
Abstract
Background:
Previous reports showed a high prevalence of obesity, diabetes, hypertension, and dyslipidemia among people suffering from posttraumatic stress disorder (PTSD). However, there is a lack of reviews that systematically analyze the relationship between PTSD and metabolic syndrome. We conducted a systematic review and meta-analysis aimed at estimating the association between PTSD and metabolic syndrome.
Methods:
We systematically searched PubMed, Embase, and Web of Science. We included observational studies assessing the prevalence of metabolic syndrome in a sample with PTSD and in a comparison group without PTSD. Data were analyzed using Review manager 5.1. Odds ratios (OR) with 95% confidence intervals were used as an association measure for pooled analysis, based on a random-effects model.
Results:
Six articles were eligible according to the inclusion criteria, for an overall number of 528 individuals suffering from PTSD and 846 controls without PTSD. The pooled OR for metabolic syndrome for people with PTSD was 1.37 (1.03–1.82). Statistical heterogeneity between the included studies was low (I 2=22%).
Conclusions:
Despite some limitations, the findings of this systematic review and meta-analysis confirmed our hypothesis that individuals suffering from PTSD have a greater risk of metabolic syndrome. The potential role of unknown factors or mediators that might clarify the nature of this association needs further research.
Introduction
Methods
The present systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement. 29
Search strategy
We used the PubMed (date range, January 1, 1990, to January 3, 2013), Web of Science (date range, January 1, 2002, to January 3, 2013), and Embase (date range, January 1, 1990, to January 3, 2013) electronic databases for search purposes. No language restrictions were applied. We used search phrases combining the terms “Metabolic Syndrome” and “Post-Traumatic Stress Disorder.” We further hand-searched reference lists of all included studies and of a recent relevant review 30 to ensure a comprehensive coverage.
Eligibility criteria
We included studies with the following characteristics: (1) Estimation of the prevalence of metabolic syndrome in a sample of people suffering from PTSD; (2) additional available data on prevalence of metabolic syndrome in a comparison group without PTSD; and (3) recruitment of samples made by at least 95% of individuals aged ≥18 years. We excluded studies if selected groups with other psychiatric diagnoses were used as comparison. If the data from the same sample were published in multiple works, we retained for meta-analysis only the study with more complete information to avoid duplicate results.
Data collection process
Preliminary screening was conducted by reading titles and abstracts. The final eligibility was assessed retrieving the full text of paper. We built a data extraction template, including for all eligible studies key items based on year of publication, country, study design, sample size, methods to assess PTSD and metabolic syndrome, and main results. We also collected information suitable for a basic quality evaluation of studies. We evaluated if the recruited sample was representative of general population suffering from PTSD or if special groups (e.g., war veterans) had been selected. We checked if PTSD was properly assessed using standardized diagnostic interviews. We assessed adequacy of the recruitment of comparison samples without PTSD, testing if they came from the same population that gave rise to the cases. We further tested if metabolic syndrome was correctly diagnosed using standardized diagnostic criteria [e.g., National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III), 31 American Heart Association/National Heart, Lung, and Blood Insitute (AHA/NHLBI) 32 ]. Finally, we evaluated if the studies included showed further analyses on the association between metabolic syndrome and PTSD, controlling for factors potentially associated with metabolic syndrome (e.g., age, gender, depression co-morbidity, antipsychotic medication).
Data analysis
We analyzed data using the Review Manager (RevMan) 5.1 software. 33 The pooled analysis was based on odds ratios (ORs) with related 95% confidence intervals (CI), according to available data from included papers. Results were summarized using conventional forest plots. The pooled estimate was obtained weighting each study, according to the inverse of its variance, following a random effects model for meta-analysis, which includes both the within-studies and the between-studies variances. This model considers both the variance of effect sizes and the variance of sampling error. We used a random effects rather than a fixed-effect model for pooled estimates because high variability across the included studies in relation to inclusion/exclusion criteria, setting, PTSD, and metabolic syndrome definitions was expected. The presence and the level of heterogeneity were assessed using a Q test and I 2 statistic, respectively. We carried out a sensitivity analysis including only more reliable data, according to the quality assessment. We visually inspected the risk of publication bias creating the RevMan funnel plot. We performed an Egger test for the statistical estimation of publication bias.
Results
Study selection
A total of 32, 35, and 73 records were generated from PubMed, Web of Science, and Embase databases, respectively. The preliminary screening based on titles and abstracts identified 17 papers as potentially relevant. The full text of these papers was retrieved. Among these, 11 were excluded because they did not meet inclusion criteria. Detailed reasons for ineligibility are shown in flow diagram (Fig. 1). Six studies 34 –39 were included for meta-analysis; all had data suitable for the pooled estimation of the OR.
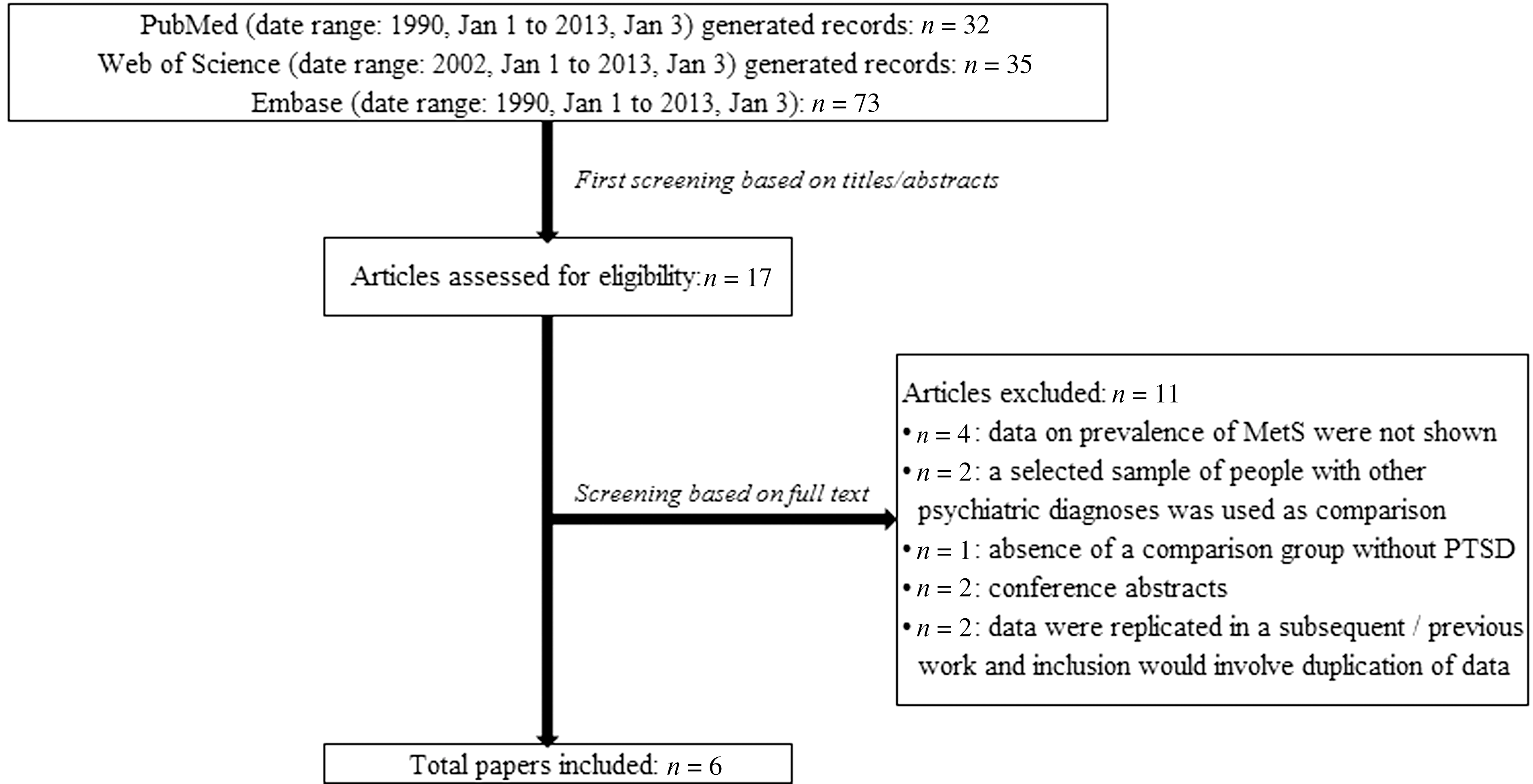
Flow diagram of search results. PTSD, posttraumatic stress disorder.
Study characteristics
All articles were in English. The years of publication ranged from 2006 to 2011. Four papers were from the United States and two were from Europe (both from Bosnia and Herzegovina). Four studies were based on samples of war veterans. Detailed characteristics of included papers are described in Table 1.
PTSD, posttraumatic stress disorder; WHR, waist-to-hip ratio; WC, waist circumference; BMI, body mass index; FBG, fasting blood glucose; TGs, triglycerides; HDL, high-density lipoprotein; SBP, systolic blood pressure; DBP, diastolic blood pressure.
OR of metabolic syndrome among people suffering from PTSD
Included studies (n=6) involved 1,374 subjects, 528 with PTSD and 846 from the comparison samples. As a whole, 192 cases of metabolic syndrome were detected from the PTSD sample and 241 from people without PTSD. The pooled OR (95% CIs) for metabolic syndrome in people suffering from PTSD was 1.37 (1.03–1.82) (Fig. 2). A low level of heterogeneity was found (P=0.27; I 2=22%). Figure 3 displays the funnel plot for publication bias. The Egger test was not statistically significant [bias coefficient, −0.71 (−7.70–6.27); P=0.79].

Forest plot: odds ratio of metabolic syndrome in people suffering from posttraumatic stress disorder (PTSD). CI, confidence interval.

Funnel plot for publication bias.
Quality assessment and sensitivity analysis
Most of included papers were prone to some relevant methodological issues and potential risk of bias. All studies analyzed samples, not representatives of general population suffering from PTSD. Four studies 34 –37 investigated the association between PTSD and metabolic syndrome in the special population of war veterans. Violanti and colleagues 38 recruited a stratified sample of police officers randomly selected from the Buffalo, NY, Police Department. Weiss and colleagues 39 selected subjects from waiting rooms in multiple primary care clinics at Grady Memorial Hospital, Atlanta, GA, a publicly funded hospital primarily serving individuals of low socioeconomic status. Furthermore, the response rate was very low.
Regarding the assessment of PTSD, Jakovljevic and colleagues 35 used properly Structured Clinical Interview for DSM-IV (SCID) for PTSD diagnosis. Two studies 34,39 integrated the PTSD Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) clinical diagnosis with Clinician Administered PTSD Scale (CAPS). The CAPS is a structured interview with excellent psychometric properties that provides a diagnosis of PTSD and can also be used as a continuous measure of PTSD symptoms. 40 Two studies 36,38 used the Impact of Event Scale (IES) to detect PTSD. However, IES is reliable for the assessment of frequency and severity of PTSD symptoms, e.g., intrusion, avoidance, and arousal, but is not suitable for a diagnosis of PTSD. Last, one study 37 was based just on a clinical evaluation of PTSD, introducing a potential risk of misclassification bias.
Two studies 35,37 selected their control groups from different sources as compared with cases. Jakovljevic and colleagues 35 recruited PTSD subjects from a clinical hospital and the comparison sample from people who attended a family medicine dispensary. Maslov and colleagues 37 recruited PTSD inpatients and outpatients and healthy volunteers and first-degree relatives of patients suffering from schizophrenia as comparison subjects. Therefore, both studies had a great risk of low degree of comparability between index cases and controls.
The metabolic syndrome assessment was limited by methodological issues in two studies. Jakovljevic and colleagues 35 declared that high-density lipoprotein (HDL) values were not determined. A low HDL value is one of the five criteria of metabolic syndrome according to the main clinical definition. 31,32 Therefore the real rate of metabolic syndrome might have been misclassified. Linnville and colleagues 36 replaced the measure of the waist circumference, which determines the presence of abdominal adiposity, with a body mass index (BMI) cutoff ≥30, introducing a potential risk of slight underestimation for this criterion and, consequently, of metabolic syndrome. Indeed, the BMI equivalent for the abdominal obesity criterion should be >28.8 kg/m2, according to previous evidence. 41,42
Most of included studies provided analyses controlled for potential confounders. The study of Heppner and colleagues 34 examined the impact of PTSD on metabolic syndrome using a logistic regression model, which included several potential predictors of metabolic syndrome, such as age, race, gender, years of education, nicotine abuse, substance abuse, alcohol abuse, and major depressive disorder. The CAPS total score for PTSD severity was a significant predictor of metabolic syndrome in the model, with risk increasing one percentage point for each unit on the CAPS (Wald=4.76, P=0.03, OR=1.01). Linnville and colleagues 36 performed a regression model, which could not support the role of PTSD in terms of metabolic syndrome predictor consistently with the relevant univariate analysis. The study of Violanti and colleagues 38 provided both age-adjusted and multivariable-adjusted (for age, education, smoking, and alcohol intake) prevalence ratios of metabolic syndrome based on PTSD severity. The study of Weiss and colleagues 39 assessed the contribution of PTSD to metabolic syndrome while controlling for other predictor variables that might have moderated the relationship (age, sex, race, smoking history, antipsychotics, trauma exposure, and major depressive disorder). The analysis showed that only a diagnosis of PTSD (Wald χ2=7.40, P=0.0065) remained a significant predictor of metabolic syndrome. Finally, no controlled analyses were shown in the studies of Jakovljevic and colleagues 35 and Maslov and colleagues. 37 The synthetic overall evaluation of quality items is illustrated in Table 2. The sensitivity analysis including only more reliable data, 34,39 according to the quality assessment, showed an OR of 1.58 (1.06–2.35) (P=0.03; I 2=0%).
Sample representative of general population suffering from posttraumatic stress disorder (PTSD).
Standardized diagnostic interview for PTSD.
Comparison sample not suffering from PTSD recruited from the same source population.
Standardized diagnostic criteria for metabolic syndrome.
Analyses controlled for confounders and factors potentially associated with metabolic syndrome.
Discussion
Summary of findings
To our knowledge, this is the first meta-analysis that systematically synthesizes data from studies comparing the risk of metabolic syndrome between individuals with and without PTSD. PTSD has an important bearing on the chances of suffering from metabolic syndrome, with an OR of 1.37 (1.03–1.82). The result is confirmed by the sensitivity analysis based on the quality assessment showing an OR of 1.58 (1.06–2.35). Therefore, our hypothesis that people suffering from PTSD had a high risk of metabolic syndrome is confirmed. This result is consistent with the findings of previous systematic reviews and meta-analyses showing high rates of metabolic syndrome among individuals suffering from severe mental illnesses. 18,20,43,44 A recent meta-analysis of 27 studies reported a crude OR between depression and metabolic syndrome of 1.42 (95% CI 1.28–1.57; I 2=55.1%). 20 A further meta-analysis of people suffering from bipolar disorder revealed a stronger association with metabolic syndrome. 44 Bipolar patients had an overall metabolic syndrome rate of 37.3% (36.1–39.0) and, if compared with general population groups, a consistently higher metabolic syndrome risk (OR=1.98; 95%CI 1.74–2.25).
Strengths and limitations
The well-known advantage of a meta-analysis of observational studies is that it allows the synthesis of results from a larger amount of studies, providing findings more robust than those deriving from data of individual studies. Observational studies are an important source in epidemiological research, but they are prone to many methodological issues. 45,46 Therefore, we paid critical attention to the quality of included papers. Some studies had several methodological limitations on important items, such as the representativeness of recruited samples, the comparability between index cases and controls, and the risk of exposure or outcome misclassification. All of these factors decreased, at least partially, the confidence in results. The effect size of association may be slightly different from the estimated one. However, the sensitivity analysis based on best-quality data confirmed the statistical significance of the association.
The published literature on PTSD and metabolic syndrome is limited. We identified just six studies with data suitable for meta-analysis, involving an overall number of 528 subjects suffering from PTSD. Most of studies analyzed metabolic syndrome rates from veterans' populations suffering from war trauma. The restricted number of papers for analysis did not allow exploring the variations of OR across subgroups analyses based on specific characteristics of included data (e.g., sample characteristics, sample size, assessment of PTSD, diagnostic methods for metabolic syndrome, geographical area). Further research based on large sample sizes examining the risk of metabolic syndrome also among PTSD individuals suffering from traumas other than war, e.g., accidents, violence, sexual abuse, is actually needed.
Available data were not sufficient for supplementary analyses testing the different rates of the five components of metabolic syndrome among people suffering from PTSD as compared with individuals without PTSD. In fact, there were no studies showing relevant dichotomous data of metabolic syndrome components among people with and without PTSD, whereas only three 34,36,39 out of six studies provided at least continuous data. Therefore, it was not possible to clarify which metabolic component had the greatest weight in determining the high rate of metabolic syndrome among people with PTSD. However, it is important to point out that reported values of metabolic syndrome components did not appear higher among individuals suffering from PTSD as compared with subjects without PTSD. For example, in the study of Weiss et al., 39 although PTSD was significantly associated with metabolic syndrome, there were no differences in waist circumference, fasting glucose, triglycerides, blood pressure, and HDL-cholesterol (HDL-C) mean values. Similarly, the studies of Heppner et al. 34 and of Linnville at al. 36 showed comparable values of metabolic syndrome parameters, apart from diastolic blood pressure and fasting triglycerides, respectively, which were higher among people suffering from PTSD. This inconsistency should be addressed and clarified by future research. Moreover, it should be noted that our findings might be affected by differences in chosen metabolic syndrome diagnostic criteria across studies. Homogeneous cut points for all components except waist circumference (which is more appropriately set at a regional level) should be used as recommended by major scientific associations statements. 47 Future research on people with PTSD might use this rigorous set of diagnostic criteria of metabolic syndrome.
Our systematic review included only published studies with sufficient data, excluding conference abstracts, because these often cannot give reliable information on patients' characteristics, inclusion criteria, assessment of outcome, and other relevant issues. The search of comprehensive databases, such as PubMed, Embase, and Web of Science, as well as the hand searching of references lists of included papers and a relevant recent review, 30 have largely granted an extensive coverage of published literature on the topic. However, we need to consider the risk that an amount of negative or uncertain results remained unpublished. Although the funnel plot visual inspection and Egger test showed the lack of risk of publication bias, we cannot exclude that this result was due to chance, as included articles were less than 10. 48
Clinical perspective
The findings of this systematic review and meta-analysis emphasize the relevance of an ongoing cardiometabolic assessment in the PTSD population. Clinicians should regularly assess metabolic syndrome in people suffering from PTSD. The ascertainment of medical co-morbidity and lifestyle habits, weight, or waist circumference and blood pressure measures, and a regular blood examination of fasting glucose and lipids should become a key part of long-term routine monitoring of these patients. However, the nature of the PTSD and metabolic syndrome co-occurrence remains unknown. Individuals suffering from PTSD may be more prone than the general population to metabolic risk behaviors. A recent systematic review highlighted that a number of health behaviors, including excessive alcohol use, smoking, low physical exercise, low self-care, and great caloric intake, may contribute to the increased risk of cardiovascular and metabolic diseases in people with PTSD. 49
It should be noted that at least three further factors may explain or mediate this association. The first factor may be the increased off-label use of antipsychotics for the treatment of subjects with PTSD. 50 Metabolic side effects of second-generation antipsychotics are related to the increase of a series of abnormalities, such as weight gain, hyperglycemia, and dyslipidemia. 51,52 Only Weiss and colleagues 39 highlighted the data on the antipsychotic medication, showing that the association between current PTSD and metabolic syndrome was not due to the use of antipsychotic drugs (Wald χ2=0.79, P=0.38). Therefore, our meta-analysis is not suitable for investigating the influence of antipsychotic agents on metabolic profile due to the lack of available relevant information. The burden of atypical antipsychotics on metabolic syndrome prevalence among individuals with PTSD should be further analyzed. Second, PTSD symptom levels and co-morbidities, similar to other severe mental illnesses, 53,54 may play an important role. Some studies have shown that PTSD people with a co-occurrent depressive disorder or a higher score of PTSD symptoms may have a greater risk of metabolic syndrome than PTSD people without these specific features. 55 –57 These findings suggest that the most severe forms of PTSD may be related to an increased risk of metabolic syndrome, regardless of the type of antipsychotic drug prescribed. The third factor may be related to the burden of stress on metabolic modifications. 58 Recent findings have highlighted that stressful life events were associated with insulin resistance, obesity, and dyslipidemia, and may be an indicator for poor metabolic health. 59 Therefore, metabolic syndrome may be a consequence of neuroendocrinal adaptations to chronic stress.
Conclusions
In summary, despite some limitations, the results of present meta-analysis highlight that individuals suffering from PTSD have a greater risk of metabolic syndrome. The potential role of unknown factors or mediators that might clarify the nature of this association deserves additional investigation. Furthermore, future research should assess longitudinally the impact of screening, prevention, and treatment measures on individuals suffering from PTSD in terms of improvement of health status and life expectancy.
Footnotes
Acknowledgments
We thank Prof. Miro Jakovljevic for providing us important information and clarification on relevant data of his articles, and all authors of the included papers.
Author Disclosure Statement
The authors declare that no competing financial interests exist.