
Abstract
Background:
The concept that androgens regulate multiple aspects of adipose tissue metabolism in women is based on studies of women with pathological androgen excess and in vitro studies generally using supraphysiological androgen concentrations. We investigated whether in women with normal-range serum testosterone, relationships exist between serum androgens and expression of proinflammatory (tumor necrosis factor-α, interleukin-6, CD68), anti-inflammatory (adiponectin), and lipid metabolic (lipoprotein lipase, hormone sensitive lipase) genes in omental adipose tissue, and severity of nonalcoholic fatty liver disease (NAFLD).
Methods:
We studied obese women undergoing laparoscopic gastric band surgery (premenopausal, regular menses, nondiabetic, serum testosterone <2.5 nmol/L, n=27). Gene expression was measured in omental adipose tissue. Liver biopsies were examined in 22 participants.
Results:
Serum testosterone or androstanediol glucuronide (an indicator of peripheral androgen metabolism) were not related to markers of inflammation or lipid metabolism in omental adipose tissue. In women with NAFLD, there was a significant trend to higher serum free testosterone, serum insulin, and insulin resistance with increasing severity of liver pathology; however, markers of inflammation in omental adipose tissue did not differ. Omental lipoprotein lipase expression was significantly increased in women with nonalcoholic steatohepatitis (NASH).
Conclusions:
These primarily correlative data suggest that physiological-range androgen levels do not influence inflammation or lipid metabolism in omental adipose tissue of women, but further studies of direct androgen effects on adipose tissue are needed for confirmation. Androgens may still play a role in the pathogenesis of NAFLD in women, via mechanisms unrelated to omental adipose tissue metabolism.
Introduction
A
Another potentially important effect of androgens in adipose tissue is on pro- and anti-inflammatory adipokines. Chronic inflammation in adipose tissue is recognized to play a key role in the pathogenesis of insulin resistance in obesity. 9 Although not yet studied in the adipose tissue of women, there is evidence in various cell systems that testosterone regulates the production of adiponectin 10 and interleukin-6 (IL-6), 11 which are relevant for their anti-inflammatory and proinflammatory effects, respectively.
Androgens also influence hepatic function. In female mice, more than a thousand genes expressed in liver are androgen-regulated. 12 This finding may be relevant to the pathophysiology of nonalcoholic fatty liver disease (NAFLD), a spectrum ranging from fatty infiltration (steatosis) to nonalcoholic steatohepatitis (NASH) to fibrosis and cirrhosis.
The evidence to date that androgens play a role in regulation of hepatic and adipose tissue metabolism in women largely consists of data from in vitro experiments or from the study of women with polycystic ovary syndrome (PCOS), a common condition in women of reproductive-age characterized by androgen excess and metabolic dysfunction. 13 A limitation of many in vitro studies of female adipose tissue metabolism is that supraphysiological androgen concentrations have been used, commonly testosterone or dihydrotestosterone (DHT) at a concentration of 1 μmol/L, making the physiological relevance of the findings uncertain. 1 –4 In women with PCOS, there are multiple differences in gene and protein expression profiles in visceral adipose tissue compared with non-hyperandrogenic women, 14,15 and adipose tissue protein expression patterns are similar to those in men, 16 consistent with a role of androgens in adipose tissue metabolism in this syndrome. NAFLD is common in women with PCOS, and evidence is accumulating that androgen levels influence the risk of NAFLD in PCOS. 17 –19 However, given that PCOS is a complex disorder with both genetic and in vivo environmental factors contributing to metabolic dysfunction, 13 whether these effects of androgens on adipose tissue and liver can be extrapolated to women without PCOS is unknown. 20
Understanding the role of sex hormones in metabolism may provide insight into the pathogenesis of common conditions such as glucose intolerance and NAFLD; however, studies investigating the metabolic effects of physiological-range androgens in women are few. In healthy nonobese women, serum testosterone was positively correlated with total fat mass, but unlike in women with androgen excess, serum testosterone was not associated with abdominal adiposity or with measures of energy and substrate metabolism. 21 Additionally, in postmenopausal women, higher androgen levels within the normal range have been reported to have beneficial metabolic effects. 22
The aim of this study was to investigate whether serum testosterone levels varying within the physiological range in premenopausal women are associated with changes in adipose tissue and hepatic metabolism. Specifically, we investigated if relationships exist between serum androgen levels and (1) inflammation in omental adipose tissue, (2) expression of genes involved in lipid metabolism in omental adipose tissue, and (3) severity of NAFLD. We hypothesized that women with higher serum androgen levels within the normal range may have increased expression of proinflammatory and lipolytic genes in omental adipose tissue and increased risk of hepatic steatosis/steatohepatitis, consistent with adverse effects of androgens on adipose tissue and liver.
Materials and Methods
Patients
Obese premenopausal women undergoing elective laparoscopic gastric band surgery were recruited (n=27). Exclusion criteria were irregular menstrual cycles (<27 or >35 days) or a previous diagnosis of PCOS, serum testosterone ≥2.5 nmol/L, fasting blood glucose ≥7.0 mmol/L, or a previous diagnosis of type 2 diabetes, and use of confounding medications within the previous 3 months, especially the combined oral contraceptive pill. Patients on hepatotoxic medications were also excluded. All of the patients had a history of nil or minimal alcohol intake. The study was approved by the institutional Human Research Ethics Committee and patients gave written consent. Three women previously diagnosed with PCOS (clinical and/or biochemical hyperandrogenism plus oligo/amenorrhea), who were not taking the combined oral contraceptive pill, were recruited to act as a reference group for serum androgen levels.
Tissue collection
Participants had blood collected after an overnight fast before surgery. Omental adipose tissue (2–10 grams) was collected during surgery. A proportion was frozen immediately in liquid nitrogen and later stored at −80°C for RNA extraction; the remainder was collected in Dulbecco modified Eagle medium (DMEM; Gibco, Grand Island, NY)+1% bovine serum albumin (BSA) for transport to the laboratory. A liver biopsy was routinely performed as part of the operative procedure using a 14-gauge, 20-mm Temno needle (Health Care Corp, McGraw Park, IL).
Blood assays
Plasma glucose (Beckman Coulter DxC Clinical System, Brea, CA) and insulin (Beckman DxI Immunoassay System, Brea, CA) were measured. Homeostasis model assessment of insulin resistance (HOMA-IR) was calculated using a HOMA Calculator 2.2 (Diabetes Trials Unit, University of Oxford,
Adipose tissue explants
Samples of ∼0.5 gram of omental adipose tissue were minced and suspended in low-glucose DMEM+1% BSA, washed, and incubated for 30 min at 37°C and 5% CO2. Duplicate samples were transferred to multiwell plates for incubation (24 or 48 hr) under the same conditions. Media samples were collected and stored at −80°C. IL-6 secretion by the explants was measured using an enzyme-linked immunosorbent assay (ELISA; R&D Systems, Minneapolis, MN).
Quantitative real-time PCR
Total RNA was extracted from adipose tissue using TRIzol reagent (Life Technologies, Carlsbad, CA), with further purification using an RNeasy Mini Kit (Qiagen, Germantown, MD). Reverse-transcription was performed using avian myeloblastosis virus reverse transcriptase (AMV RT) and random primers (Promega, Madison, WI) according to the manufacturer's instructions. Real-time PCR (ABI 7900HT, Applied Biosystems, Carlsbad, CA) was used to measure gene expression of tumor necrosis factor-α (TNF-α), IL-6, CD68, adiponectin, hormone-sensitive lipase (HSL), and lipoprotein lipase (LPL). The primers used were: TNF-α-F 5′-CTTGTTCCTCAGCCTCTTCTCC-3′, TNF-α-R 5′-CAGGCTTGTCACTCGGGGTTCG-3′; IL-6-F 5′-CCTTCGGTCCAGTTGCCTTCT-3′, IL6-R 5′-TGTTTTCTGCCAGTGCCTCTTTG-3′; CD68-F 5′-AGTGGACATTCTCGGCTCAG-3′-, CD68-R 5′-TGATGAGAGGCAGCAAGATG-3′; adiponectin-F 5′-GGTGAGAAGGGTGAGAAAGGAGAT-3′, adiponectin-R 5′-GAATGGGCATGTTGGGGATAGTAA-3′; HSL-F 5′-TGTCGGAGCCCATAGCAGA-3′, HSL-R 5′-GCATCCTCAGGTGGTAATAAGA-3′; LPL-F 5′-TAAAGTCAGAGCCAAAAGAAGC-3′; LPL-R 5′-CCACGGTGCCATACAGAGAAAT-3′). Cycling conditions were one cycle at 50°C for 2 min, 95°C for 10 min, followed by 40 cycles of 95°C for 15 sec and 60°C for 1 min. Duplicate experimental samples were quantified by comparison with standards of known concentrations. Expression of each gene was normalized to the housekeeping gene cyclophylin (cyclophylin-F 5′-CTTGGGCCGCGTCTCCTTC-3′, cyclophylin-R 5′-TGCCGCCAGTGCCATTAT-3′).
Liver histopathology
All liver biopsy specimens were reviewed by the same pathologist (P.S.B.) who was blinded to the patient's clinical and biochemical data. Scoring on a scale of 0–4 was carried out for steatosis, inflammation, and fibrosis according to criteria which have previously been described in detail. 25 A diagnosis of NASH was made on the basis of published criteria. 25
Stromal-vascular fraction primary culture
The effect of testosterone on secretion of IL-6 by cultured adipose tissue stromal-vascular cells was assessed. Because insufficient omental adipose tissue was available for stromal-vascular fraction harvesting and culture from women undergoing laparoscopic gastric band surgery, subcutaneous abdominal adipose tissue was obtained from healthy women aged <50 years (37±5 years, mean±standard deviation (SD); n=12) undergoing elective abdominoplasty. The study was approved by the institutional Human Research Ethics Committee, and patients gave written informed consent. Stromal-vascular fraction cells were isolated by collagenase digestion and primary cultures incubated in DMEM containing 10% fetal bovine serum (FBS; JRH, Lenexa, KS). At confluence, cultures were washed in phosphate-buffered saline (PBS); then duplicate wells were incubated in serum-free medium (DMEM +1% BSA) for 48 hr with vehicle (0.1% ethanol) or testosterone 10 nmol/L or 100 nmol/L. Medium was changed and collected after a further 24 hr. Medium IL-6 was measured by ELISA (R&D Systems).
Statistical analysis
Normality of data was tested using the D'Agostino and Pearson test. All continuous variables except for fasting serum insulin and HOMA-IR followed a normal distribution. Serum insulin and HOMA-IR were log-transformed for analysis; the nontransformed data in original units are presented. On the basis of our published 26 and unpublished data, the experiments using primary cultured stromal-vascular cells and omental explants, respectively, were powered (α=0.05) to detect a 20% change. Differences between groups were determined using the Student t-test or analysis of variance (ANOVA) with posttest (Tukey multiple comparison test). ANOVA with posttest for linear trend was used to analyze patient characteristics versus categories of liver histopathology. Correlations between variables were assessed using the Pearson correlation coefficient with Bonferroni correction applied for testing of multiple correlations. A P value of <0.5 was considered statistically significant. Statistical analyses were performed using GraphPad Prism version 5.02 (GraphPad Software, San Diego, CA).
Results
Patient characteristics
Twenty-seven women participated in the study. Seven women reported any degree of hirsutism requiring therapy, varying from occasional plucking of facial hair to regular waxing. The hirsute women did not fulfill National Institutes of Health (NIH) 1990 diagnostic criteria for PCOS 27 given they had regular menstrual cycles, but they may have been diagnosed with PCOS according to Rotterdam 2003 criteria 28 if polycystic ovary morphology was present. Pelvic ultrasound examination was not performed in this study.
As expected, the hirsute women had significantly higher serum total testosterone levels within the normal range and a tendency for higher free testosterone than the nonhirsute group. However, fasting glucose, insulin, SHBG, and HOMA-IR were similar to the nonhirsute women, suggesting that the hirsute group lacked the metabolic sequelae typical of PCOS 13 (Table 1). The three women with PCOS who were included to provide a reference point for serum androgen levels were comparable to the other study participants in age (36.6±3.3 years), body mass index (BMI) (41.5±2.0 kg/m2), and fasting glucose (4.7±0.1 mmol/L), but had higher fasting insulin (23±6.0 μU/mL) and HOMA-IR (2.9±0.6) values, although these differences did not reach statistical significance. Of the 27 participants, 18 were on no prescribed medications; four had hypertension and were treated with angiotensin-converting enzyme inhibitors (ACEI) or angiotensin receptor antagonists (ARB). Only one woman, also on an ARB, was taking a statin. Five women smoked cigarettes.
Note: fasting insulin and HOMA-IR are presented as median (interquartile range); other characteristics are mean±standard error of the mean (SEM).
The Student t-test.
BMI, body mass index; HOMA-IR, homeostasis model assessment of insulin resistance; SHBG, serum hormone-binding globulin.
Relationship between serum testosterone and adiol-glucuronide
Serum total testosterone was significantly higher in the women with hirsutism compared with the nonhirsute women (Fig. 1A). However, whereas serum adiol-glucuronide tended to be higher in the women with hirsutism compared with nonhirsute women, this did not reach statistical significance (Fig. 1B). For comparison, levels of total testosterone and adiol-glucuronide were also measured in women with PCOS; the serum testosterone was ∼70% higher than in the hirsute group, whereas adiol-glucuronide was similar. There was no correlation between serum total testosterone and adiol-glucuronide in the whole group (i.e., nonhirsute and hirsute women) (Fig. 1C). Similarly, there was no correlation between calculated free testosterone and adiol-glucuronide (data not shown). Serum total testosterone, free testosterone, or adiol-glucuronide did not correlate significantly with SHBG, fasting insulin, fasting glucose, or HOMA-IR (data not shown).
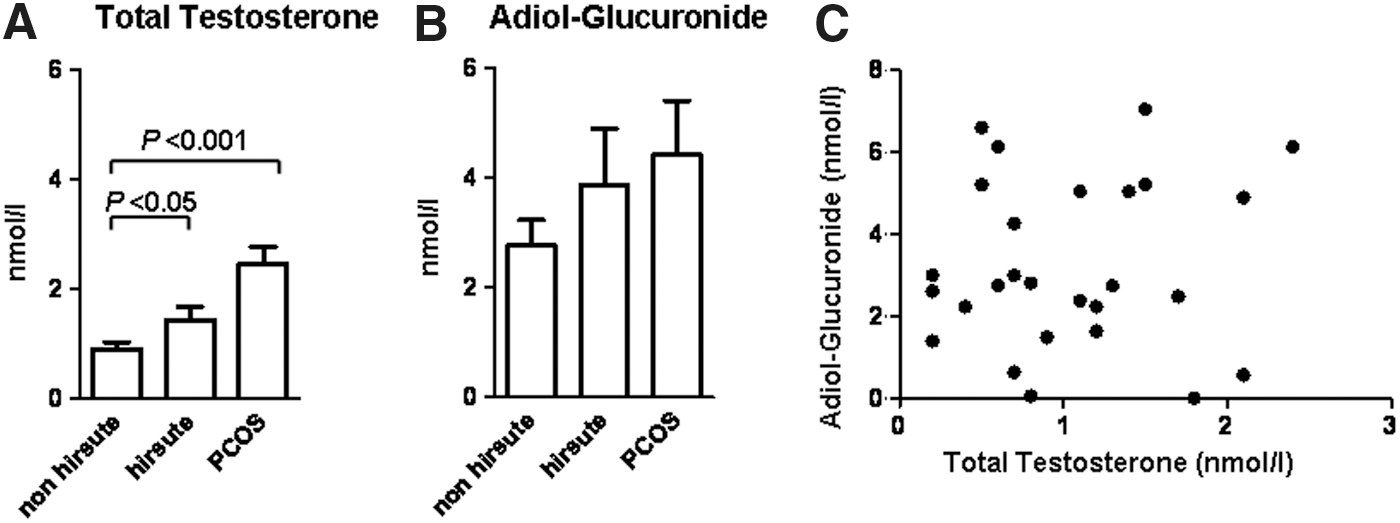
Serum total testosterone
Relationships between serum androgens and omental inflammation and lipid metabolism
Correlations were sought between serum total testosterone, free testosterone, and adiol-glucuronide with omental adipose tissue expression of proinflammatory cytokines (TNF-α, IL-6), a marker of macrophage lineage cells (CD68), and the anti-inflammatory adipokine adiponectin, as well as key enzymes involved in lipid metabolism (HSL and LPL). There was a significant positive correlation between serum adiol-glucuronide and expression of TNF-α in omental adipose tissue (P=0.03), but this did not remain significant after Bonferroni correction (data not shown). There was no correlation between serum total or free testosterone and TNF-α expression. Expression of IL-6, CD68, and adiponectin in omental adipose tissue did not correlate with serum total or free testosterone or adiol-glucuronide. Additionally, expression of HSL and LPL did not correlate with serum androgens. There was no relationship between expression of adiponectin and IL-6 or CD68. There was a trend toward an inverse relationship between expression of adiponectin and TNF-α (P=0.08)
Relationships between serum androgens and adipose tissue IL-6 secretion
Secretion of IL-6 at 24 or 48 hr from explants of omental adipose tissue did not correlate with serum levels of total or free testosterone or adiol-glucuronide (data not shown). To further investigate whether IL-6 secretion in adipose tissue was regulated by androgens, we examined the effect of testosterone (10 nmol/L or 100 nmol/L for 48 hr) on IL-6 secretion by primary cultures of stromal-vascular fraction cells. Testosterone had no effect on IL-6 secretion (Fig. 2).

Effect of testosterone on interleukin-6 (IL-6) secretion by primary cultures of stromal-vascular fraction cells harvested from abdominoplasty specimens of premenopausal women (n=11–12). Confluent cultures were treated with vehicle and testosterone 10 nmol/L or 100 nmol/L for 48 hr, and medium was collected after a further 24 hr. Medium IL-6 was measured by enzyme-linked immunoassay (ELISA), and results are expressed as a percentage of secretion by vehicle-treated cells.
Relationships between liver histopathology and omental adipose tissue metabolism
Liver biopsy data were available in 22 patients. These were grouped according to the severity of histological changes of NAFLD, i.e., Group 1=steatosis levels 0, 1 (i.e., nil steatosis or steatosis involving <5% of lobular parenchyma, n=10); Group 2=steatosis levels 2, 3, 4 (i.e., steatosis involving 5%–25%, 25%–75%, or >75% of lobular parenchyma, respectively, without inflammation or with nonspecific inflammation, n=9); Group 3=NASH (n=3). None of the liver biopsy specimens showed changes consistent with viral hepatitis. Only two patients had essentially normal liver biopsies (Group 1, steatosis level 0). Exclusion of these individuals from Group 1 did not alter the outcome of the analyses.
The characteristics of the patients in each group are shown in Table 2. The age of the participants was comparable. There was a nonsignificant increase in BMI in Group 3: One patient in this group had a BMI of 91 kg/m2. Retrospective exclusion of this patient from the study on the grounds of her BMI was deemed unjustifiable, given that she fulfilled all of the stringent inclusion criteria of the study. There was a significant trend for increase in serum free testosterone, insulin, and HOMA-IR across the three groups. Total testosterone, adiol-glucuronide, and glucose increased across the three groups and SHBG decreased, but did not reach statistical significance. Any degree of hirsutism was reported by three patients in Group 1 and by two patients in Group 2; in Group 3, none reported hirsutism. ACEI or ARB drugs were taken by nil patients in Group 1, two patients in Group 2 (one of whom was also on a statin), and one patient in Group 3.
One patient in this group had a BMI of 91.
Analysis of variance (ANOVA) with posttest for linear trend.
Note: fasting insulin and homeostasis model assessment of insulin resistance (HOMA-IR) are presented as median (interquartile range); other characteristics are mean±standard error of the mean (SEM).
NASH, nonalcoholic steatohepatitis; BMI, body mass index; SHBG, sex hormone-binding globulin; NS, not significant.
Expression of TNF-α, IL-6, CD68, adiponectin, HSL, and LPL was compared in the three groups (Fig. 3). There was a trend for a higher TNF-α expression in Group 2 compared with Group 1, but this did not reach significance (P<0.10). IL-6 and CD68 expression did not differ across the three groups. Adiponectin expression tended to be lower in Group 2 than in Group 1, but this did not reach significance (P<0.10). HSL expression did not differ across the groups. However, LPL expression was significantly higher in Group 3 than in Groups 1 or 2.

Omental adipose tissue gene expression of tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), CD68, adiponectin, hormone-sensitive lipase (HSL), and lipoprotein lipase (LPL) in women with minimal or no steatosis on liver biopsy (Group 1; n=9–10), women with moderate to severe hepatic steatosis but no inflammation (Group 2; n=5–9), or women with nonalcoholic steatohepatitis (NASH) (Group 3, n=3). Gene expression was measured by real-time PCR, and each result normalized to expression of cyclophylin. LPL expression was significantly higher in the omental adipose tissue of women with NASH compared with women with milder degrees of nonalcoholic fatty liver disease (NAFLD) (P<0.05, analysis of variance (ANOVA) with Tukey multiple comparison test).
Secretion of IL-6 from omental explants as measured at 24 or 48 hr did not differ between Groups 1 and 2 (Fig. 4). Group 3 was not included in this analysis because measurement of omental explant IL-6 secretion was available in only one patient from this group.
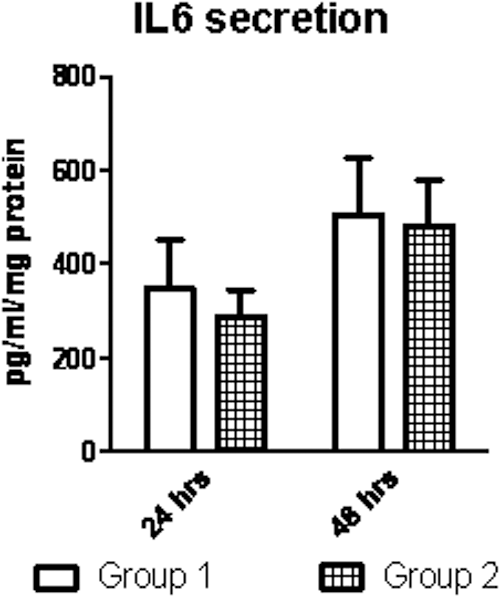
Interleukin-6 (IL-6) secretion at 24 and 48 hr by omental adipose tissue explants obtained from women with minimal or no steatosis on liver biopsy (Group 1; n=8) and women with moderate-to-severe hepatic steatosis but no inflammation (Group 2; n=9).
Discussion
Little information exists on whether androgen levels within the normal range have implications for metabolic dysfunction in women. Understanding the role of sex hormones may provide insight into the pathogenesis of common metabolic disorders, such as glucose intolerance and NAFLD, and potentially indicate new therapeutic targets for these conditions. This study examined this question in a selected group of premenopausal women who were obese, nondiabetic, had regular menstrual cycles, and had no significant biochemical androgen excess. Measurement of serum testosterone is problematic in women due to lack of accuracy and sensitivity of many commercially available assays. 23 The testosterone radioimmunoassay used in this study has been shown to correlate well with measurement of testosterone by liquid chromatography/mass spectrometry, 23 considered to be the preferred assay method. 29
We also measured androstanediol glucuronide (adiol-glucuronide) as a marker of androgen metabolism in peripheral tissues such as adipose tissue, as well as exposure of the liver to androgen metabolites for glucuronide conjugation. 30 In women, synthesis of testosterone in peripheral tissues accounts for a significant proportion of total testosterone production: It is estimated that only 10%–15% of testosterone diffuses from these tissues into the circulation without prior metabolism to the more biologically active DHT. 31 DHT is inactivated in adipose tissue 32 to form the metabolites androstane-3α,17β-diol, and androstane-3β,17β-diol, glucuronide conjugation of which occurs in the liver. Serum testosterone is therefore mainly a measure of testosterone directly secreted by ovaries and adrenals and does not reflect total body production or tissue levels in women. 31 Obesity in women is associated with markedly increased production rates of testosterone, DHT, and androstanediol, but clearance rates are also increased, probably due to inactivation in adipose tissue, resulting in normal serum levels. 33
As expected, we found no correlation between serum adiol-glucuronide and testosterone levels. However, none of the clinical metabolic parameters (serum insulin, HOMA-IR, etc.) or expression of omental genes associated with inflammation correlated with either serum testosterone or adiol-glucuronide. Accordingly, we found that IL-6 secretion by omental adipose explants did not correlate with serum androgens. Consistent with this correlative data, we found that testosterone did not influence IL-6 secretion from cultured stromal-vascular fraction cells. Four women in our study were taking ACEI or ARB drugs for management of hypertension; although there is accumulating evidence that inhibition of the renin–angiotensin–aldosterone system is associated with anti-inflammatory effects in adipose tissue, 34 we think it is unlikely that this small number of women on ACEI/ARB significantly influenced our results. Our data imply that, at least in obese women without classic PCOS, physiological-range androgen levels do not exert significant influence on inflammation in adipose tissue. An alternative conclusion would be that due to increased rates of production and clearance of androgens in obese women, 33 direct measurement of androgen concentrations within adipose tissue are necessary to determine relationships between androgens and tissue metabolism. A more direct experimental approach would be to study the effects of androgens on adipose tissue macrophages, the major mediators of the immune response in adipose tissue, but this was beyond the scope of our study. Our data are consistent with a recent study showing that chronic suppression of serum androgens using gonadotropin-releasing hormone (GnRH) agonist therapy did not influence serum IL-6 levels in obese ovulatory women, 35 although interestingly in obese women with PCOS, serum IL-6 levels increased, consistent with an anti-inflammatory effect of androgens in this group.
We found no correlation of serum testosterone or adiol-glucuronide with expression of omental LPL or HSL. LPL releases lipolytic products from chylomicra and very-low-density lipoproteins that are taken up by adipocytes for deposition as triacylglycerol; thus, LPL is a key regulator of lipid accumulation. 36 HSL catalyzes the rate-limiting step of adipose tissue lipolysis, i.e., the hydrolysis of triacylglycerol to diacylglycerol, then monoacylglycerol. 37 In men, in vivo and in vitro studies have shown that testosterone inhibits adipose tissue LPL activity. 38 In vitro studies, generally using pharmacological androgen concentrations, suggest that androgens also regulate lipid metabolism in women. Androgens inhibited LPL activity in omental adipose tissue explants but had no effect in subcutaneous adipose tissue of women. 4 Conversely, androgens stimulated LPL protein expression in subcutaneous adipocytes. 1 In subcutaneous adipocytes of women, androgens inhibited HSL protein expression, 1,2 catecholamine-stimulated lipolysis, and expression of β2-adrenoceptors, with no effect on visceral adipocytes. 2 Few in vivo studies in females have been published. Administration of testosterone enhanced the antilipolytic effect of insulin in postmenopausal women. 39 Treatment of ovariectomized female mice with DHT increased the expression of LPL in visceral adipose tissue, 40 suggesting that in the postmenopausal state androgen excess may contribute to accumulation of visceral fat.
The pathophysiology of NAFLD has been the subject of extensive investigation. 41 Women with androgen excess due to PCOS have increased risk of NAFLD, but whether this is related to insulin resistance or androgens or both is unknown. As expected, we found that increasing severity of NAFLD was associated with a significant trend to increasing insulin resistance. Consistent with studies showing an inverse relationship between liver fat content and SHBG levels, 42,43 the mean SHBG concentration in the women with NASH was ∼60% of that in women with minimal or no hepatic steatosis, although this difference did not reach statistical significance. There was a significant trend to higher serum-free testosterone with worsening liver pathology, and a similar but nonsignificant trend to increased total testosterone and adiol-glucuronide. Our findings are similar to those reported in women with PCOS in whom increased bioavailable testosterone was associated with higher risk of NAFLD 18,19 and raise the possibility that androgens may also be relevant to the pathogenesis of NAFLD in women without PCOS.
Given the direct drainage of free fatty acids (FFA) and cytokines from the omentum to liver via the portal vein, 44 omental adipose tissue metabolism in patients with NAFLD is of particular interest. NAFLD has been shown to be associated with increased macrophage accumulation, 45 deregulation of genes related to inflammation, 46 alteration of pathways related to insulin signaling, 47 and increased lipolysis 48 in omental adipose tissue. We examined expression of genes related to inflammation in omental adipose tissue and also IL-6 secretion by omental explants and found no significant differences in women grouped according to severity of NAFLD. This unexpected finding could be due to insufficient patient numbers or to the highly selected population of obese women included in this study. Although omental HSL expression did not differ according to liver histology, omental LPL expression was significantly increased in women with NASH compared with women with less severe NAFLD. Increased LPL expression implies greater capability for accumulation of lipid by omental adipose tissue and is therefore likely to be relevant to the risk of developing NAFLD. Insulin is a major positive regulator of LPL, 49 and higher insulin levels in the NASH group may account for the increase in LPL expression. Alternatively, increased LPL expression may be due to other unidentified factors, resulting in increased lipid accumulation, worsening of insulin resistance, and thus increased insulin levels.
Our study has several important limitations. Although we had extensive clinical information on the participants, this was incomplete; we did not measure waist circumference, and participants did not undergo an oral glucose tolerance test or have plasma lipids assessed. We found no relationship between physiological androgen levels and expression of lipid metabolic genes in omental adipose tissue of women, but we did not measure LPL or HSL protein expression or activity. Additionally, adipocyte lipolysis is a complex process regulated at multiple levels by pathways in addition to the classic G-protein-coupled receptor–modulated cAMP-dependent pathway. 50 Further studies are required to examine the effect of androgens on these signaling pathways. Markers of inflammation in omental adipose tissue did not differ in women grouped according to severity of NAFLD; small participant numbers, especially in the group of women with NASH, may have influenced this outcome.
In conclusion, in obese premenopausal women without significant biochemical androgen excess, there was no relationship between serum androgens and markers of inflammation in omental adipose tissue. In contrast to in vitro studies using supraphysiological androgen concentrations, we found no relationship of serum androgens with omental expression of LPL or HSL. There was a significant trend to higher serum free testosterone, serum insulin, and insulin resistance with increasing severity of NAFLD, but markers of inflammation in omental adipose tissue did not differ. Omental LPL expression was significantly increased in women with NASH, implying a greater capacity for omental lipid accumulation. These data suggest that physiological-range androgen levels do not exert significant influence on inflammation or lipid metabolism in omental adipose tissue of women. However, it remains possible that androgens play a role in the pathogenesis of NAFLD in women via mechanisms unrelated to omental adipose tissue metabolism.
Footnotes
Acknowledgments
This work was supported by Diabetes Australia Research Trust. A.C. is the recipient of a National Health and Medical Research Council (NHMRC) Australia Health Professional Research Fellowship. The authors acknowledge Dr. Joseph Montalto PhD, Dorevitch Pathology, Heidelberg, Victoria, for validation of the serum testosterone assay.
Author Disclosure Statement
No competing financial interests exist for all authors.