
Abstract
Background:
High-sensitivity C-reactive protein (hsCRP) is an important biomarker of risk for coronary heart disease morbidity and mortality. We investigated the influence of short-term cardiac rehabilitation (CR) after acute myocardial infarction (AMI) on values of hsCRP and classical risk factors, including metabolic syndrome.
Methods:
hsCRP and classical risk factors were measured before and after completed 2-week CR program in 30 men after AMI. The comparison group comprised 30 age-balanced healthy men, with no risk factors for coronary heart disease.
Results:
As expected, in comparison to healthy individuals, patients had higher values of hsCRP; furthermore, smokers had significantly higher hsCRP values than nonsmokers. Patients had more expressed markers of metabolic syndrome and due to pharmacological therapy lower blood pressure, total cholesterol and low-density lipoprotein cholesterol (LDL-C). After CR was completed, a significant drop in hsCRP (P=0.006) and improvement of metabolic syndrome parameters (lower body mass index, blood pressure, LDL-C, triglycerides) was observed in nonsmokers, whereas no such changes occurred in smokers.
Conclusions:
Our study revealed that hsCRP and metabolic syndrome parameters can be substantially reduced by a 2-week CR program; however, this effect is present only in nonsmokers. Thus, all patients entering the CR program after AMI should be advised to quit smoking before entering the program to achieve optimal benefits.
Introduction
C
Although increased chronic low-grade inflammation measured by hsCRP might be genetically determined, 7,8 there are also several pharmacological and nonpharmacological measures, such as regular physical activity, optimized body weight, and smoking cessation, that might reduce hsCRP and thus lower the risk of CAD. 9
The latest data show that there is no ideal pharmacological or nonpharmacological intervention that effectively cures chronic inflammation. 10,11 Considering this, it seems extremely important to find integrated directives that combine optimal pharmacological treatment with nonpharmacological interventions to reduce chronic low-grade inflammation (accordingly, values of hsCRP), particularly in secondary prevention of CAD in patients after AMI.
It is already known that physical activity decreases chronic inflammation and that the extent of inflammatory markers' reduction depends also on the type of the activity. 12 There is unfortunately no current data about the effect of routine, insurance-based, short-term (2 weeks), postmyocardial cardiac rehabilitation (CR) in Slovenia on either classical risk factors or inflammatory markers. Therefore, the primary aim of our study was to explore the possible influence of short-term CR on hsCRP in patients already on optimal pharmacological therapy shortly after AMI. The secondary aim, if the first one has been reached, was to show how these changes of hsCRP are associated with classical risk factors, markers of metabolic syndrome, smoking status, and exercise capacity.
Material and Methods
Patients
Thirty male patients with the median age of 58 years (minimum 40 years, maximum 73 years) discharged from the hospital at least 2 weeks and not more than 9 weeks after AMI were included in our randomized study. All patients after AMI were optimally treated according to current guidelines. 13
All patients were on acetylsalicylic acid 100 mg daily (combined with clopidogrel in five patients, prasugrel in 14, or ticagrelol in 10 patients for a year after AMI), angiotensin-converting enzyme or angiotensin receptor blockers, and statins. All patients were treated with appropriate statin doses (24 of them were receiving rosuvastatin and 6 of them atorvastatin), so that the target values recommended by the European Society of Cardiology (ECS) were met. All but three patients were taking beta-blockers or ivabradine. The patient group consisted of 16 smokers and 14 nonsmokers. We defined nonsmokers as patients who never smoked or stopped at least a year before AMI occurred (most of them had quit smoking many years before AMI occurred). We sorted out the patients to groups of equivalent statin doses, and no statistically significant differences were seen in equivalent doses of statins between smokers (2 patients were receiving atorvastatin and 14 rosuvastatin) and nonsmokers (4 patients were receiving atorvastatin and 14 rosuvastatin) (P=0.951). Patients were successively recruited from the standard short-term (2-week) CR program. In Slovenia, such a CR program is funded by the national insurance company for all patients after AMI. Its aim is to improve patients' physical performance and educate them about prevention of further disease progression, emphasizing the importance of taking medicines and making changes in their lifestyles.
Exclusion criteria for the studied group were: AMI treated with urgent coronary bypass surgery, complications of AMI involving the need for urgent surgical intervention, and other larger surgical procedures needed during hospitalization in the coronary unit.
In preintervention (CR) analysis, we compared patients after AMI with the comparison group of 30 healthy age-matched men, which had a median age of 57 (minimum 46 years, maximum 82 years), and without known existing risk factors for CAD (arterial hypertension, diabetes, hyperlipidemia, and chronic renal failure). Moreover, all of the healthy individuals were nonsmokers. We made an assessment of the cardiovascular disease development risk from measured data and laboratory parameters for each healthy participant. The inclusion criteria for the comparison group were the Framingham Coronary Heart Disease 10-Year Risk Score ≤13% and European 10-Year Risk Score for fatal CAD ≤8%.
Exclusion criteria for both healthy adults and patients after AMI were female gender, symptoms, signs and laboratory indications of acute infection, known diseases with ongoing chronic inflammation, and daily intake of dietary supplements/vitamins.
The study was approved by the Slovenian board for Medical Ethics No. 159/06/10, and all subjects gave their written informed consent.
Study design
CR protocol
The CR program was carried out in a local health resort. The rehabilitation comprised a 14-day-long, gradual training regimen in accordance with the position paper from the Cardiac Rehabilitation Section of the European Association of Cardiovascular Rehabilitation and Prevention. 14 The program consists of a supervised physical activity, which includes periodic ergometric training, aerobic exercises, and a stress relief program, including massages and baths. All patients took part in the educational program, which provided the information about the importance of pharmacological therapy, healthy diet, and changes in lifestyle.
Cardiac stress testing
We performed a cardiac stress test on a stationary exercise bicycle ergometer (cycloergometry) for each patient/healthy participant. Patients underwent cycloergometry before entering and at the end of the CR program.
During the cycloergometry, we raised the load by 25 Watts every 2 min. The testing was terminated when the patient reached the submaximal value for his heart rate (85% of the maximal heart rate), complained of dyspnea or pain (in the chest or other parts of the body) due to exhaustion, if we found ischemic changes in the electrocardiogram (ECG), bundle branch block, hypertensive reaction, or if arrhythmias appeared. There were no ischemic changes seen in the ECGs of healthy individuals. This fact, plus considering that the subjects were completely asymptomatic and without risk factors, implies that probability of significant CAD in these participants was rather low.
Clinical parameters
Clinical examination, measurements of blood pressure (Riva-Rocci), body weight, height, waist and hip circumference, calculation of body mass index (BMI), waist-to-hip ratio, and blood sampling were performed in each patient after AMI (before and at the end of the CR program) and each participant from the comparison group. All measurements were carried out in the morning in the fasting state at approximately the same time. Data from both groups were collected in the same time of the year.
Specimen characteristics
Blood samples were drawn from the antecubital vein of each patient/healthy participant in the morning, after 15 min of rest. In patients after AMI, blood was drawn before entering and at the end of CR program. Laboratory tests for complete blood count, glucose, lipids, and hsCRP were performed on the day of the blood collection.
Assay methods
The metabolic variables of fasting glucose, triacylglycerides (TAG), total cholesterol, high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C) were determined from serum by routine biochemical methods (all Cobas, Roche, Germany). Leukocytes were determined from whole blood by an automated analyzer (Sysmex, Clin Lab Products, USA).
hsCRP was determined using polystyrene particles coated with monoclonal antibodies specific to human CRP (Siemens, CardioPhase hsCRP). In this procedure, the sample is mixed with the coated particles, and these aggregates scatter a beam of light passed through the sample. The result is evaluated by comparison with a standard known concentration. 15,16
Statistical analysis methods
Considering that the distribution was not normal, we used nonparametrical tests for statistical analysis. Our data are presented as medians with ranges between the first and third quartile for continuous variables and as numbers and percentages for categorical variables. Differences in data in independent samples were compared using the Mann–Whitney U-test. Differences in medians of measured variables before and after the CR program in the whole group of patients were calculated using the Wilcoxon rank-sum test for continuous measures and the Fisher exact test for categorical variables. Nonparametric Spearman correlation coefficients were calculated to test associations between hsCRP and other parameters. To check the impact of smoking on these results, the whole group of patients was divided into smokers (n=16) and nonsmokers (n=14). Differences in measured variables before and after the CR program between the subgroups of smokers and nonsmokers were determined using the Wilcoxon rank-sum test for continuous measures and Fisher exact test for categorical variables. Differences between the group of smokers and nonsmokers were then compared using the Mann–Whitney U-test. The significant effects were indicated when the P value was less than 0.05. We used the SPSS statistics program (v.16.0) for statistic analysis and the graphic presentation of data.
Results
In preintervention analysis, due to optimal pharmacological treatment of arterial hypertension and hyperlipidemia, patients after AMI had significantly lower values of SBP, total cholesterol, and LDL-C compared to healthy men from comparison group (Table 1). However, patients had elevated measured markers of metabolic syndrome (higher BMI, waist circumference, waist-to-hip ratio, and lower HDL-C) and markers of inflammation, including higher hsCRP, leukocytes, neutrophils, and lymphocytes count in comparison to healthy individuals (Table 1; for hsCRP, see also Fig. 1).

Comparison of high-sensitivity C-reactive protein (hsCRP) in healthy adults and patients after acute myocardial infarction (AMI), and hsCRP before and after cardiac rehabilitation (CR). (*) P=0.002; (**) P=0.035.
All data are presented as medians with ranges between first and third quartile.
AMI, acute myocardial infarction; CR, cardiac rehabilitation; NS, nonsignificant; BMI, body mass index; SBP, systolic blood pressure; HR, heart rate; HDL-C, high-density lipoprotein; LDL-C, low-density lipoprotein; TAG, triacylglyceride; hsCRP, high-sensitivity C-reactive protein; MET, metabolic equivalent.
hsCRP at the beginning of the study in the complete group of patients significantly correlated with leukocytes count (r=0.414, P=0.01), BMI (r=0.40, P=0.03), and LDL-C (r=0.45, P=0.012) and hsCRP after CR significantly correlated with leukocytes count (r=0.575, P=0.001), smoking status (r=0.43, P=0.02), and LDL-C (r=0.42, P=0.02). Only in nonsmoking patients did hsCRP correlate with waist-to-hip ratio (r=0.75, P=0.002) before the CR program and with total cholesterol (r=0.64, P=0.01) and triglycerides (r=0.64, P=0.015) after the CR program.
As expected, when compared to healthy men, patients after AMI presented reduced exercise capacity (inferior maximal load and lower double product) and inferior values of maximal heart rate, SBP, and shorter total time of load. They also presented lower maximal blood pressure than healthy adults due to both good control of blood pressure with antihypertensives and inferior fitness. Because almost all patients were receiving β-blockers or ivabradine, chronotropic insufficiency was clearly seen and maximal heart rate was much more lower than in healthy individuals (Table 1).
Exercise capacity significantly improved during CR in patients after AMI. We noted higher achieved load, maximal heart rate, double product, and longer times of load. Their BMI, resting SBP, and resting pulse had also reduced during CR (Table 1). Amongst laboratory parameters, significant reductions were observed in total cholesterol, LDL-C, triacylglyceride (TAG), and in inflammatory markers (hsCRP, leukocytes, and neutrophils) after CR (Table 1 and Fig. 1).
When we divided the group of patients after AMI into smokers and nonsmokers, we found that patients who smoked tended to be younger (which was not statistically significant) and presented more expressed metabolic syndrome (lower HDL-C and higher TAG) and higher values of inflammatory markers (hsCRP almost significant, leukocytes, neutrophils, lymphocytes) (Table 2). There were no significant differences found in exercise capacity between smokers and nonsmokers at the time of study commencement, although we observed a trend toward longer times of load in nonsmokers.
All data are presented as medians with ranges between first and third quartile.
AMI, acute myocardial infarction; CR, cardiac rehabilitation; NS, nonsignificant; BMI, body mass index; SBP, systolic blood pressure; HR, heart rate; LDL-C, low-density lipoprotein; HDL-C, high-density lipoprotein; TAG, triacylglyceride; hsCRP, high-sensitivity C-reactive protein; MET, metabolic equivalent.
When comparing cycloergometric parameters separately in the smokers and nonsmokers group, both groups profited from the CR regarding achieved maximal load at the end of the CR. Besides that, nonsmokers also had significantly higher maximal heart rates, double product, time of load, and heart rate restoration in the first minute of rest at the end of the CR (Table 3). No such statistically significant differences were observed in the smokers group.
All data are presented as medians with ranges between first and third quartile.
CR, cardiac rehabilitation; MET, metabolic equivalents; SBP, systolic blood pressure; NS, nonsignificant; HR, heart rate.
In addition, we found a significant decrease in hsCRP (1.4 vs. 0.9; P=0.006; Fig. 2), leukocytes (6.8 vs. 6.1, P=0.023), neutrophils (3.7 vs. 3.4, P=0.016), BMI (27.8 vs. 27.2, P=0.017), resting SBP (130 vs. 120; P=0.041), resting pulse (66 vs. 61; P=0.007) total cholesterol (mean 3.4 vs. 3.1; P=0.006), LDL-C (1.8 vs. 1.7, P=0.014), and TAG (1.3 vs. 1.0, P=0,032) in the nonsmokers group. No such significant differences were demonstrated in the group of smokers. After completed CR, nonsmokers had higher HDL-C (1.1 vs. 0.85; P=0.004), lower TAG (1.0 vs. 1.7; P=0.002), lower leukocytes (6.1 vs. 8.5; P=0.0), lower neutrophils (4.3 vs. 4.8; P=0.0), lymphocytes (1.9 vs. 2.6; P=0.0), and lower resting pulse (61.0 vs. 65.5; P=0.031) than smokers. Importantly, nonsmokers also showed a trend of lower values of hsCRP than smokers (0.94 vs. 1.4; P=0.058) at the end of CR (Fig. 2).
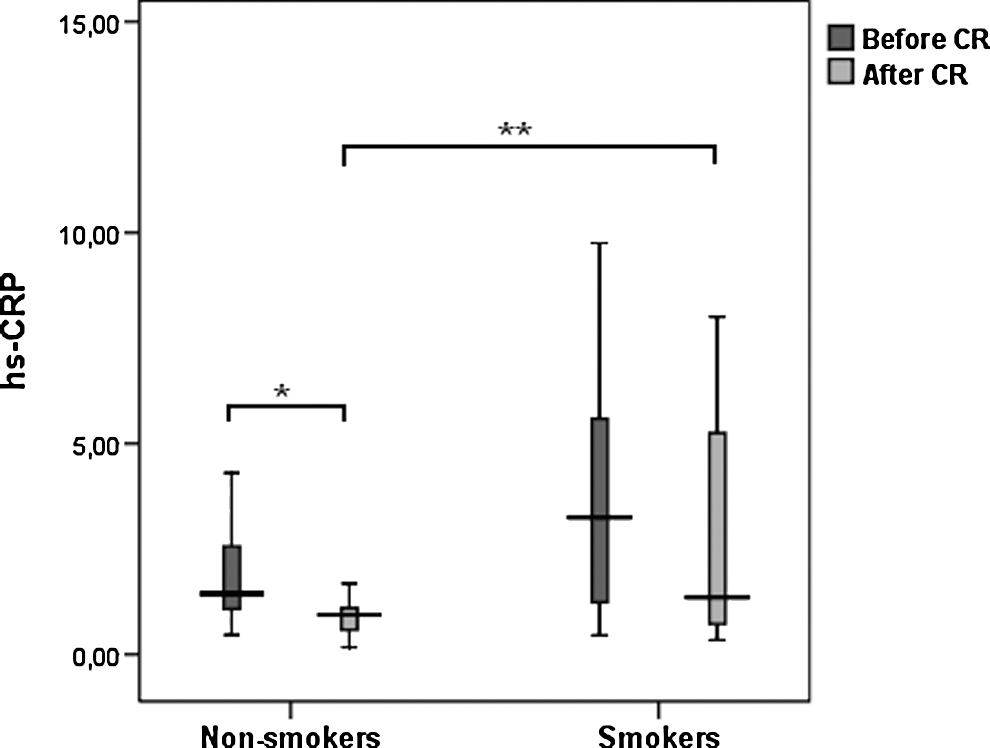
High-sensitivity C-reactive protein (hsCRP) dynamics between cardiac rehabilitation (CR) in nonsmokers and smokers. (*) P=0.006; (**) P=0.058.
Discussion
The results of our observational study show that our program of short CR after AMI (lasting only 14 days), which is supported by the Slovenian national insurance agency, is effective not only in improving exercise capacity and reduction of classical risk factors but also in decreasing the values of increased hsCRP, the most important marker of chronic low-grade inflammation. This effect has been associated with the reduction of markers of metabolic syndrome and was significant only in nonsmokers. These findings are to our best knowledge new and were not studied yet in previous studies.
According to preintervention analysis, the patients studied shortly after AMI had significantly lower blood pressure, total cholesterol, and LDL-C compared to age-matched healthy individuals. Blood pressure, total cholesterol, and LDL-C values of our patients reached on average the recommended target values for secondary prevention of CAD. 13
However, patients (vs. healthy men from comparison group) were shown to have higher markers of inflammation measured by hsCRP and leukocyte count, which was associated both with metabolic syndrome (expressed by lower HDL-C, higher BMI, hip circumference, and waist-to-hip ratio) and with a higher percentage of smokers (53.3%). This was in accordance with previous studies, which demonstrated that patients with clinically expressed atherosclerosis have higher values of inflammation markers than healthy adults. 4,5 Furthermore, an important note is that increased hsCRP was detected in our patients despite optimal treatment with drugs for secondary prevention of CAD. These drugs include statins and acetylsalicylic acid, both of which have already been proven to be effective in diminishing the incidence of CAD events through the reduction of low-grade inflammation in AMI survivors. 17 –19 This points to the fact that treatment exclusively with drugs is not effective enough to reduce low-grade inflammation in patients after AMI to the level of age-matched healthy adults.
We assumed that increased low-grade inflammation was associated with metabolic syndrome and smoking status, because the studied patients had, compared to age-matched healthy men, significantly higher BMI, waist-to-hip ratio, and lower HDL-C, and considering that 53.3% (16 out of 30) patients were smokers. A positive correlation between hsCRP and smoking in the complete group of patients and correlation between hsCRP and some markers of metabolic syndrome in nonsmoking patients further confirm previously known facts established by many studies. 1,20,21
In further analysis, we demonstrated that the short-term CR program proved to be effective not only in improving exercise capacity but also in the further reduction of classical risk factors, markers of metabolic syndrome, and levels of hsCRP in the entire group of patients. This result is new because no studies have proven to diminish classical risk factors, markers of metabolic syndrome, and hsCRP in such a short-term CR program in survivors of AMI.
Although many recent investigations suggest that physical activity reduces hsCRP levels up to one-third (independent of baseline levels of hsCRP, body composition, or weight loss), all of these conclusions have only been associated with long-term physical activity. 12,22 Short and exhausting exercise was, on the contrary, shown to bring about an acute-phase response with elevation of CRP and white blood cells, which remained elevated up to 6 days after acute exercise. 23 Furthermore, some studies have indicated that specific forms of physical activity are associated with a lower likelihood of elevation of inflammatory markers, which means that the type of exercise in CR exerts an important influence on inflammatory risk factors. 24 Therefore, due to our obtained results, we presumed that our 2-week CR program, not studied in previous studies, which in accordance with the position paper from the Cardiac Rehabilitation Section of the European Association of Cardiovascular Rehabilitation and Prevention 14 contains both gradual physical training and advice about healthy lifestyle, already activates adaptive processes. It not only improves exercise capacity but also diminishes low-grade inflammation in addition to reducing classical risk factors and metabolic syndrome parameters.
Although the compliance was equal between smokers and nonsmokers, this positive effect was shown to be significant only in nonsmoking patients. This difference was independent of lipid treatment because nonsmoking and smoking patients did not differ in lipid treatment or in lipid profile before and after CR program. According to a strong, positive dose-dependent relationship between cigarette smoking and hsCRP demonstrated in several studies, it was apparent in 2006 that new studies were required to determine the impact of physical activity on hsCRP in physically active current smokers. 12 Yet, as we searched through the literature, we found only one study by Hammet and co-workers that focused on inflammatory markers and smoking during exercise training. 25 Importantly, this study was performed in healthy women and not in patients after AMI. Overall, we found no similar study in patients after AMI that compared CRP in smokers and nonsmokers.
Our new results imply a possible explanation, that smoking is indeed a risk factor, which is strongly associated with chronic low-grade inflammation. The observed decrease of hsCRP (in nonsmokers) might be related to spontaneous disease processes, which cannot be verified due to lack of a control group. In spite of that, it is possible that smokers, who are continuously in a higher inflammatory state than nonsmokers after AMI, are unable to activate adaptive processes (or they activate them more slowly) that diminish low-grade inflammation during the short-term CR program. There are several possible explanations. It has been proven that smoking lowers lung capacity, that smokers achieve lower maximal heart rates, and that the exchange of gases in the lungs is obstructed. Therefore, smokers achieve lower maximal oxygen consumption and have impaired endothelial vascular tone control and impaired oxygen transport. 26 Furthermore, smokers are known to be in an elevated state of oxidative stress and chronic inflammation. Bloomer and co-workers have shown that smokers responded to strenuous exercise with elevated oxidative stress markers, while nonsmokers of comparable age did not. 27 It is also known that smokers have lower concentrations of antioxidants (such as ascorbate) and increased numbers of activated phagocytes that can generate large amounts of reactive oxygen species, which damage endothelial cells. Smokers also have activated pro-oxidant cytokine networks, including increased concentrations of tumor necrosis factor-α (TNF-α), interleukin-8 (IL-8), and interleukin-1 (IL-1). 28 To conclude, this state of chronic inflammation and oxidative stress might be the cause of inability to lower hsCRP throughout the rehabilitation program and profit from physical activity and other nonpharmacologic measures. This finding, which is to our knowledge new, seems to be very noteworthy because it may already lead to practical clinical consequences. All patients after AMI should be advised to stop smoking before entering CR to achieve its beneficial effects in the sense of improving low-grade inflammation.
In conclusion, the results of our study demonstrate that patients after AMI have elevated levels of hsCRP despite optimal pharmacological treatment. hsCRP was associated with both metabolic syndrome and smoking. Chronic low-grade inflammation, i.e., hsCRP, can be reduced by a 2-week cardiac rehabilitation program; however, this effect is significant only in nonsmokers. The clinical relevance of our study should be to advise all patients after AMI to quit smoking before entering the CR program if they want to achieve optimal beneficial effects from it.
Limitations
This study was an observational study on a small number of patients, using a pre–post/test design and a true control group, with no physical activity and other components of CR; but only with medical management, was lacking due to ethical reasons. Therefore the results of the study might be partly subject to spontaneous disease processes, including reduction of hsCRP levels in nonsmokers. It is also possible that the observed reduction of hsCRP might be a consequence of not only CR but also of multiple other mechanisms associated with the postmyocardial infarction period and CR.
Footnotes
Acknowledgments
The study was completely supported by Slovenian project called Target Research Programmes until 2013 (grant no. CRP V4-0513). Our special thanks go to head nurse Marinka Sečnik, nutritionist Janja Strašek, and all of the medical and nurse staff from Terme Krka Šmarješke Toplice Health resort, Slovenia, who helped with the clinical part of the study and to Prof. Marija Prezelj, chief of laboratory, and laboratory technicians Marjana Prah and Vera Troha at the Clinical Institute of Clinical Chemistry and Biochemistry, University Medical Center Ljubljana, Slovenia, for the excellent performance of laboratory investigations.
Author Disclosure Statement
No competing financial interests exist.