
Abstract
Background:
This study sought to explore the relationship between cystatin C (CysC) and anthropometric measures of obesity and the influence of this association on mortality [cardiovascular disease (CVD), coronary heart disease, and all-cause] in a nationally representative population free of CVD, diabetes mellitus, and macroalbuminuria (MA).
Methods:
The study cohort included 4577 adult participants of the Third National Health and Nutrition Examination Survey (NHANES). Spearman correlation analysis was performed to ascertain the association between various anthropometric measures and CysC. Formal statistical analyses of the interaction term between anthropometric measures and CysC for outcomes were performed followed by stratified multivariate Cox proportional hazard analyses.
Results:
A moderate degree of association was seen between CysC and measures of visceral adiposity as represented by waist-to-height ratio (WHR) and waist circumference (WC) and only a weak association between CysC and body mass index (BMI). CysC was predictive of all study outcomes in individuals with normal anthropometric measurements only.
Conclusions:
CysC correlated better with measures of visceral adiposity (WC and WHR) compared to BMI and appears to be a better predictor of adverse cardiovascular outcomes among those with anthropometric measures not suggestive of obesity compared to those with abnormal measures of anthropometry.
Introduction
C
The main objectives of our study were two-fold: (1) To explore the relationship between CysC and anthropometric measures of obesity and (2) to further evaluate the influence of this association, if any, on mortality in a nationally representative population free of CVD, diabetes mellitus, and macroalbuminuria (MA) with creatinine-estimated glomerular filtration rate (eGFR) ≥60 mL/min per 1.73 m2.
Methods
Study population
The study cohort was derived from National Health and Nutrition Examination Survey (NHANES) III, which was conducted by the National Center for Health Statistics of the Centers for Disease Control and Prevention from 1988 to 1994. The study cohort included adult participants representative of a civilian, noninstitutionalized US general population. CysC was measured on a sample of 6951 subjects including all NHANES III subjects aged 60 years and a random sample of those aged 20–59 years. For the purpose of our study, subjects with missing information on study variables were excluded, leaving a sample size of 4577. A detailed description of the study design is described elsewhere. 12 –14
Data collection
Data were collected by trained personnel according to standardized procedures. Information for age, sex, and smoking (defined as lifetime smoking of ≥100 cigarettes) was self-reported. Hypertension was defined as an average systolic blood pressure (SBP) of 140 mmHg, a diastolic blood pressure (DBP) of 90 mmHg, a physician's diagnosis, or the use of antihypertensive medication. Diabetes mellitus was either self-reported or identified by the use of diabetic medications, a nonfasting plasma glucose of 200 mg/dL, or a FPG of 126 mg/dL.
Laboratory measurements
CysC was measured using a particle-enhanced immunonephelometric assay (N Latex Cys-C, Dade Behring, Deerfield, IL) using the serum from fasting blood samples, which was stored at −70°C until analyzed at the Cleveland Clinical Research Laboratory. Lipid parameters, C-reactive protein (CRP), urinary albumin, and creatinine were analyzed by standardized laboratory methods, further details of which have been published previously. 12 –14
Statistical analysis
Spearman correlation analysis was performed to ascertain the association between various anthropometric measures and CysC. Formal statistical analyses of the interaction term between anthropometric measures and CysC for outcomes were performed followed by stratified multivariate Cox proportional hazard analyses. Outcomes were defined as follows: All-cause mortality=Death due to any cause, CVD mortality=Death due to any cardiovascular disease only, and coronary heart disease (CHD) mortality=Death due to ischemic heart disease only. The International Classification of Diseases (ICD), 10th version, was used by National Center for Health Statistics, where the National Death Index (NDI) was used to ascertain mortality status (median follow-up duration, 14.5 years). ICD codes 53–75 were used to define CVD mortality and ICD codes 58–63 were used to define CHD mortality.
Results
The baseline characteristics of study population across strata of anthropometric measures are shown in Table 1. The individuals with abnormal anthropometric measures were more likely to be older, hypertensive with higher total cholesterol (TC) and lower high-density lipoprotein cholesterol (HDL-C), and more likely to be on lipid-lowering therapy. The values of CRP and CysC also tended to be higher in subset of individuals with abnormal anthropometric indices.
Figure 1 depicts the Spearman correlation analysis between CysC and anthropometric measures. A moderate degree of association was seen between CysC and measures of visceral adiposity as represented by WHR (rho 0.32, p<0.001) and WC (rho 0.34, p<0.001). There was only a weak association between CysC and BMI (rho 0.15, p<0.001). Table 2 shows the predictive association of CysC with mortality across strata of anthropometric measures. As shown, CysC was predictive of all outcomes including CHD [hazard ratio (HR) 3.25, 95% confidence interval (CI) 2.14–4.94, p<0.001], CVD mortality (HR 3.07, 95% CI 2.12–4.45, p<0.001), and death (HR 2.16, 95% CI 1.58–2.96, p<0.001) in individuals with normal WC. Similarly, CysC was also predictive of CHD (HR 2.75, 95% CI 2.02–3.75, p<0.001), CVD mortality (HR 2.87, 95% CI 2.25–3.66, p<0.001), and death (HR 1.90, 95% CI 1.53–2.34, p<0.001) in individuals with normal WHR and normal BMI (HR 3.01, 95% CI 2.20–4.31, p<0.001; HR 2.99, 95% CI 2.27–3.94, p<0.001 for CVD; HR 1.98, 95% CI 1.56–2.51, p<0.001 for death). Of note, the above analyses were adjusted for age, sex, race, traditional cardiovascular risk factors such as SBP, antihypertensive medications, history of smoking, HDL-C, TC, lipid-lowering therapy, and CRP. Furthermore, similar results were obtained on adding creatinine to the multivariable model (see Table S1; Supplementary Data are available at
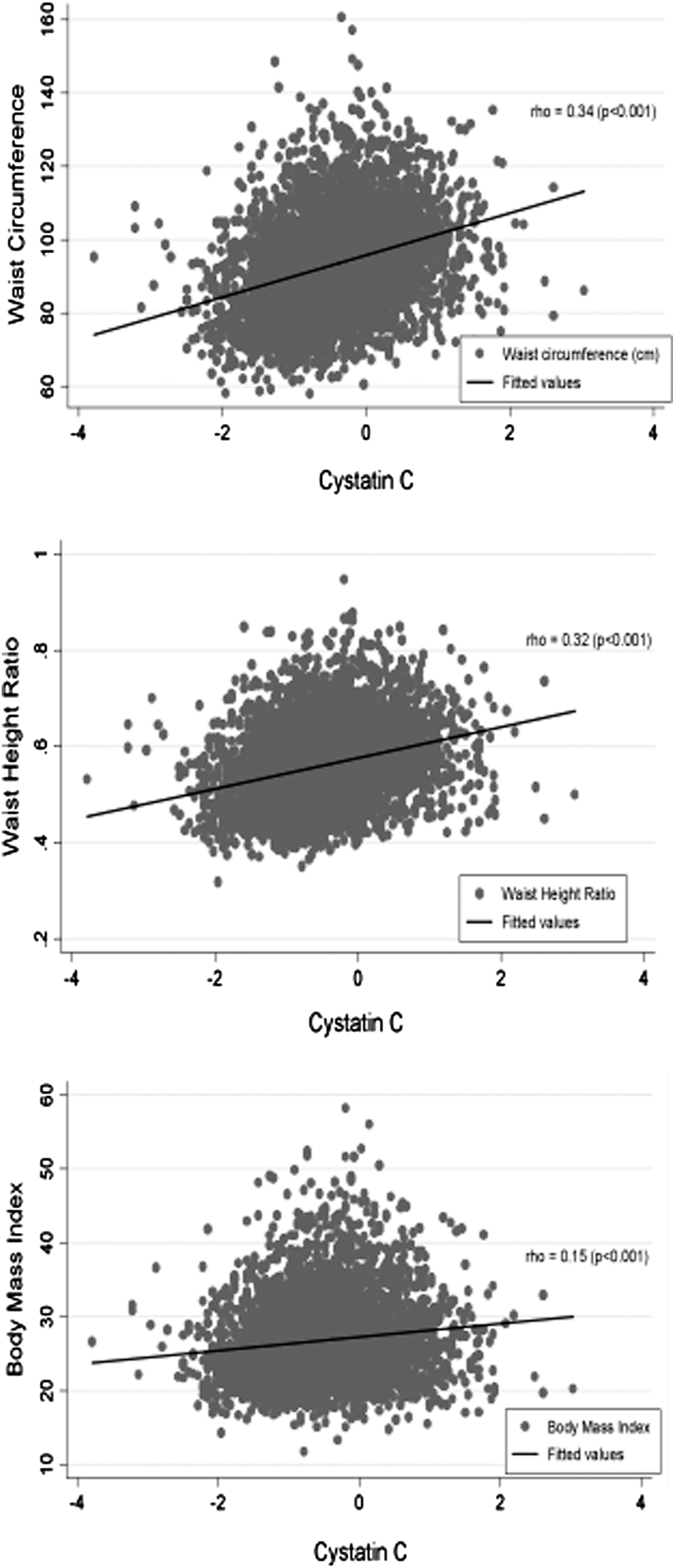
Spearman correlation analysis between cystatin C (CysC) and measures of anthropometry. CysC has a moderate degree of association with waist circumference and waist-to-height ratio and only a weak association with body mass index. CysC was transformed as standard deviation (SD) change of log(CysC) to normalize distribution.
CysC was transformed as SD change of log(CysC) to normalize distribution.
Interaction terms between CysC and all three measures of anthropometry were statistically significant (P<0.05).
CysC was adjusted for age, sex, race, systolic blood pressure, antihypertensive medications, history of smoking, high-density lipoprotein cholesterol, total cholesterol, lipid-lowering therapy, and log(CRP).
HR, hazard ratio; CI, confidence Interval; CysC, cystatin C; CRP, C-reactive protein; CHD, coronary heart disease; CVD, cardiovascular disease.
Discussion
Our study is the first to report an association between CysC and various anthropometric measures and the impact of this association on mortality. In our study cohort, CysC had a moderate degree of association with measures of central obesity including WC and WHR and only a weak association with general obesity or BMI. Furthermore, CysC was predictive of all-cause and cardiovascular mortality only in subjects with normal anthropometric measurements.
CysC has been previously associated with various cardiovascular risk factors, 15 especially hypertension, 16 subclinical CVD, including left ventricular hypertrophy, 17 as well as hard cardiovascular outcomes in multiple population cohorts. 1,5,18 In a recent report, CysC was shown to be strongly associated with all-cause and cardiovascular mortality in a cohort of patients referred for coronary angiography. 19 Its ability to reliably predict preclinical renal disease 20 as well as its plausible role in inflammation and atherogenesis 21 may explain its utility in the prognostication of CVD mortality. Indeed, published studies have reported severely reduced CysC levels and correspondingly increased activity of the cysteine proteases (cathepsins K and S) in atherosclerotic and aneurysmal lesions 22 with deregulated arterial integrity during experimental atherogenesis. 23 Apparently, ischemic, pressure/volume overload or toxic insult could lead to alterations in the cardiac extracellular/collagen matrix via disturbances in cathepsins and cystatins with resultant structural myocardial remodeling that eventually culminates as ventricular dysfunction. 23 In this context, studies have reported reductions in CysC levels with angiotensin receptor blocker (ARB) therapy in parallel with salutary improvements in blood pressure, vascular resistance, and regression of left ventricular hypertrophy. 24
Visceral obesity is more deleterious than general obesity and has been associated with proatherogenic elements, such as insulin resistance, the metabolic syndrome, dysglycemia, and dyslipidemia. 25 Furthermore, visceral fat seems to play a role in inflammation and is thus involved in the pathogenesis of atherosclerosis. 25,26 Indeed, visceral adipoctyes are believed to release more inflammatory cytokines like interleukin-6 than subcutaneous fat cells. 27 When compared to WC and WHR, BMI has a poor specificity for excessive adiposity 28 and is believed to underestimate visceral obesity. A stronger association of CysC with anthropometric measures of visceral/central obesity in our study reiterates the plausible role of this biomarker in inflammation and atherogenesis. Indeed, high CysC levels previously have been demonstrated to predict development of metabolic syndrome 29 and adversely affect metabolic factors, including abdominal obesity.
In our study, CysC was predictive of cardiovascular and all-cause mortality only in individuals with normal anthropometric measures, thereby highlighting its potential utility in this patient population. The lack of predictive value in individuals with abnormal anthropometric indices could be explained on the basis of risk factor clustering in these subjects, which might have diluted the significance of CysC in this population. In the current study, this subset of individuals was more likely to have a higher burden of traditional risk factors at baseline (Table 1), which is consistent with previous studies that have shown a positive association between obesity and cardiometabolic risk factors. 25 Our observations are nonetheless particularly relevant because they help identify a subset of the population without central obesity or traditional risk factors that are at risk for an adverse cardiovascular event, implicating the possibility of an obesity-independent mechanism at play. Our observations comport with a recent report showing higher CysC levels to be associated with early coronary atherosclerosis (noncalcified plaques) detected on multidetector computerized tomographic angiography in individuals independent of renal dysfunction or cardiovascular risk factors. 30
Our study has certain limitations. Given the cross-sectional design of the study, directions of causality need to be interpreted carefully. Hip circumference was not available, precluding the appraisal of an association between WHR and CysC. Nonetheless, a large sample size of an ethnically diverse nationally representative population free of baseline CVD or significant renal disease with comprehensive adjustments for potential confounders are some of the notable strengths of our study.
CysC correlated better with measures of visceral adiposity (WC and WHR) compared to general obesity (BMI) and appears to be a better predictor of adverse cardiovascular outcomes among those with anthropometric measures not suggestive of obesity compared to those with abnormal measures of anthropometry. Future studies should potentially focus on the prospective evaluation of CysC as a cardiovascular risk marker in low-risk individuals, especially those with normal indices of visceral adiposity. Future research should also be directed at better characterizing the precise pathogenetic underpinnings of how CysC mediates cardiovascular risk in the subset of the population without visceral obesity as well as to ascertain whether the risk is modifiable.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.