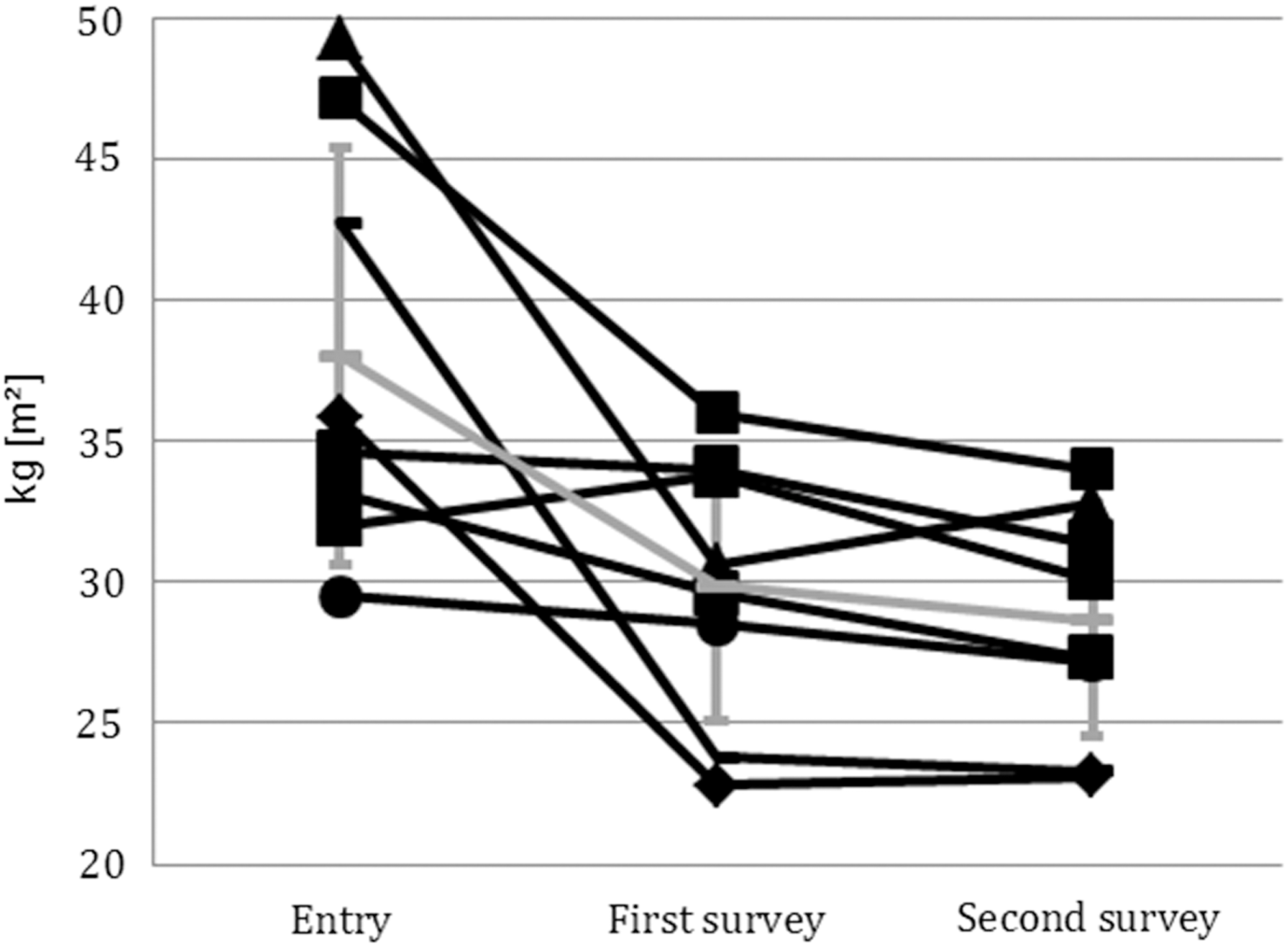
Developing of body mass index (BMI) during life in assisted living and after start of the survey. Each square represents 1 individual; the trend is given in gray, means±standard deviation (SD).
During the survey, the fat proportion could be reduced from 27.1±8.9% to 25.2±8.1% (Fig. 2). There were no changes in the lean mass (from 57.0±7.4 kg to 57.1±8.1 kg). Thus, the improvement in BMI is attributable to the loss of fat mass.
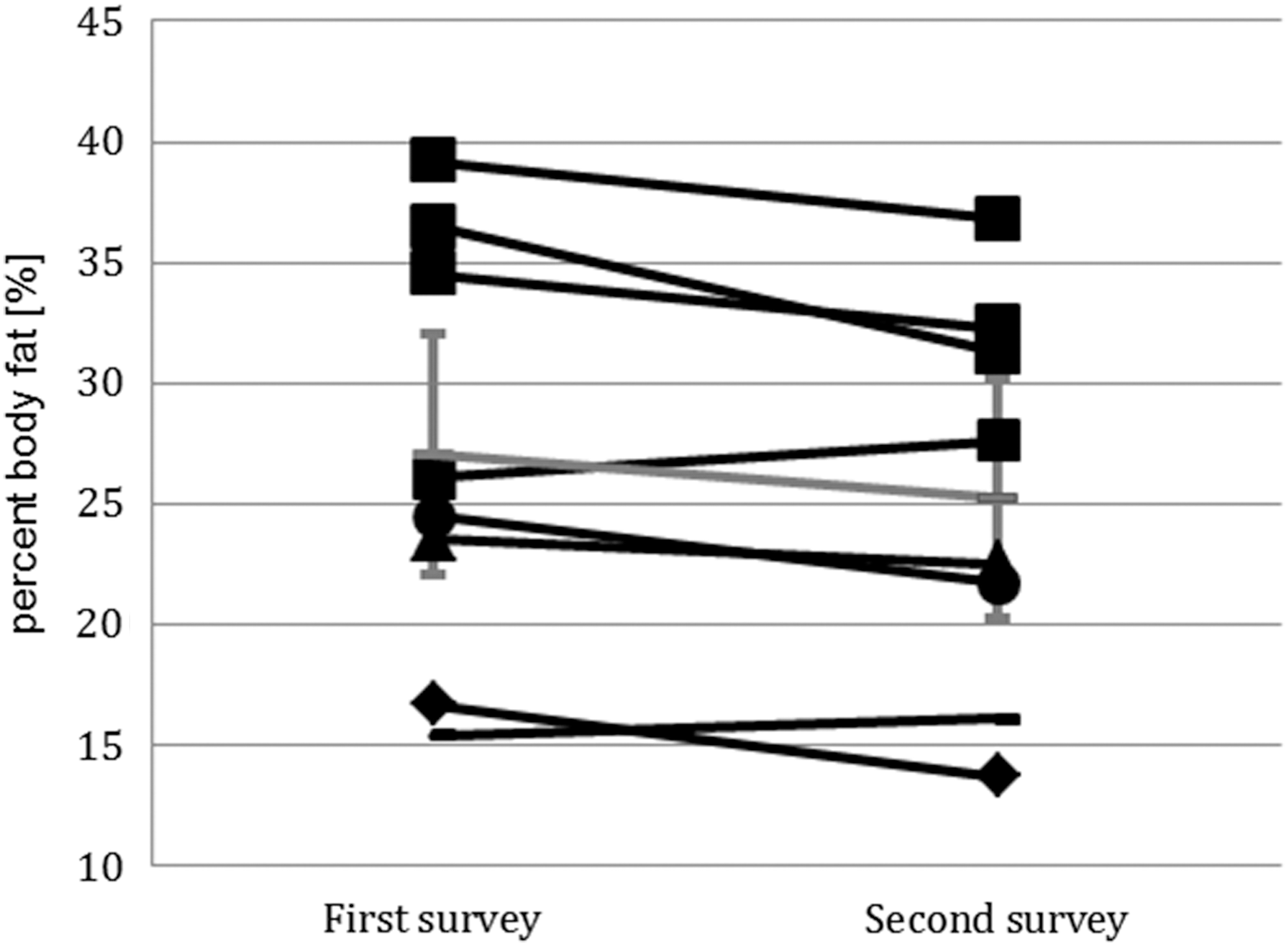
Development of fat proportion during life in assisted living after the start of the survey measured by bioelectrical impedance analysis. Each square represents 1 individual; the trend is given in grey, means±standard deviation (SD).
Diabetes mellitus type 2
Two persons were tested by using OGTT for diabetes; both were negative at enrollment, and 1 subject developed impaired glucose tolerance during follow-up. Regarding the persons with diabetes, a significant reduction in HbA1c was achieved during the survey (6.5–6.0%, P<0.05) (Fig. 3, Table 1b). Mild hypoglycemia was reported by 1 person, and antidiabetic medication was adapted. Common antidiabetics were oral antidiabetics (metformin, repaglinid, sitagliptin) or for 1 person in combination with insulin. For a detailed overview, please refer to Table 2. The oral therapy was intensified during the observation period. Metformin therapy was initiated for 1 patient. During the stay in the assisted living group, the number of diabetics requiring insulin for glycemic control could be reduced from 3 to 1 subject during the stay in the group.

Development of glycosylated hemoglobin (HbA1c) during life in assisted living after start of the survey. Each square represents 1 individual; the trend is given in gray, means±standard deviation (SD).
Cholesterol and triglycerides
There were significant changes for the blood fat laboratory values. The triglycerides decreased from 111.3±50.3 mg/dL in the first to 97.9±46.2 mg/dL in the second examination of the survey. Total cholesterol decreased from 187.4±32.3mg/dL to 177.9±27.5 mg/dL. HDL-C changed slightly from 46.6±14.0 mg/dL to 44.9±10.2 mg/dL, but the LDL-C was lowered from 125.5±19.3 mg/dL at the first and 115.3±30.6 mg/dL at the second examination. For 2 people, a statin therapy was initiated at the first examination.
Blood pressure
The systolic blood pressure changed from 122.5±8.2 mmHg at the first and 117.1±8.9 mmHg at the second examination. The diastolic blood pressure rose from 75.3±6.5 mmHg to 79.1±10.9 mmHg. These changes were not significant. An antihypertensive medication with an angiotensin-converting enzyme (ACE) inhibitor was started with 1 person. For another person, antihypertensive medication with an ACE-inhibitor was adapted (dose increase).
Carotid duplex
At both examinations at survey start and follow-up, no stenosis or plaques were detectable. The number of persons with an age-specific borderline IMT rose from 4 persons at the first examination to 5 persons at the second examination.
Discussion
This survey clearly demonstrates that a scheduled daily plan, including occupation and sports, a restriction of caloric intake, and psychological support is useful for the management of PWS. People with PWS clearly benefit from an assisted life in a group. The concept of living in a group rather than in the familiar environment proved to be of advantage in terms of physiologic and psychological health. The survey done in this group of patients was able to show a further improvement of the clinical situation of the subjects. The close medical guidance throughout their life was helpful and obligated treatment of metabolic diseases to prevent late complications that are triggered by obesity and diabetes mellitus. Effective weight reduction was achieved, and weight gain during the survey could be prevented by lifestyle intervention. The loss of weight was mainly due to the reduction of body fat detected by bioelectrical impedance analysis. Although this measurement has several limitations, we can assume that caloric intake in combination with lifestyle modification has beneficial effects in terms of reduction of fat mass. Keeping body weight on a constant and tolerable level should be regarded as success in PWS patients. Regarding the fatty acid metabolism, the dietary concept shows that the caloric limitation not only resulted in weight reduction but also resulted in an improvement of blood pressure. The fact that statin therapy had to be started in 2 patients may be in correlation with diabetes duration and previous or ongoing insulin therapy.
The use of glucagon-like peptide-1 (GLP-1) mimetics and dipeptidyl peptidase-4 (DPP4) inhibitors has been discussed with regard to weight management and HbA1c control in PWS patients to avoid or replace insulin therapy. 12 The effects on satiety and glucose levels should lead to an improvement of the metabolic situation. To conclude, the primary goal of treating PWS patients should be increasing life quality and prevention of late complications. Weight management serves both goals and is therefore the primary objective in this context. The assistance in a group instead of individual therapy proved to be of benefit for PWS patients regarding mental and medical health.
Limitations of the study
This data evaluation and medical follow-up of subjects who lived in an assisted environment was started years after the persons started living in the group. Effects of caloric restriction were much more pronounced if entrance in the group is compared to our first survey. Nevertheless, an improvement in terms of body weight, diabetes medication, and some metabolic parameters was achieved, although the persons lived for more than 7 years in this group during our two surveys with a time span of about 13 months. Data from a control group (e.g., familiar environment instead of assisted living) are not available. These data may be highly individually different and thus are not comparable to our group of persons having lived in the group for some years.
Footnotes
Acknowledgments
The authors would like to thank Karin Fruend and Ulrike Strauhs for their assistance regarding the nutritional concept of this study.
Author Disclosure Statement
All authors have no competing interests or conflicts of interest regarding the topic of this manuscript to declare.