
Abstract
Background:
Chronic endotoxemia has been proposed to contribute to obesity-related complications. We aimed to investigate the potential impact of lipopolysaccharide (LPS) and subsequent monocyte activation measured as soluble CD14 (sCD14) on markers of vascular dysfunction in obese subjects undergoing bariatric surgery.
Methods:
This was a prospective study of 49 obese patients and 17 controls, assessed by plasma levels of LPS, sCD14, asymmetric dimethylarginine (ADMA), and symmetric dimethylarginine (SDMA).
Results:
Levels of ADMA were increased in obese subjects compared to controls, but were not significantly reduced after bariatric surgery. In obese subjects at baseline, there was a significant trend to increasing levels of ADMA and SDMA through tertiles of sCD14 and decreasing levels of both markers through tertiles of LPS. In models adjusting for age and gender, sCD14 but not LPS remained independently associated with ADMA and SDMA. For every 10% age- and gender-adjusted increase in sCD14, ADMA increased 0.031 μM (5.6%), whereas SDMA increased 0.039 μM (10.8%).
Conclusions:
Our results suggest that monocyte activation as measured by sCD14 is associated with obesity-related vascular dysfunction, whereas potential upstream triggers including microbial products should be investigated in future studies.
Introduction
O
LPS promotes inflammation mainly by signaling through Toll-like receptor 4 (TLR4) on monocytes and other effector cells, and CD14 plays a central role by transferring LPS to the TLR4 receptor complex. 2 Soluble CD14 (sCD14) is secreted to the circulation mainly by activated monocytes and macrophages upon stimulation with LPS and other microbial products.
Interestingly, chronic LPS infusion is sufficient to initiate obesity and insulin resistance in mice, an effect that is almost abolished in CD14 knockout mice. 1 In human cohorts, elevated LPS levels have been reported in obesity and type 2 diabetes mellitus (T2DM), and we recently showed that plasma LPS correlated significantly with all components of the metabolic syndrome as well as intra-abdominal adipose tissue volumes in bariatric surgery patients. 3
Endothelial dysfunction represents an early stage of atherosclerosis and is accelerated in obesity. In clinical studies, endothelial dysfunction is commonly assessed by flow-mediated dilatation (FMD), which is a direct assessment of the vascular function. Several studies have found impaired FMD in obesity and related co-morbidites, 4 –6 although results on the effect of bariatric surgery on FMD have been conflicting. 7,8
Endothelial cells often express TLR4 as a response to proatherogenic stimuli, and a link between LPS-induced TLR4 activation of endothelial cells and coronary artery disease has been reported. 9 Previously, we have shown that elevated levels of LPS and sCD14 are strong predictors of human immunodeficiency virus (HIV)-associated hypertension, 10 and TLR4 upregulation by angiotensin II may contribute to hypertension and vascular dysfunction through formation of reactive oxygen species (ROS). 11 Furthermore, ROS formation has been shown to play a critical role in vascular TLR expression and vascular dysfunction in high-fat-induced obesity. 12
An indirect way of assessing vascular dysfunction in the absence of FMD is by measuring plasma levels of asymmetric dimethylarginine (ADMA) and its stereoisomer symmetric dimethylarginine (SDMA). ADMA contributes to impaired endothelial function through its inhibitory effect on nitric oxide synthase (NOS). 13 SDMA does not inhibit NOS, but is regarded as a novel marker of vascular dysfunction and renal disease. 14
Recently, we have shown that the plasma level of sCD14, but not LPS, is independently associated with both ADMA and SDMA in HIV-infected patients. 15 However, this relationship has not previously been evaluated in obese subjects. The aim of the present study was to investigate potential associations between LPS and sCD14 and markers of vascular dysfunction in a cohort of obese subjects undergoing bariatric surgery.
Materials and Methods
Patients and controls
The study cohort has previously been described in detail. 3 Forty-nine patients were included, and all of the patients underwent conservative and subsequent surgical treatment at the regional center for treatment of morbid obesity at Nordland Hospital in Norway. In addition, 17 individuals undergoing elective laparoscopic procedures (cholecystectomia) at the same hospital were included as controls at baseline, selected to be of the same race (Caucasians) and from the same geographical area. Out of the 17 controls, eight were normal weight [body mass index (BMI) <25 kg/m2], and nine were overweight (BMI ≥25), with maximum BMI <28. Baseline characteristics of the obese patients and controls are given in Table 1. All patients and controls classified as having hypertension or T2DM received antihypertensive or antidiabetic drugs, respectively. It should be noted that the diagnosis and treatment of hypertension and T2DM was made by the referring primary care physician, before inclusion in our study.
Categorical data are reported as n (percentages) and continuous data as mean [standard deviation (SD)], or as median and 25th and 75th percentile, as appropriate.
BMI, body mass index; HbA1c, glycated hemoglobin; ADMA, asymmetric dimethylarginine; SDMA, symmetric dimethylarginine.
Two surgical methods were used for the patients undergoing bariatric surgery: Laparoscopic Roux-en-Y Gastric bypass was performed by a standardized procedure and used for patients with a BMI <50 kg/m2. This procedure included a small ventricular pouch of 30 mL and a bileopancreatic limb of 50 cm, with an alimentary limb of 100 cm. For patients with a BMI >50 kg/m2, duodenal switch was performed by a standardized procedure that included a gastric sleeve using a 32 French probe to measure the diameter, an alimentary limb of 150 cm, and a common channel of 100 cm. All operations were performed by two experienced bariatric surgeons. Intervention effects on metabolic components, 16 as well as LPS and sCD14, 3 have been published elsewhere. The effect of bariatric surgery on ADMA and SDMA levels are presented here.
Patients with an abdominal diameter >50 cm were excluded from attending a computed tomography (CT) scan due to the diameter of the CT scanner. Hence, 24 obese patients and 17 controls were evaluated with CT scan and included in the correlation analyses at baseline (flow chart, Fig. 1). Those attending CT scan had a lower BMI than those excluded from this evaluation (41.8±3.4 vs. 48.3±8.6 kg/m2, P=0.001), without differing in the other demographic, clinical, or biochemical characteristics, with the possible exception of lower ADMA levels (0.52±0.14 vs. 0.57±0.07 μM, P=0.145). The study was performed in accordance with the Helsinki Declaration, 3 and written, informed consent was obtained from all patients.

Flow chart. Patients with abdominal diameter >50 cm were excluded from attending a computed tomography (CT) scan due to the diameter of the CT scanner.
Plasma levels of LPS and sCD14 and endovascular function
Fasting blood samples were collected with standard venipuncture. LPS, sCD14, ADMA, and SDMA were determined in pyrogen-free EDTA plasma tubes, which were snap frozen and stored at −70°C until analysis in batch. LPS activity was analyzed by a Limulus Amebocyte Lysate colorimetric assay (Lonza, Walkersville, MD), using pyrogen-free Nunc® tubes, whereas sCD14 was analyzed using an enzyme-linked immunosorbent assay (ELISA) according to the manufacturer's instructions (R&D, Minneapolis, MN). In our hands, the interassay coefficient of variation (CV) was <10% for both LPS and sCD14. 3
ADMA and SDMA were measured by high-performance liquid chromatography and precolumn derivatization with o-phthaldialdehyde (Sigma Chemicals Co., St. Louis, MO) as described in details elsewhere with minor modifications. 17 The interassay CVs were <5% for both analyses.
Quantification of adipose tissue volumes
Preoperative CT scans were performed on a Siemens Sensation 4 sliced CT scanner (Siemens AG, DE), using validated methods. 18 The scans were performed at 120 kV and 250 mA, and the subjects were examined in a supine position with their arms stretched above their head. To minimize the amount of radiation, a CT volume scan with a slice thickness of 10 mm was performed at only one site—in women 5 cm above the L4/L5 level and in men 10 cm above the L4/L5 level. The subcutaneous and intra-abdominal adipose tissue compartments were traced manually, and the inner abdominal muscular wall separated the compartments. All CT scans were examined by the same radiologist at the end of the study. 3
Statistical analyses
Differences between groups at baseline were evaluated with independent samples t-test or with the Mann–Whitney U-test for continuous data, and with the chi-squared or Fisher exact test for categorical data, as appropriate. Differences from baseline to 1 year after bariatric surgery were evaluated with the paired samples t-test, and data were given as mean±standard deviation (SD). Correlation analyses were performed using the Spearman rho due to skewed distribution of LPS values. Analysis of variance (ANOVA) was used for trend analyses through tertiles of CD14 and LPS. Given the small sample size, multivariate linear regression models included only age and gender as covariates. Due to a large range of CD14 values (1070 ng/mL) and a narrow range of ADMA and SDMA in obese subjects, CD14 was entered into the model as+10% change (+107 ng/mL), to obtain beta coefficients comparable to the published literature. Entering CD14 as+1 ng/mL change resulted in similar P values but lower beta coefficients (data not shown).
Models including a third covariate were created, adding variables one at a time on the basis of significant associations in the univariate analyses or potential impact on vascular dysfunction. Triglycerides (TGs) were log-transformed before being entered into the model; BMI and age were normally distributed and entered as continuous variables, whereas gender, smoking, hypertension, and T2DM were entered as dichotomous variables. In models investigating correlates of LPS, LPS was log-transformed. Statistical assumptions for the use of the linear regression model were satisfied. A two-tailed significance level of 0.05 was used. The statistical analyses were performed with SPSS software, version 19.0 (SPSS Inc, Chicago, IL).
Results
Increased levels of ADMA in obese subjects at baseline
As shown in Table 1, ADMA levels were significantly elevated in obese subjects compared to controls, whereas the difference in SDMA levels was borderline significant. Because endothelial dysfunction is impaired in subjects with T2DM, we also restricted comparisons to subjects without diabetes. In this subgroup, we observed a similar difference between obese subjects and controls for levels of ADMA (0.57±0.10 vs. 0.48±0.07 μM, P=0.001) and SDMA (0.37±0.11 vs. 0.32±0.06 μM, P=0.056).
No effect of bariatric surgery on markers of vascular dysfunction
One year after bariatric surgery, no significant changes from baseline were observed for ADMA (mean change 0.02±0.13 μM, P=0.475) or SDMA (−0.02±0.09 μM, P=0.166). As previously reported, plasma levels of LPS and sCD14 were elevated in the obese subjects compared to controls, whereas levels of LPS but not sCD14 were reduced after bariatric surgery. 3
Disparate associations between sCD14 and LPS and markers of vascular dysfunction
In obese subjects at baseline, there was a positive correlation between sCD14 and both ADMA (r=0.49, P=0.025) and SDMA (r=0.60, P=0.004). Furthermore, there was a significant increase in levels of ADMA (P=0.008) and SDMA (P=0.007) through tertiles of sCD14 (Fig. 2).
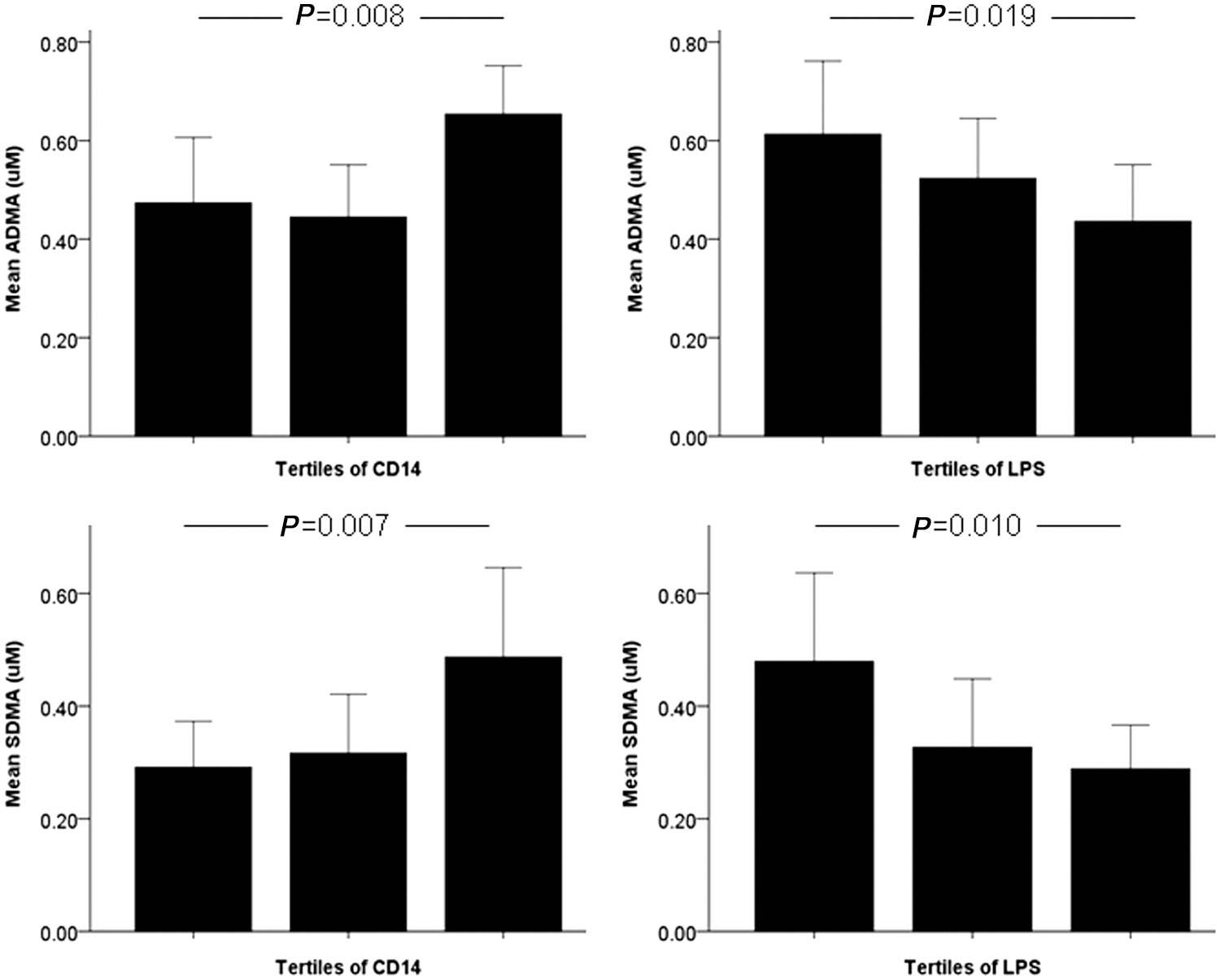
CD14 and lipopolysaccharide (LPS) are disparately associated with markers of vascular dysfunction in bariatric surgery patients at baseline. Mean [standard deviation (SD)] values of asymmetric dimethylarginine (ADMA) and symmetric dimethylarginine (SDMA) through tertiles of CD14 and LPS. P values refer to trend analyses [analysis of variance (ANOVA)].
Conversely, plasma LPS was negatively correlated with both ADMA (r=−0.47, P=0.034) and SDMA (r=−0.54, P=0.012), and there was a significant decrease in levels of ADMA (P=0.019) and SDMA (P=0.010) through tertiles of LPS (Fig. 2). Correspondingly, there was a negative correlation between LPS and sCD14 levels in the obese subjects (r=−0.50, P<0.001).
sCD14 is associated with ADMA and SDMA in obese subjects
ADMA levels were significantly correlated with BMI (r=0.31, P=0.036), but not with the other components of the metabolic syndrome, including waist circumference and intra-abdominal or subcutaneous adipose tissue compartments. In multivariate linear regression models, sCD14 but not LPS remained independently associated with ADMA and SDMA after adjustment for age and gender. For every 10% age- and gender-adjusted increase in sCD14, ADMA increased 0.031 μM (5.6%), whereas SDMA increased 0.039 μM (10.8%). These associations remained significant and almost unchanged when a third covariate was added to the multivariate linear regression model one at a time, i.e., BMI, TGs, diabetes, smoking, and hypertension (Table 2). Adding intra-abdominal or subcutaneous adipose tissue compartments to the model did not change these associations (data not shown). As depicted in Fig. 2, the influence of CD14 on ADMA levels seems to be particularly high in the upper tertile of CD14, suggesting a potential threshold effect rather than a dose–response relationship. Hence, entering CD14 as tertiles in the multivariate model resulted in similar P values but considerably higher beta coefficients (data not shown). However, as we could not identify any clear cutoff values of sCD14, we have chosen to present the main result in a linear regression model.
Beta-coefficients represent changes in ADMA and SDMA for each 10% increase (+107 units) in CD14. Data are adjusted for age and gender alone, or in combination with a third covariate, added to the model one at the time. Triglycerides were log-transformed before being entered into the model.
ADMA, asymmetric dimethylarginine; SDMA, symmetric dimethylarginine; CI, confidence interval; BMI, body mass index.
Discussion
The main finding in this study was an association between sCD14 and both ADMA and SDMA, indicative of a potential role of monocyte activation in obesity-related vascular dysfunction. We found that an age- and gender-adjusted increase in CD14 of 10% was associated with an increase of 0.031 μM in ADMA levels. For comparison, in the Framingham offspring study, a 0.13 μM increase in ADMA was associated with 21% increased risk of death. 19
ADMA inhibits NOS, thereby decreasing the bioavailability of nitric oxide (NO) in the endothelium. ADMA is degraded by dimethylarginine dimethylaminohydrolase (DDAH), and it has been suggested that several proatherogenic factors may lead to inactivation of DDAH, thereby increasing the level of circulating ADMA. Although SDMA has been associated with endovascular dysfunction, hypertension, and renal impairment, the mechanism seems to be different, because SDMA does not inhibit NOS, but has been shown to have proinflammatory effects by enhancing ROS and activating leukocytes. 20,21
We and others have previously shown that increased ADMA levels are associated with several traditional risk factors, including obesity. 13,22 The novel finding of this study is the potential role of monocyte activation in this process, and our findings fit well with a previous report of association between sCD14 and aortic stiffness in a population-based study. 23 Furthermore, we have recently reported similar findings in an HIV-infected population, with sCD14, but not LPS levels, being independently associated with ADMA and SDMA. 15 Moreover, although levels of LPS-binding protein (LBP) and sCD14 are elevated in the metabolic syndrome, only sCD14 is associated with monocyte TLR4 protein and activity, and addition of sCD14 to LPS-primed human aortic endothelial cells resulted in a greater TLR4 abundance as compared to addition of LBP. 24
Concentrations of CD14 have been reported to increase after LPS exposure in vitro, presumably after shedding from activated monocytes, and systemic levels of sCD14 have therefore been assumed to reflect the amount of LPS-associated cell activation. 25 However, the circumstances might be different in conditions with prolonged low-grade endotoxemia, and a previous study reported opposing associations between sCD14 and endothelial dysfunction in diabetic compared to nondiabetic subjects. 25 The biological effect of LPS itself may also differ in acute and chronic conditions, in part by immune cells becoming refractory to repeated bouts of low-grade endotoxemia. 26
However, the negative associations between plasma LPS and markers of vascular dysfunction in the present study were unexpected and should be interpreted with caution, both due to the relatively small study population and to the fact that this association was no longer significant in multivariate analyses. Of note, CD14 might be shed to the circulation by several stimuli beyond LPS, including microbial products such as peptidoglycan and CpG DNA, and may even act as a cofactor for several TLRs, in addition to TLR4. 27 Thus, different upstream triggers might be involved in this cohort of bariatric surgery patients. Relevant to this, we have recently shown that morbidly obese patients have elevated levels of complement factors C3 and C4, central components of the innate immune system, and that bariatric surgery and subsequent weight loss can normalize such elevated levels. 28
Moreover, the association between vascular dysfunction and monocyte activation could work in both directions, because ADMA has been shown to induce adhesion 29 and activation of monocytes. 30 Hence, measurement of other markers of monocyte activation (such as sCD163), microbial products (e.g., 16S DNA, peptidoglycan, flagellin antibodies), as well as gut microbiota composition could add valuable information in future studies. LBP could also add information in future studies. However, this is an indirect measurement of endotoxin activity that cannot replace direct LPS measurements, which in our hands have shown low variability in several studies.
There are some limitations that need to be acknowledged in the interpretation of the results. First, the lack of a direct measure of endothelial dysfunction such as FMD is of particular relevance in our cohort of obese individuals given recent evidence that proinflammatory adipokines may contribute to vascular dysfunction independently of NO availability. 31 Hence, this should be regarded as an exploratory study that should be followed by larger studies including FMD or other direct measurement of vascular dysfunction. However, we have investigated both a NO-dependent marker (ADMA) and a NO-independent marker (SDMA), and it is reassuring that sCD14 is independently associated with both markers.
Another limitation is the small sample size, increasing the probability of type II statistical errors. Hence, the lack of effect of bariatric surgery on levels of ADMA and SDMA should be interpreted with caution, in light of other published reports, 32 and 1-year follow-up may not be sufficient to assess long-term vascular effects of bariatric surgery. 7,8 Finally, there are many unknown and unmeasured factors, including socioeconomic status, lifestyle factors, dietary intake, detailed registration of medication, and gut microbiota composition, that could have potentially confounded the results—both the negative results for LPS and the positive results for sCD14.
In conclusion, monocyte activation as measured by sCD14 was closely associated with markers of vascular dysfunction in bariatric surgery patients. Our results support a role for monocyte activation in development of vascular dysfunction and subsequent increased cardiovascular risk in obesity, but potential upstream triggers should be investigated in future studies.
Footnotes
Author Disclosure Statement
No competing financial interests exist.