
Abstract
Background:
Patients with morbid obesity have a high risk of developing type 2 diabetes mellitus (T2DM). Important risk factors include body mass index (BMI), waist circumference, and insulin resistance. In this prospective study, we investigated if preoperative lifestyle changes followed by bariatric surgery could reduce these risk factors.
Methods:
Forty nondiabetic obese patients aged 27–57 years participated. Baseline BMI was 36.1–65.6 kg/m2. Fasting glucose, C-peptide, and glycated hemoglobin (HbA1c) were measured at baseline and 1 year after surgery. The patients underwent lifestyle changes for a period of 3 months prior to bariatric surgery and were followed for 1 year after surgery. The correlations between risk factors and weight reduction were assessed by a Pearson test.
Results:
Lifestyle changes resulted in a mean weight reduction of 14.3 kg. One year after bariatric surgery, the patients had a mean reduction in BMI of 17.6. Mean waist circumference was reduced from 136.5 cm to 100.7 cm. At baseline, all 40 patients had a waist circumference >100 cm; 1 year after surgery 18 of 40 patients did. At baseline, 11 out of 40 had insulin resistance (as defined by a homeostasis model score >3.99), whereas 1 year after surgery none of the patients did. There was a statistically significant correlation between change in waist circumference and change in insulin resistance (P<0.02), and between HbA1c and weight loss (P<0.002).
Conclusions:
Our study shows that, in morbidly obese individuals, lifestyle changes followed by bariatric surgery led to a significant weight loss and a reduction in risk factors for development of T2DM.
Introduction
Materials and Methods
Study participants and experimental design
This was a prospective study with 40 morbidly obese nondiabetic patients admitted to the Regional center for treatment of morbid obesity at Nordland Hospital, Norway. The patients were followed from admission to 1 year after bariatric surgery. The study was approved by the regional ethics committee of Northern Norway in accordance with the Helsinki II declaration and by the Norwegian Data Protection Authority. Written informed consent was obtained from all participation patients.
Inclusion criteria were body mass index (kg/m2, BMI) ≥40 or BMI ≥35 with co-morbidity, such as hypertension and sleep apnea, but with no overt diabetes and with a normal oral glucose tolerance test (OGTT). The patients underwent lifestyle changes for a mean period of 3 months prior to bariatric surgery and were followed 1 year after surgery. Waist circumference was measured midway between the lateral lower ribs and the iliac crest with the patient in an upright position at first admission and at 1 year after surgery.
Blood sampling
Fasting blood samples were obtained by standard venipuncture on three occasions—at admission, at the time of surgery, and 1 year after surgery. Routine blood analyses were performed at the laboratory of Nordland Hospital. The analyses included an OGTT at first visit and glycated hemoglobin (HbA1c) at all three occasions. In addition, fasting glucose and C-peptide were measured at first admission and after 1 year. C-peptide was analyzed at Aker University Hospital, Oslo. Samples for C-peptide were frozen in aliquots at −80°C and analyzed in batches at the end of the study. For HbA1c, the Tosoh Bioscience HLC-723 G8 (Tokyo, Japan) method was used.
HOMA-IR score was calculated using the HOMA-IR calculator, developed by the “Diabetes Trials Unit” (University of Oxford, UK). 11 The HOMA-IR score is a method to assess insulin resistance from fasting glucose and insulin or C-peptide concentration.
Lifestyle changes
Patients had to undergo lifestyle changes preoperatively, resulting in an average weight loss of 10%. The aim of this was to prepare the patients for a life with a small gastric pouch after gastric bypass. Patients received repeated personal guidance concerning change of eating habits and increased physical activity at baseline and by phone consultations with a nutritionist or specially educated nurse every 2 weeks preoperatively. The patients were told to have a meal every 3–4 hours, for a daily total of three main meals and three to four small meals in between. They were advised to eat an energy-restricted diet of 2000 kcal for males and 1500 kcal for women. That included fat content of <30 energy %, complex carbohydrates content of <40–50 energy %, and protein content of <20 energy %. It was also mandatory to participate in a 2-day course focusing on lifestyle changes and on how bariatric surgery would affect daily life. Information and education were given according to the Norwegian guidelines for treatment of morbidly obese patients, and Norwegian guidelines for nutrition given by the Norwegian Ministry of Health and Care Services. The patients were not accepted for surgery before they had achieved a 10% weight loss. It took patients on average 12 weeks to achieve a 10% weight loss.
Surgery
Two surgical methods were used: (1) LRYGB was performed using a standardized procedure by creating a small ventricular pouch of 30 mL, a bileopancreatic limb of 50 cm, and an alimentary limb of 100 cm. 12 This method was used for patients with BMI ≤50. (2) Bileopancreatic diversion with duodenal switch (BPDDS) was performed using a standardized procedure. We created a gastric sleeve using a 32 French probe to measure the diameter of the gastric sleeve, then made an alimentary limb of 150 cm and a common channel of 100 cm. 12 This method was chosen for patients with a BMI >50. One patient received a LRYGB despite a BMI of 51.7. One patient received a BPDDS despite a BMI of 46.7. This patient had lost 14.7 kg prior to the first admission, so the initial BMI of the patient was 51.7. All operations were performed by two experienced bariatric surgeons.
Statistics
Numerical data are presented with mean. Repeated-measures analysis of variance (ANOVA) was used for comparing changes in weight, BMI, and HbA1c during the observation period. A one-sample paired t-test was used for comparing changes in weight, BMI, and HbA1c from baseline to the time of surgery and from the time of surgery to 1 year after surgery. A one-sample paired t-test was also used for comparing HOMA-IR score and waist circumference. Correlation between variables was calculated with a Pearson correlation test. Graphs and analyses were done in PRISM 6 (GraphPad Software Inc., La Jolla, CA).
Results
Baseline characteristics
Baseline characteristics are given in Table 1.
LRYGBP, laparoscopic Roux-en-Y gastric bypass; BPDDS, bileopancreatic diversion with duodenal switch; BMI, body mass index; HOMA-IR score, homeostasis model assessment of insulin resistance.
Effect on weight loss, BMI, and waist circumference
The 3-month lifestyle change resulted in a mean preoperative weight loss of 14.3 kg, (range 12.1–19.5 kg, P<0.0001). One year after surgical intervention, patients had a mean weight loss from baseline of 50.52 kg (range 30.1–85.8 kg, P<0.0001) (Fig. 1A). Correspondingly, BMI was reduced from a mean baseline value of 46.94 kg/m2 (range 36.1–65.6 kg/m2) to a mean value of 41.75 kg/m2 before surgery (range 33.5–58.7 kg/m2, P<0.0001). One year after surgery, mean BMI was 29.31kg/m2 (range 22.4–38.2 kg/m2, P<0.0001) (Fig. 1B). All patients had a statistically significant reduction in waist circumference from baseline to 1 year after surgery. The mean reduction was 35.8 cm (range 33.0–46.0 cm, P<0.0001) (Fig. 1C).
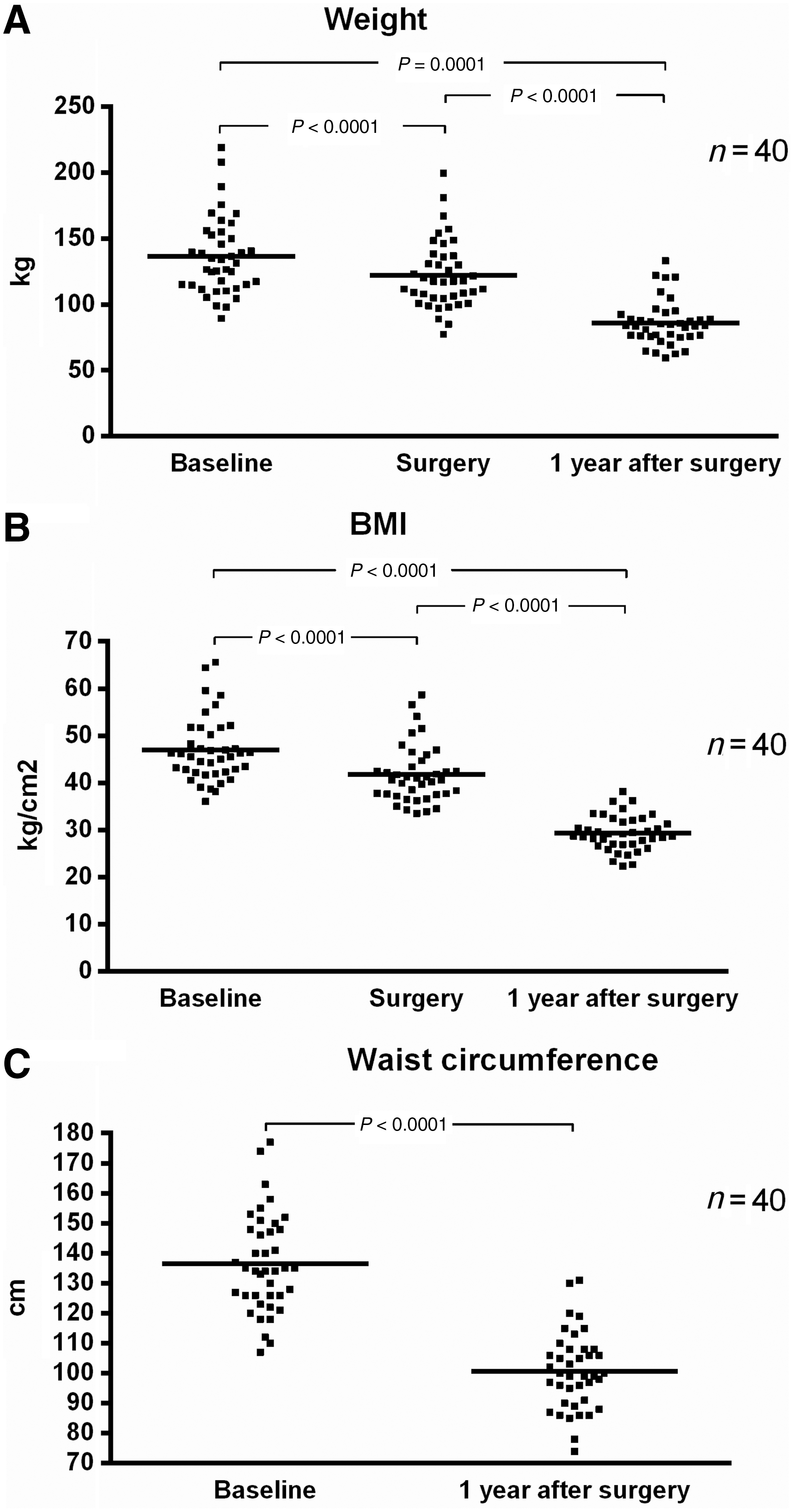
Weight
Effects on glucose metabolism
Mean fasting glucose decreased from 5.46 mmol/L at baseline to 4.76 mmol/L 1 year after surgery (P<0.0001) (Fig. 2A). Ten out of 40 patients had a fasting glucose between 6 and 7, possibly indicating impaired glucose tolerance (IGT) or T2DM, but none of the patients had 2-h fasting glucose (2hFG) ≥11.1 mmol/L. Three patients had 2hFG ≥7, whereas one of them had 2hFG of 10.7 mmol/L (data not shown). The patients had a statistically significant reduction in HbA1c %. Mean value decreased from 5.81% at baseline to 5.70 % at time of surgery (P<0.02), and further to 5.46% 1 year after surgery (P<0.0001) (Fig. 2B).
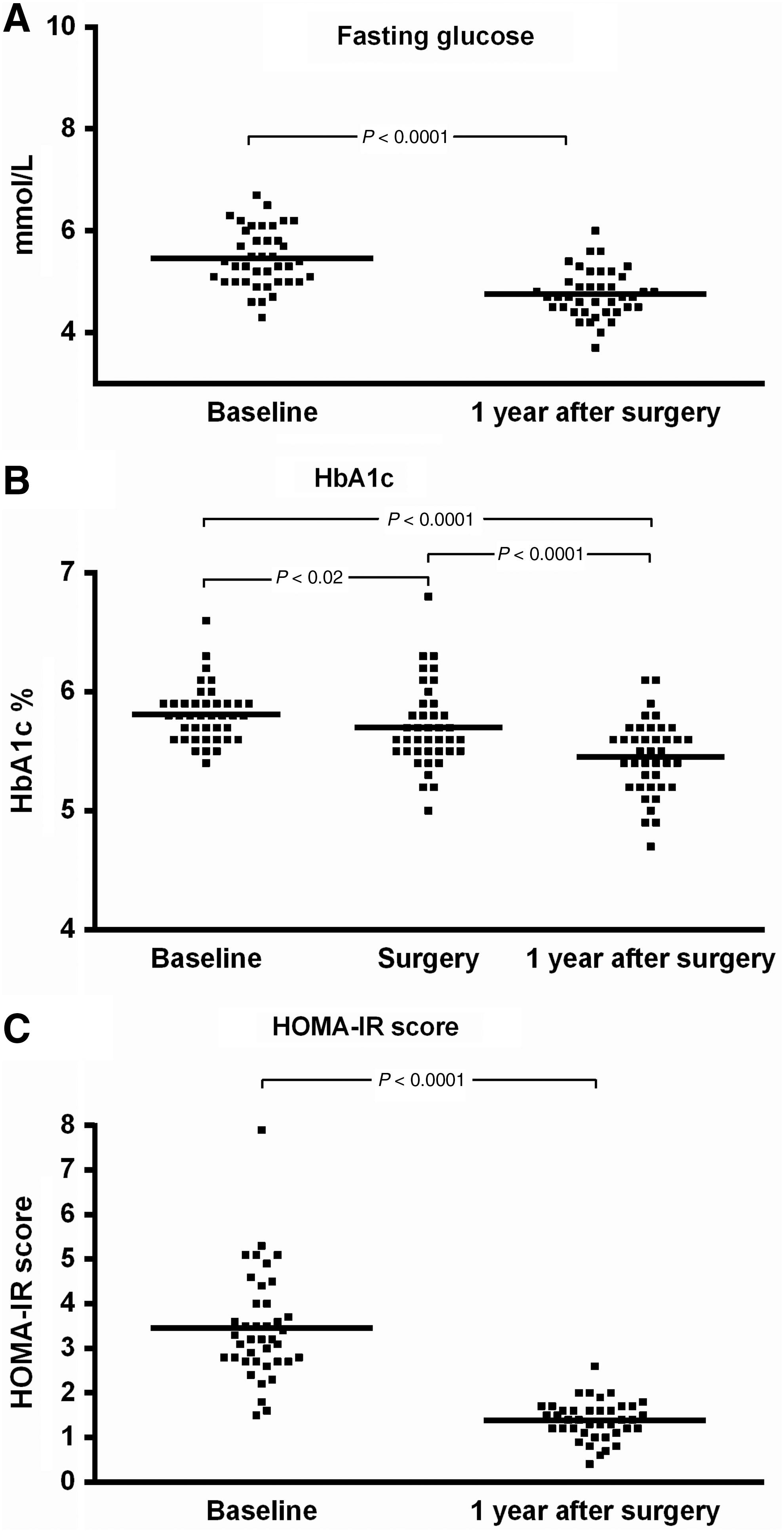
Fasting glucose
Correspondingly, mean C-peptide value decreased from 1.56 nmol/L at baseline to 0.64 nmol/L 1 year after surgery. Mean reduction was 0.92 nmol/L (range 0.49–3.27 nmol/L, P<0.0001; data not shown). Mean HOMA-IR score reduction from baseline to 1 year after surgery was 2.1 (range 1.1–5.3, P<0.0001) (Fig. 2C).
Correlations
There was a statistically significant correlation between reduction in HOMA-IR score and weight loss from baseline to 1 year after surgery (R 2=0.121, P<0.03) (Fig. 3A). Furthermore, correlation between HOMA-IR score reduction and waist circumference reduction was also statistically significant (R 2=0.148, P<0.02) (Fig. 3B). There was a strong correlation between weight loss and waist circumference reduction (R 2=0.712, P<0.0001; data not shown).
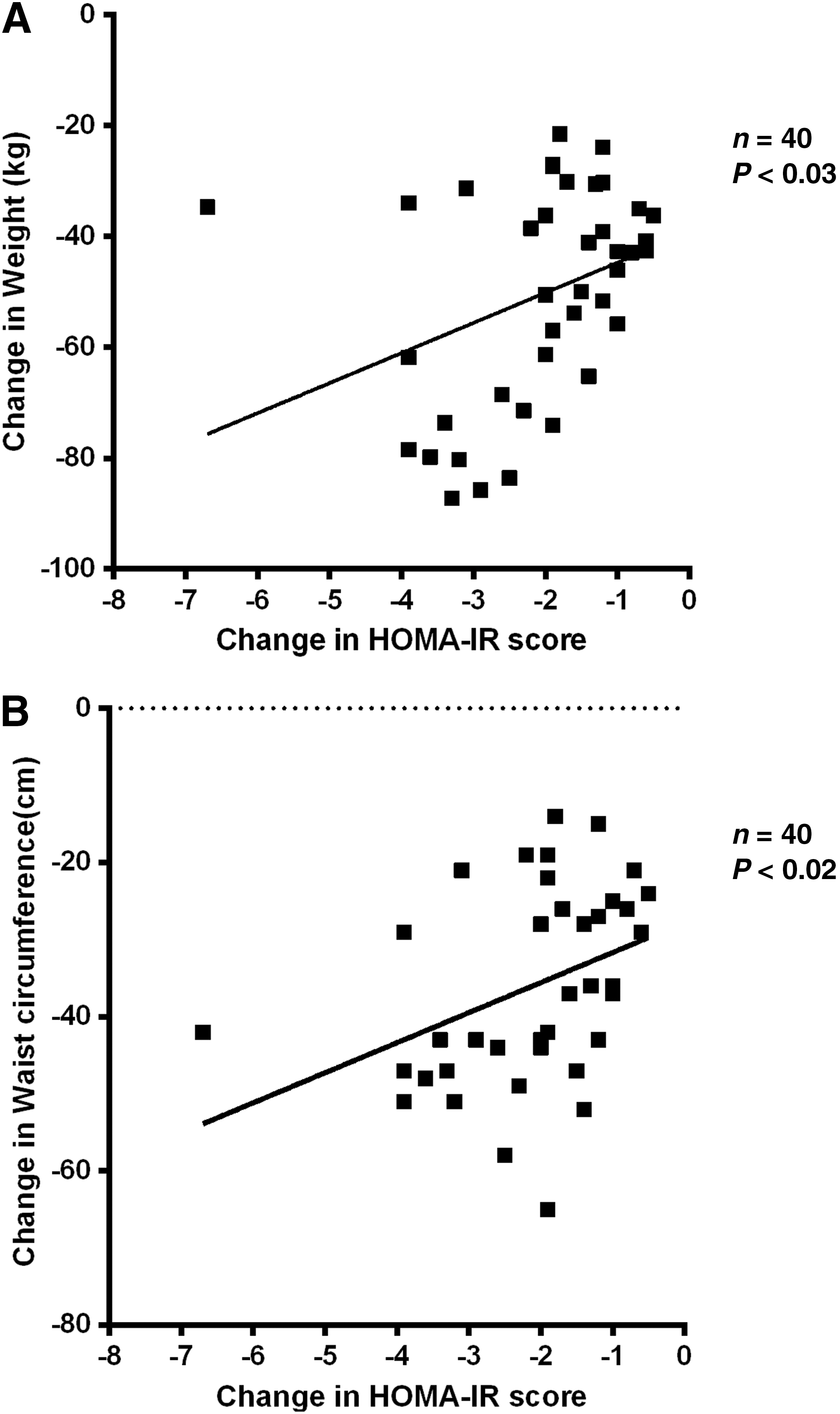
Correlation between change in homeostasis model assessment of insulin resistance (HOMA-IR) score and weight
The correlation between preoperative weight loss and preoperative HbA1c reduction was not statistically significant (R 2=0.041, P<0.3) (Fig. 4A). From baseline and from time of surgery to 1 year after surgery, however, the same correlations were statistically significant [R 2=0.10, P<0.05 (Fig. 4B) and R 2=0.247, P<0.002, respectively (Fig.4C)].
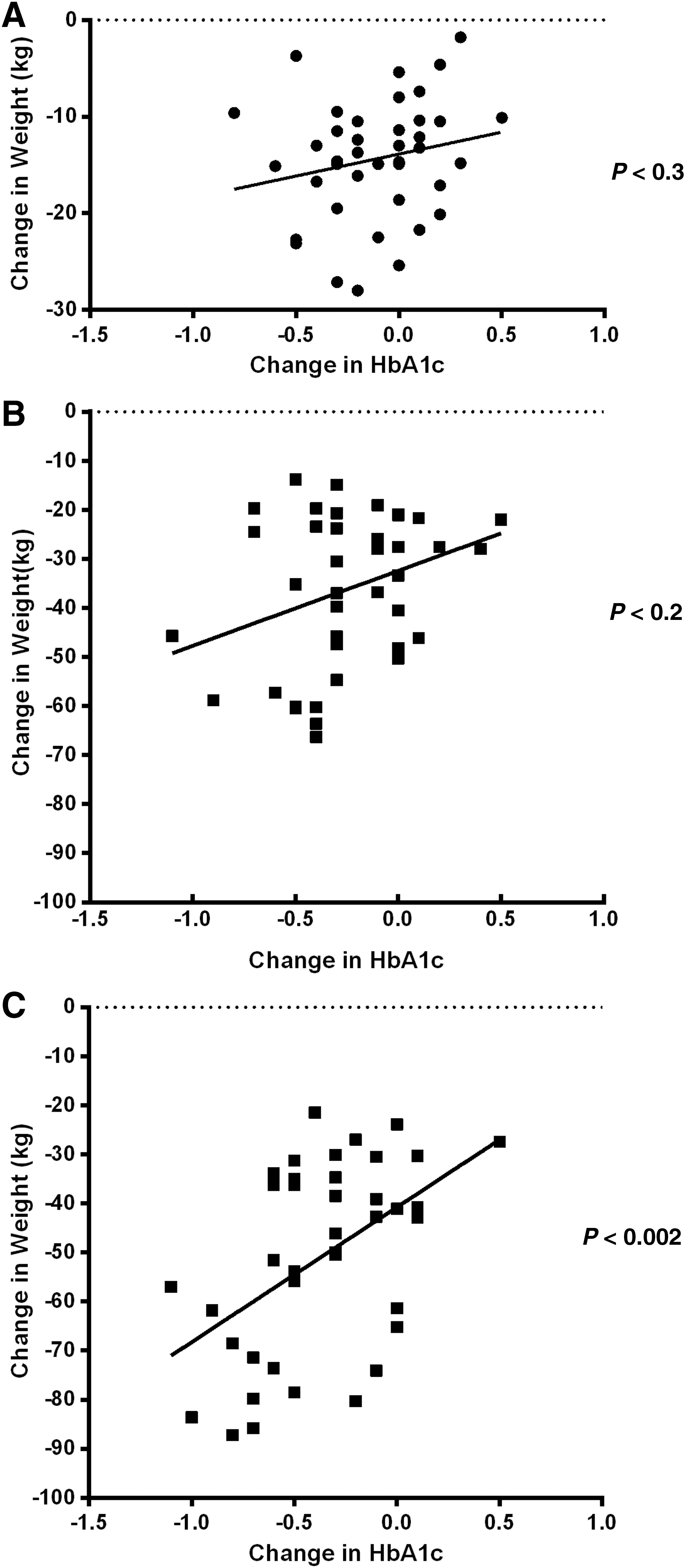
Correlation between change in glycated hemoglobin (HbA1c) and weight at three different occasions—baseline versus surgery
Discussion
In this study, we have demonstrated how lifestyle changes followed by bariatric surgery reduce risk factors for development of T2DM in nondiabetic patients. The main factor for development of T2DM is increasing body weight and the development of obesity. The relative risk of T2DM increases exponentially with increasing BMI. 1 The true incidence of T2DM in morbidly obese patients has been estimated to 31%, but only a fourth of these were detected by fasting plasma glucose screening. 10,13 In addition, many morbidly obese patients have IGT. IGT is defined as glucose plasma levels of 7.8–11.0 mmol/L 2 h after an OGTT. Fasting glucose levels may be normal or slightly elevated in IGT. The term “prediabetes” is used to define patients with IGT and/or insulin resistance. 3 Up to 70% of morbidly obese patients who have “prediabetes” develop T2DM during their lifetime. 3 Using fasting C-peptide and fasting glucose to calculate the HOMA-IR score can identify patients in danger of developing T2DM, even if their OGTT is normal. 11 There are clinical trials that show a decrease in development of T2DM after lifestyle intervention or treatment with metformin. 14,15 In our study, nondiabetic patients did not (by definition) have IGT, but 11 out of 40 patients had a HOMA-IR score higher than 3.99, which indicates insulin resistance. Prioritizing these patients for lifestyle intervention and bariatric surgery could prevent development of T2DM.
HbA1c has been used to monitor patients suffering from diabetes mellitus. However, the World Health Organization now accepts using HbA1c as a diagnostic criterion for diabetes mellitus. 16,17 HbA1c reflects the blood glucose level over the last 8–12 weeks. Even if the weight loss was 10%, our patients had a limited effect on reduction of HbA1c preoperatively. This can be explained by the short period from admission to surgery, on average only 12 weeks. In previous trials, patients going through conventional treatment for morbid obesity had an average weight loss of 4.3%–10% after 1–2 years. 2,18,19 Conventional treatment included change of lifestyle and eating habits as well as increased physical activity. However, these patients were randomized to conventional therapy or bariatric surgery, and individuals already diagnosed with T2DM were not excluded. Jorgensen et al. did not find a statistically significant reduction in HbA1c 1 year after intervention in a group of nondiabetic obese patients undergoing LRYGBP. 20 These results differ from ours. In our study, however, patient`s weight and HbA1c at baseline were higher, weight range was wider, and patients lost more weight during the study period compared to patients in the study by Jorgensen et al. Also, in our study, several patients received the more extensive BPDDS procedure because of baseline BMI higher than 50. The BPDDS procedure leads to a greater weight loss. In our study, 11 out of 40 patients had a baseline BMI higher than 50. However, even if we exclude patients with a baseline BMI higher than 50 from in our study, we still observed a higher weight loss 1 year after surgery than did the Jorgenson study. In our study, a higher weight loss was correlated with a higher reduction in HbA1c.
Waist circumference is also a good predictor (of risk) for development of T2DM. 21 –24 The risk for developing insulin resistance increases at a waist circumference higher than 102 cm in men and higher than 88 cm in women in subjects with a BMI ≥30. 24 –26 Waist circumference reflects the amount of intra-abdominal fatty tissue and thereby the hormonal effect on insulin secretion and action. Intra-abdominal fatty tissue contains larger adipocytes than subcutaneous fatty tissue. The larger the adipocytes, the more dysfunctional they become concerning the antilipolytic effect of insulin. 27 Increased insulin resistance in intra-abdominal fatty tissue leads to reduction of glucose uptake compared to subcutaneous fatty tissue. 27 Through measurement of plasma glucose, HbA1c, and plasma lipopolysaccharide (LPS) before and after bariatric surgery, several studies have indicated a relationship between obesity, gut microbiota, and development of T2DM. 28 –30 Recently, we have shown a statistically significant correlation between plasma levels of LPS and intra-abdominal fatty tissue volume as well as a significantly increased gradient of bacterial DNA content in adipose tissue compartments with increasing proximity to the gut. Furthermore, bariatric surgery significantly reduced plasma levels of LPS, and the reduction correlated with a reduction in HbA1c. 31 Because intra-abdominal fatty tissue is the leading factor for an increased waist circumference, these findings underline the importance of waist circumference as a risk factor for development of T2DM.
Our study has some limitations. One is the lack of a control group, but it is difficult to compare patients undergoing bariatric surgery and patients undergoing conventional treatment due to the big difference in achieved weight loss. Furthermore, the study has a limited sample size, which can lead to statistical Type II errors, whereas Type I errors are less likely. The imbalance between female and male participants could be of significance, but knowing that male fat distribution leads to a bigger waist circumference our male-to-female ratio should indicate that our results are not overestimated. Furthermore, waist circumference and HOMA-IR score were measured only two times during the study period. On the other hand, the prospective study design and the fact that the study group was followed for 1 year after surgery strengthen our results.
Conclusion
Our study shows that, in morbidly obese nondiabetic individuals, lifestyle changes followed by bariatric surgery lead to a significant weight loss, a reduction in waist circumference, and reduction in HOMA-IR score. We postulate that lifestyle changes followed by bariatric surgery reduce the probability of developing T2DM. To measure waist circumference is an easy and cheap measurement to perform and should therefore be a part of examination of all obese patients. It is important to identify patients at risk and initiate treatment modalities that reduce their body weight and thereby reduce the risk of developing T2DM.
Footnotes
Acknowledgments
The skillful assistance by the nurses at the Regional Centre for Treatment of Morbid Obesity and Hilde Fure at the Somatic Research Laboratory at Nordland Hospital is greatly acknowledged. This study was supported by Nordland Hospital and research grants from the regional health authorities of Northern Norway.
All authors contributed to the study design. T.K.N. interpreted results of analyses, prepared figures and table, and drafted the manuscript. E.W.N. and K.T.L. edited and revised the manuscript. T.K.N., E.W.N., and K.T.L. approved the final version of manuscript.
Author Disclosure Statement
T.K.N., E.W.N., and K.T.L. state that we have no competing financial interests.