
Abstract
Background:
The healthy immigrant effect is a phrase that has been used for decades to describe better cardiometabolic health in African immigrants than African Americans. The recent global increase in cardiometabolic diseases raises the possibility that immigrant health may be changing. Therefore, a new assessment of cardiometabolic health in African immigrants is warranted.
Methods:
Glucose tolerance status, blood pressure, and visceral adipose tissue (VAT) volume were compared in 214 self-identified healthy men comprised of 138 African immigrants, 76 African Americans, mean age 36±9 years [mean±standard deviation (SD); range 20–64 years]. Insulin resistance was defined by the lowest quartile of the insulin sensitivity index (SI≤2.28 mU/L−1·min−1). The waist circumference (WC) which predicts insulin resistance was determined using receiver operating characteristic curves and the Youden index.
Results:
Body mass index (BMI) and WC were lower in African immigrants than African Americans (BMI, 27.4±3.8 vs. 29.3±5.5 kg/m2, P<0.01; WC, 91±11 vs. 97±16 cm, P<0.01). However, blood pressure, fasting glucose, and 2-hr glucose were higher in the African immigrants (all P<0.01). In addition, African immigrants had a higher prevalence of previously undiagnosed diabetes (8% vs. 0%, P<0.01) and prediabetes (35% vs. 22%, P<0.01). After adjusting for WC, African immigrants had more visceral adipose tissue (VAT) than African Americans (P<0.01). Consequently, the WC that predicted insulin resistance was 92 cm in African immigrants but 102 cm in African Americans.
Conclusion:
African immigrants were less obese than African Americans but had worse cardiometabolic health, specifically higher glucose levels, more hypertension, and greater visceral adiposity. Overall, the healthy immigrant effect may no longer be valid.
Introduction
D
Historically, the view has been that Africans acquired obesity, type 2 diabetes mellitus (T2DM), and cardiovascular disease only after living in the United States. 1 However, an epidemic of cardiometabolic disease is occurring in Africa. 4 –6 According to the International Diabetes Federation (IDF), by the year 2030, 28 million Africans will have T2DM and 63 million will have prediabetes. 7 This represents a 90% increase in diabetes and prediabetes, the highest anticipated increase in the world. 7 Therefore, it is reasonable to expect that a significant number of Africans will have cardiometabolic disease prior to immigration.
Our goal was to evaluate the current status of the healthy immigrant effect concept by comparing cardiometabolic risk factor prevalence in African immigrants and African Americans. Furthermore, because diabetes is related to both central obesity and insulin resistance, we compared body size and fat distribution, as well as the waist circumference (WC), which best predicts insulin resistance in both groups.
Materials and Methods
Two hundred and fourteen self-identified healthy men [138 African immigrants, 76 African Americans; age range, 20–64 years; body mass index (BMI) range, 18.5–46.0 kg/m2] enrolled in the protocol Diabetes and Heart Disease Risk in Blacks. African immigrants enrolled in this protocol are known as the African Immigrants in America cohort. All participants lived in the Washington, DC, metropolitan area. African immigrants reported that both they and their parents were born in western (49%), central (30%), or eastern (21%) Africa. African Americans were born in the United States with both parents identifying as African Americans born in the United States. Data from 39 African immigrants and 68 African Americans have been reported previously.
8,9
Recruitment was by flyers and newspaper advertisements. Participants denied a history of human immunodeficiency virus (HIV) infection and symptoms of diabetes such as polyuria, polydipsia, or recent weight loss. Participants denied taking medications, vitamins, or dietary supplements that influence glucose or lipid metabolism. The study was approved by the NIDDK Institutional Review Board (
The study was designed to have three outpatient visits within 1 month. At visit one, a medical history and physical examination were performed, and an electrocardiogram (EKG) and blood samples were obtained to ensure an absence of anemia or kidney, liver, or thyroid dysfunction. For visits two and three, participants arrived to the Clinical Center at 7 AM after a 12-hr fast. Visit 2 was designed to determine the lipid profile, abdominal fat distribution, and glucose tolerance status with a 2-hr oral glucose tolerance test (OGTT; Trutol 75, Custom Laboratories, Baltimore, MD). 10 WC was measured according to National Health and Nutrition Examination Survey (NHANES) guidelines at the level of the superior border of the iliac crest. 11 Visceral adipose tissue (VAT) and subcutaneous adipose tissue (SAT) volumes were determined with computerized tomographic (CT) scans.
At visit 3, a frequently sampled intravenous glucose tolerance test (FSIGT) was performed. An intravenous catheter was placed in each antecubital vein, and baseline samples were obtained. Dextrose (0.3 gram/kg) was administered intravenously over 1 min. Insulin was infused from 20 to 25 min (4 mU·kg−1·min−1). Samples for glucose and insulin were drawn at −10, −1, 0, 1, 2, 3, 4, 5, 6, 7, 8, 10, 12, 14, 16, 19, 22, 23, 24, 25, 27, 30, 40, 50, 60, 70, 80, 90, 100, 120, 150, and 180 min. Glucose and insulin concentrations were entered into the minimal model for calculation of the insulin sensitivity index (SI) (MinMOD Millenium v.6.02). 12 Beta-cell secretion was assessed by acute insulin response to glucose (AIRg). 12 The disposition index (DI), which is the product of AIRg and SI, was used to determine whether beta-cell secretion was sufficient to compensate for the degree of insulin resistance. 12
Twenty-five African immigrants and seven African Americans did not have an FSIGT. Eleven Africans did not have an FSIGT because their OGTT revealed previously undiagnosed T2DM. The remaining 14 African immigrants and seven African Americans did not have an FSIGT due to scheduling issues.
Analytic measures
Glucose concentrations were determined with the glucose oxidase method (YSI, Yellow Springs, Ohio). Insulin levels were measured with double-antibody chemiluminescent sandwich assays (Diagnostic Products, Los Angeles, CA). Coefficients of variation for the glucose and insulin assays were 1.9% and 3.2%, respectively. Cholesterol, triglycerides (TG), and high-density lipoprotein cholesterol (HDL-C) were measured on a Dimension Vista 1500 (Siemens, Newark, DE). Coefficient of variations for cholesterol, TGs, and HDL-C were 2.5%, 3.0%, and 2.5%, respectively. Low-density lipoprotein cholesterol (LDL-C) was calculated using the Freidewald equation. 13
Abdominal CT measurements
CT scanning parameters were 5- to 10-mm slice thickness, 0.7–0.98 in-plane pixel resolution, and 120 kVp. Adipose tissue volumes were assessed at L2–L3 using automated software. 14 The algorithm consisted of body masking, noise reduction, adipose tissue labeling, VAT and SAT separation, and quantitation. The body mask was created by a region-growing algorithm on the image background that segmented the low-intensity pixels outside the body and in a second pass removed the CT table. Once the body mask was created, an anisotropic diffusion filter reduced noise and voxels between −274 Hounsfield units (HU) and −49 HU. A contour around the outside of the body, the “external contour,” was initialized. Active contour models were then used to modify the external contour iteratively to find the inner boundary of the SAT; this resulted in a contour along the abdominal wall, specifically the “internal contour.” The adipose tissue volume inside the internal contour contributes to the VAT and the adipose tissue volume between the external contour and internal contour contributes to SAT. Six men (three African Americans and three Africans) did not have CT scans.
Statistics
Data are presented as mean±standard deviation (SD). P values ≤0.05 were considered significant. Comparisons were by the Student t-test, one-way analysis of variance (ANOVA) with Bonferroni corrections, or the chi-squared test. The association between VAT and SAT with WC was determined with Pearson correlations. Multiple regressions were performed. Independent variables were WC, ethnicity, and a term for interaction between ethnicity and WC. Dependent variables were either VAT or SAT.
SI was not significantly different in African immigrants and African Americans (P=0.90) or among West, Central, and East Africans (P=0.88). Therefore, the entire cohort was divided into quartiles of SI. The lowest quartile of SI was used to define insulin resistance (≤2.28 (mU/L)−1·min−1). An area under the receiver operating characteristic (AUC-ROC) curve was calculated to determine if WC could predict insulin resistance. The Youden index was used to determine the WC threshold with the optimal combination of sensitivity and specificity. Analyses were performed with STATA (v. 13.0, College Station, Texas).
Results
Analyses of social, demographic, and metabolic data revealed many differences between African immigrants and African Americans (Table 1). In contrast, the West, Central, and East Africans were similar to each other in every variable except for age. As a group, West Africans were 5 years older than Central and East Africans (Table 1). However, age did not differ between African Americans and Central and East Africans.
Continuous variables: unpaired t-test; categorical variables: chi-squared test.
Continuous variables: one-way analysis of variance (ANOVA); categorical variables: chi-squared test.
Comparison between African Americans and Africans adjusted for WC.
One drink at least once a week.
SD, standard deviation; BMI, body mass index; WC, waist circumference; VAT, visceral adipose tissue; SAT, subcutaneous adipose tissue; SI, insulin sensitivity index; AIRg, acute insulin response to glucose; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol.
Social characteristics
African immigrants were more likely than African Americans to be married, college educated, and nonsmokers. African immigrants were less likely than African Americans to engage in vigorous physical activity (≥30 min, three times/week) or have health insurance. Median income and alcohol intake were similar.
Age at immigration
Eighty-four percent of Africans arrived in the United States as adults (age ≥20 years), 8% as teenagers (age 13–19 years), and 8% as children (age [≤12 years). Length of residence in the United States was 11±9 years, range 0.1–42 years. For Africans who immigrated as adults, 83% reported weight gain after living in the United States, 6% reported no weight change, and 11% reported weight loss.
Body size and related metabolic characteristics
BMI and WC values were lower in African immigrants than African Americans (Table 1), but, after adjusting for either BMI or WC, African immigrants had more VAT and less SAT (P<0.01) (Table 1). Systolic blood pressure (SBP) and diastolic blood pressure (DBP) was higher in African immigrants than African Americans (Table 1). Fasting and 2-hr glucose levels were also higher in African immigrants. Therefore, African immigrants had a higher prevalence of previously undiagnosed T2DM (8% vs. 0%, P<0.01) and prediabetes (35% vs. 22%, P<0.01). However, the glucose patterns in African immigrants and African Americans with abnormal glucose tolerance were similar such that for both groups approximately 7% had elevated fasting glucose, 67% had elevated 2-hr glucose, and 27% had both elevated fasting and 2-hr glucose. SI did not differ by ethnicity, but AIRg and the DI were lower in African immigrants (Table 1).
Neither African immigrants nor African Americans were hyperlipidemic. TG and HDL-C concentrations did not vary by ethnicity, but total cholesterol and LDL-C were lower in African immigrants (Table 1).
Relationship of WC to abdominal fat
The correlation between BMI and WC was highly significant in both African immigrants (r=0.89, P<0.01) and African Americans (r=0.92, P<0.01). However, there were key differences in the distribution of abdominal fat between the VAT and SAT compartments. At the same WC, African immigrants had more VAT (Fig. 1A) and less SAT (Fig. 1B) than African Americans. This was confirmed by multiple regression analyses. Table 2 (model A) shows that as WC increases, the increase in VAT is greater in African immigrants than African Americans (5.42 vs. 3.50, P<0.01). This finding was replicated when the African immigrants were divided by region of origin and each group compared to African Americans (Table 2, models B, C, and D).

Central body fat distribution.
African Americans are the referent group.
SE, standard error.
The situation was reversed with SAT. There was a significant interaction between WC and ethnicity. This means that as WC increases, the increase in SAT is greater in African Americans than African immigrants (8.62 vs. 6.26, P<0.01) (Table 2, model E). This remained true when the African immigrants were divided by region of origin and each group compared to African Americans (data not shown).
The ability of WC to predict insulin resistance
The AUC- ROC curve for the ability of WC to predict insulin resistance for African immigrants was 0.77±0.05 [95% confidence interval (CI) 0.66–0.87] (Fig. 2A) and for African Americans it was 0.76±0.07 (95% CI 0.62–0.91) (Fig. 2B). By region of origin, the AUC-ROC curve for the ability of WC to predict insulin resistance in West Africans was 0.69±0.09 (95% CI 0.52–0.86), in Central Africans it was 0.80±0.08 (95% CI 0.65–0.95), and East Africans it was 0.92±0.06 (95% CI 0.80–0.99).
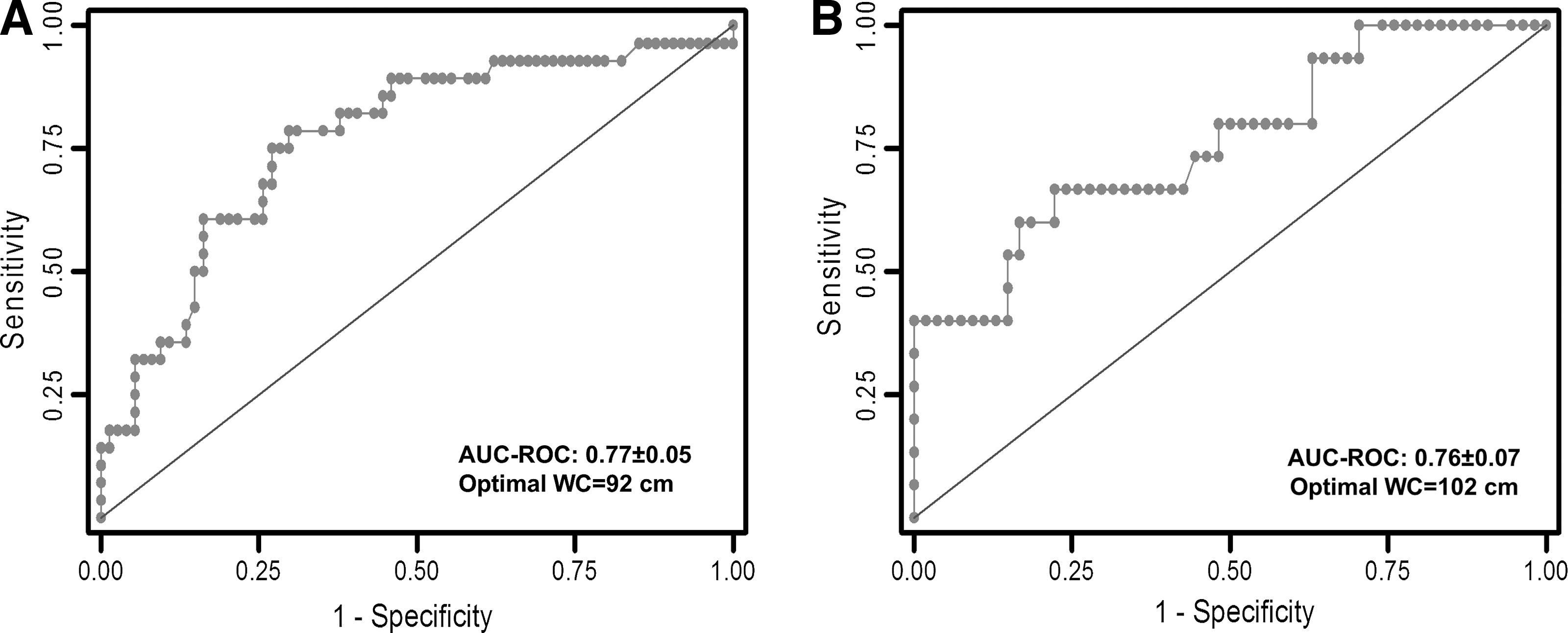
Waist circumference of risk predictions. Area under the receiver operating characteristic (AUC-ROC) curve for the ability of waist circumference (WC) to predict insulin resistance is shown. Optimal WC calculated by the Youden index is provided.
The WC threshold that optimally predicts insulin resistance
The Youden index revealed that the WC that optimally predicted insulin resistance was 92 cm in African immigrants and 102 cm in African Americans. By region of origin, the WC values that best predicted insulin resistance in West, Central, and East Africans were 92 cm, 91 cm, and 96 cm, respectively.
Discussion
On the basis of evaluation of glucose tolerance, beta-cell function, visceral adiposity, blood pressure, and BMI, we report that African immigrant men were less obese but had worse cardiometabolic health than African American men. Most striking was the finding that African immigrant men had higher rates of diabetes and prediabetes. Worse glucose tolerance in the African immigrants than African Americans may be explained by greater visceral adiposity and more beta-cell failure. Support for this concept comes from reports from the Pennington Longitudinal Study, the Dallas Heart Study, and cohorts of Japanese Americans. 15,16,17 –21 These investigations have revealed that VAT mass is associated with cardiac risk factors and predictive of diabetes and cardiovascular disease. 15 –21
In addition, we found that African immigrants had lower AIRg and DI values than African Americans, despite similar SI values. This suggests that beta-cell failure, rather than insulin resistance, is contributing to the high rate of diabetes and prediabetes observed in the African immigrants. Consistent with our finding, beta-cell failure has been implicated as a key cause of T2DM in Africans living in France. 22
Our observation that African men had worse cardiometabolic health than African American men conflicts with the concept of the healthy immigrant effect. The healthy immigrant effect suggests that African immigrants are healthier than African Americans and that this health differential persists for decades. 2,23,24 However, as Africa is becoming urbanized and Africans exercise less and consume more refined and processed food, it can no longer be assumed that Africans are arriving in the United States as healthy as they were in the past. To recognize this change, two techniques commonly used to gauge immigrant health need critical reassessment: The first is self-reported health and the second is the use of BMI as a marker of overall cardiometabolic health.
African immigrant health is most often determined from datasets that rely on self-reported health. The most frequently used surveys include data from the United States Census Bureau, the National Health Interview Surveys, the Healthy Directions-Health Centers Study, and the National Survey of American Life. 2,3,23 –27 For example, Hamilton and Hummer evaluated data from the United States Census Bureau collected between 1996 and 2010 in 67,941 African Americans and 9014 black immigrants. 2 Their dataset contained detailed self-reported information about income, labor, family structure, and country of origin, but only one health question. Respondents were asked to rate their current health status on a five-point scale as excellent, very good, good, fair, or poor. The authors converted this health rating into a binary variable: “fair/poor health” received a “1”, and “other” received a “0”. On the basis of this type of analysis, the authors concluded that African immigrants had an overall better health profile than African Americans. However, it is more accurate to state that immigrants had a better impression of their health status than African Americans. Furthermore, African immigrants were less likely to have health insurance and therefore less likely to visit a primary care provider. Therefore, it is reasonable to assume that immigrants were more likely than African Americans to have undiagnosed disease. In addition, self-reported health is highly influenced by cultural perception of illness. 28 On a cultural basis, immigrants may be less likely than African Americans to self-report poor health status.
The potential for undiagnosed disease to lead to inaccurate health assessment of immigrants is especially pertinent to the African immigrant population. The International Diabetes Federation (IDF) estimates that on the continent of Africa 78% of Africans with diabetes are undiagnosed. Therefore, the African continent has the highest percent of undiagnosed diabetics in the world. 7 Indeed, all of our participants, both African and African American, self-identified as healthy. However, on the basis of metabolic testing after enrollment, Africans were found to have a much higher rate of previously undiagnosed diabetes and prediabetes than African Americans. Therefore, our results support the concept that self-reported health alone is not reflective of actual health status and may make cross-cultural comparisons without clinical validation problematic. 28
The second area of concern is the use of BMI as a measure of cardiometabolic health in African immigrants. There is a general consensus that because BMI is lower in African immigrants than African Americans, African immigrants are healthier. 23,24,27 The inherent error with this approach is that BMI does not provide information on body fat distribution. Central obesity and visceral adiposity in particular are more predictive of cardiometabolic disease than BMI. 16,29 At a lower BMI and WC than African Americans, we found that African immigrants had more VAT as well as a higher rate of diabetes and prediabetes. Furthermore, the WC that predicted insulin resistance was 92 cm in African immigrants and 102 cm in African Americans. Even when African immigrants were examined by region of origin, the WC that predicted insulin resistance in West, Central, and East Africans was less than 102 cm. Therefore, relying on WC thresholds that are used to evaluate African American health may lead to an overly optimistic view of health status of the African immigrants. Our finding that African Americans and African immigrants do not have the same WC threshold of risk may be analogous to the situation with Asian populations, in which WC risk thresholds are different among Asian Indians, Japanese, and Chinese. 30
In the evaluation of cardiometabolic risk, it is important to evaluate lipid status. However, African Americans characteristically have a normal lipid profile, even in the presence of cardiometabolic disease. 31 We note, with interest, that the lipid profile was very good in both groups and in some aspects even better in African immigrants than African Americans.
The main strength of our study is the direct comparison of cardiometabolic risk factors in African immigrants and African Americans by OGTT, FSIGT, and CT scan. We recognize that Osei et al. have performed OGTT and FSIGT in Ghanaian immigrants and African Americans and found no difference in fasting glucose, fasting insulin, insulin resistance, hepatic insulin extraction, or insulin clearance. 32,33 However, the goal of their studies was to compare glucose and insulin physiology in Ghanaian immigrants and African Americans with normal glucose tolerance. 32,33 They did not perform a cardiometabolic risk assessment in the two groups across a spectrum of hyperglycemic states.
Our investigation is the largest comparison of cardiometabolic health in African immigrant and African American men of which we are aware. Nonetheless, we recognize our sample size as a limitation. In addition, we appreciate that our studies in African immigrant men may not be applicable to African immigrant women. However, African immigrant and African American men enrolled in our study appear to be representative of their larger communities. As universally seen in other comparisons of African immigrants and African Americans, the African immigrants in our study were more likely to be married, college educated, nonsmokers, as well as less likely to have health insurance or be physically active. 1,2,27 Additionally, the African American men in our investigation had a prevalence of obesity, prediabetes, and hypertension similar to data reported from large representative cohorts such as NHANES. 34 –36
In the 21st century, cardiometabolic diseases are a major health threat in Africa. 4 –6 Therefore, immigrants are now more likely than in the past to arrive in the United States with established cardiometabolic risk factors. In fact, we have demonstrated that African immigrants were less obese but had more hyperglycemia, hypertension, and visceral adiposity than African Americans. These findings suggest that WC or BMI thresholds that trigger intervention may need to be lower in African immigrants than African Americans. Overall, to achieve cardiometabolic health in African immigrants, health care providers need to recognize that the healthy immigrant effect may no longer be valid.
Footnotes
Acknowledgments
Michelle Y. O'Connor, Caroline K. Thoreson, Madia Ricks, and Anne E. Sumner were supported by the intramural program of NIDDK, National Institutes of Health (NIH). Amber B. Courville, Francine Thomas, and Jack Yao were supported by the NIH Clinical Center.
Author Disclosure Statement
None of the authors have any conflicts of interest to disclose.