
Abstract
Metabolic syndrome is closely associated with morbid obesity and leads to increased risk of cardiovascular diseases and related mortality. Bariatric surgery is considered an effective option for the management of this condition. We searched MEDLINE, Current Contents, and the Cochrane Library for papers published on bariatric surgery outcomes in English from January 1, 1990, to April 20, 2014. Bariatric surgery can significantly reduce body weight, resolve or cure many of the symptoms of metabolic syndrome, including type 2 diabetes, hypertension, hyperlipidemia, and improve long-term survival. Surgery, in addition to existing therapy, could therefore be considered as an optimal treatment for patients with metabolic syndrome and morbid obesity.
Introduction
M
Bariatric surgery can significantly reduce body weight, resolve obesity-related co-morbidities, and increase life expectancy. This article reviews the common types of surgical bariatric procedures and their impact on components of metabolic syndrome, including obesity, T2DM, dyslipidemia, and hypertension.
Etiologies and Prevalence
The factors that are most commonly blamed in the development of metabolic syndrome are insulin resistance and obesity. Insulin resistance plays a critical role in the pathologies constituting metabolic syndrome, such as dyslipidemia, hyperglycemia, and hypertension. The pathology is at the postreceptor level and it develops as a result of disorders in the intracellular pathways after insulin binding to its receptor. 4,5 Obesity is another clear risk factor for the development of metabolic syndrome. The prevalence of metabolic syndrome appears to be increasing along with a parallel rise in the prevalence of obesity, and the likelihood of a further increase in metabolic syndrome can be anticipated because of projections of a greater prevalence of obesity in the future. 6 National Health and Nutrition Examination Survey (NHANES) data reveal metabolic syndrome in approximately 5% of people with normal body weight, 22% of people who are overweight, and 60% of people with obesity by body mass index (BMI) criteria. 7 Other risk factors for metabolic syndrome appear to be genetic and environmental and include family history, sedentary lifestyle, smoking, high carbohydrate diet, ethnicity, and older age, which bring about insulin resistance, hyperinsulinemia, endothelial dysfunction, and inflammation. There are also abnormalities of adipocyte function, accompanied by inappropriate secretion of multiple hormones and cytokines, along with abnormal accumulation of fat in tissues such as muscle and liver. 8
The worldwide prevalence of metabolic syndrome ranges from <10% to as much as 84%, depending on the region, urban or rural environment, composition (sex, age, race, and ethnicity) of the population studied, and the definition of the syndrome used. 9 In general, the International Diabetes Federation (IDF) estimates that one-quarter of the world's adult population has metabolic syndrome. 10 Higher socioeconomic status, sedentary lifestyle, and high BMI are significantly associated with metabolic syndrome, and differences in genetic background, diet, levels of physical activity, smoking, family history of diabetes, and education all influence the prevalence. 11 In the United States, prevalence increased from 6.7% among participants aged 20–29 years to 43.5% and 42.0% for participants aged 60–69 years and aged >70 years, respectively. 12 In Asia, the total prevalence of metabolic syndrome varies from 7.8% to 14.9% on the basis of different criteria in different studies in Japan. 13 In China, the prevalence of metabolic syndrome was 9.8% in men and 17.8% in women, corresponding to the prevalence of overweight, which was 26.9% in men and 31.1% in women. 14
Evolution of Definition
The concept of metabolic syndrome has existed for at least 80 years, but it was more comprehensively described in 1988 by Reaven as “a cluster of risk factors for diabetes and cardiovascular disease”; he named it “Syndrome X.” His main contribution was introduction of the concept of insulin resistance. 15 Since that time, to help define metabolic syndrome for clinical and research purposes, diagnostic criteria have been proposed by different national and international health organizations (Table 1). Although the actual definitions differ in their criteria and threshold values, most agree on the essential components—obesity, dyslipidemia, hypertension, and glucose intolerance.
Insulin sensitivity measured under hyperinsulinemic euglycemic conditions, glucose uptake below lowest quartile for background population under investigation.
In 2003, the American Diabetes Association changed the criteria for IFG tolerance from>110 mg/dL to>100 mg/dL.
Includes family history of type 2 diabetes mellitus, polycystic ovary syndrome, sedentary lifestyle, advancing age, and ethnic groups susceptible to type 2 diabetes mellitus.
WHO, World Health Organization; EGIR, European Group for the Study of Insulin Resistance; ARTP III, Adult Treatment Panel III; AACE. American Association of Clinical Endocrinologists; IDF, International Diabetes Federation; AHA/NHLBI, American Heart Association/National Heart, Blood, and Lung Institute; IGT, impaired glucose tolerance; IFG, impaired fasting glucose; T2DM, type 2 diabetes mellitus; BMI, body mass index; WC, waist circumference; Rx, receiving treatment; HDL-C, high-density lipoprotein cholesterol; TGs, triglycerides.
The first attempt was made by a World Health Organization (WHO) diabetes group in 1998, which included obesity based on BMI, insulin resistance, microalbuminuria, and hypertension as additional risk factors; they identified insulin resistance as the dominant cause of metabolic syndrome, and clinical indicators of insulin resistance were required for diagnosis. 15 In response, the European Group for the study of Insulin Resistance (EGIR) proposed a modification of the WHO definition in 1999. 16 They excluded diabetes, on the basis of the presumption that insulin resistance preceded the development of diabetes, and central obesity was classified by waist circumference (WC). In 2001, the National Cholesterol Education Program Adult Treatment Panel (NCEP ATP) released its definition. 17 Abdominal obesity was integrated as a key component of metabolic syndrome, and insulin resistance was excluded, because its measurement was difficult and not standardized. In 2003, the American Association of Clinical Endocrinologists (AACE) offered its views and definition of the syndrome, which reintroduced the concept of insulin resistance as the underlying means of linking the metabolic abnormalities. 18
In 2005, recognizing the difficulties in unified criteria for metabolic syndrome, the IDF dropped the WHO requirement for insulin resistance but made abdominal obesity necessary as one of five factors required in the diagnosis, with a particular emphasis on waist measurement, with geographic and ethnic variation as a simple screening tool. 10 The American Heart Association and the National Heart, Lung, and Blood Institute (AHA/NHLBI) recognized the clinical simplicity of the Adult Treatment Panel III (ATP III) definition and accepted the limitations of the remaining questions pertaining to underlying pathophysiological mechanisms, but they reduced the threshold for impaired fasting glucose (IFG) to 5.6 mmol/L, which was outlined by the American Diabetes Association (ADA), and also recognized ethnicity-dependent measurement of WC. This definition and treatment guidelines included patients with established CVD or diabetes if they fulfilled the appropriate criteria. 19
The proliferation of definitions suggested that a single unifying definition was desirable. A global “harmonized” definition has now been proposed by IDF and AHA/NHLBI. Both sides agreed that abdominal obesity should not be a prerequisite for diagnosis but that it is one of five criteria, so that the presence of any three of five risk factors, including WC, triglycerides (TGs), high-density lipoprotein cholesterol (HDL-C), blood pressure, and fasting glucose, constitutes a diagnosis of metabolic syndrome (Table 1). 2
Surgical Treatment for Metabolic Syndrome
A multidisciplinary approach is required for clinical management of patients with metabolic syndrome, which includes lifestyle changes as well as pharmacological and surgical approaches, to reduce both short-term and lifetime risk of subsequent diseases. Major changes in lifestyle that are recommended for individuals with metabolic syndrome include weight loss of at least 5–10% of initial body weight, reduction in the dietary contribution of total and saturated fat, increased physical activity, and long-term weight control. Pharmacological treatment should be considered for those whose risk factors are not adequately reduced with the preventive measures and lifestyle changes. Surgery is recommended for individuals who fail to respond to lifestyle change or medications, or are extremely obese (BMI >40 kg/m2), or if they have a BMI >35–40 kg/m2 and one or more co-morbid conditions. 1,20
Losing weight and long-term maintenance of the weight loss are primary targets to beneficially reverse all of the components of metabolic syndrome. 5,21 Bariatric surgery is an effective, durable, and safe treatment for obesity and associated co-morbidities. It is increasingly appreciated that the effects of bariatric surgery, in particular with regard to co-morbidities, are due not only to forced caloric restriction but also more sophisticated neurohormonal mechanisms. In essence, bariatric surgery is not only a weight-loss surgery but also metabolic surgery. 22 Long-term total mortality after bariatric surgery has been reduced significantly, particularly deaths from diabetes, heart disease, and cancer. Cause-specific mortality in the surgery group decreased by 56% for coronary artery disease and by 92% for diabetes. 23 In the Swedish Obese Subjects (SOS) study, with an average follow-up of 10.9 years, mortality significantly decreased in patients who had undergone operations compared to those treated conventionally; the unadjusted hazard ratio in the surgery group was 0.76 compared with the control. 24
In 1991, The National Institutes of Health Consensus Development Conference on Gastrointestinal Surgery for severe obesity recommended that surgical intervention be considered for patients with a BMI>35 kg/m2 who have co-morbid conditions of obesity or patients with a BMI>40 kg/m2 without co-morbid conditions. 25 In light of the mounting clinical evidence that demonstrates clear benefit in the use of bariatric surgery for T2DM, several clinical guidelines and statements have been published on this topic. These include recommendations by the Diabetes Surgery Summit of 2007 (DSS 2007), IDF, ADA, and the AACE in conjunction with the American Society for Metabolic and Bariatric Surgery (ASMBS) and The Obesity Society (TOS). 26 –29 Among these organizations, there is general agreement regarding the potential use of bariatric surgery as a treatment for T2DM in obese individuals with BMI of 35 kg/m2 or greater. The IDF, AACE, ASBMS, and TOS go a further step to propose that diabetic individuals with a BMI between 30 and 35 kg/m2 may be considered for bariatric surgery in certain circumstances under the direction of diabetic specialist. All of these organizations insist upon the careful selection of obese diabetic patients that stand to the most benefit from bariatric surgical procedures with clear discussion of the risks and surgical options. 30
Common Types of Bariatric Surgery
Bariatric/metabolic surgeries are among the most commonly performed gastrointestinal procedures in operating rooms today. Procedures can be divided into three broad categories on the basis of their mechanism of action. 31,32
1. Restrictive procedures aim to restrict the amount of eaten food by surgically reducing the size of the stomach. The restrictive procedures most commonly performed are vertical banded gastroplasty (VBG), laparoscopic adjustable gastric banding (LAGB), and sleeve gastrectomy (SG).
2. Malabsorptive procedures are less popular than restrictive procedures and are more technically demanding; patients often develop nutritional deficiencies. Procedures aim to bypass a segment of the small bowel so that less food is absorbed, such as jejunoileal bypass, distal gastric bypass, biliopancreatic diversion (BPD), and biliopancreatic diversion with duodenal pouch (BPD-DS).
3. The mixed procedure—the Roux-en-Y gastric bypass (RYGB)—aims to restrict food intake by creating a small gastric pouch and limits absorption by bypassing the proximal small bowel. It leaves 95% of the small bowel intact and so avoids many of the unwanted malabsorptive side effects, such as diarrhea and nutritional deficiencies.
Bariatric surgery has evolved through numerous modifications to achieve optimal weight loss while minimizing surgical morbidity and nutritional deficiency, and a few safe operations have emerged. Although many surgical operations for weight loss currently exist, some have been relegated to history. Additionally, the types of bariatric operations are in continuous flux. A survey conducted by the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO) shows that the global total number of bariatric procedures in 2011 was 340,768. The most commonly performed procedures were RYGB (46.6%), sleeve gastrectomy (27.8%), adjustable gastric banding (17.8%), and BPD-DS (2.2%). 33 Although BPD and BPD-DS less commonly performed, they are often considered in extremely obese individuals. 34
LAGB was the first bariatric procedure to be performed by laparoscopically. Introduction of LAGB into clinical practice was an immediate success in Europe and Australia. A silicone prosthesis is fitted around the stomach just below the gastroesophageal junction, creating a 15- to 20-mL pouch; moreover, the diameter of the inflating band can be adjusted to the individual needs of the patient via a subcutaneous port (Fig. 1a). It does not involve either rerouting of food through the upper gastrointestinal tract or exclusion of intestinal segments. The weight loss in the short and long term is due to the food intake restriction and early satiety. 32
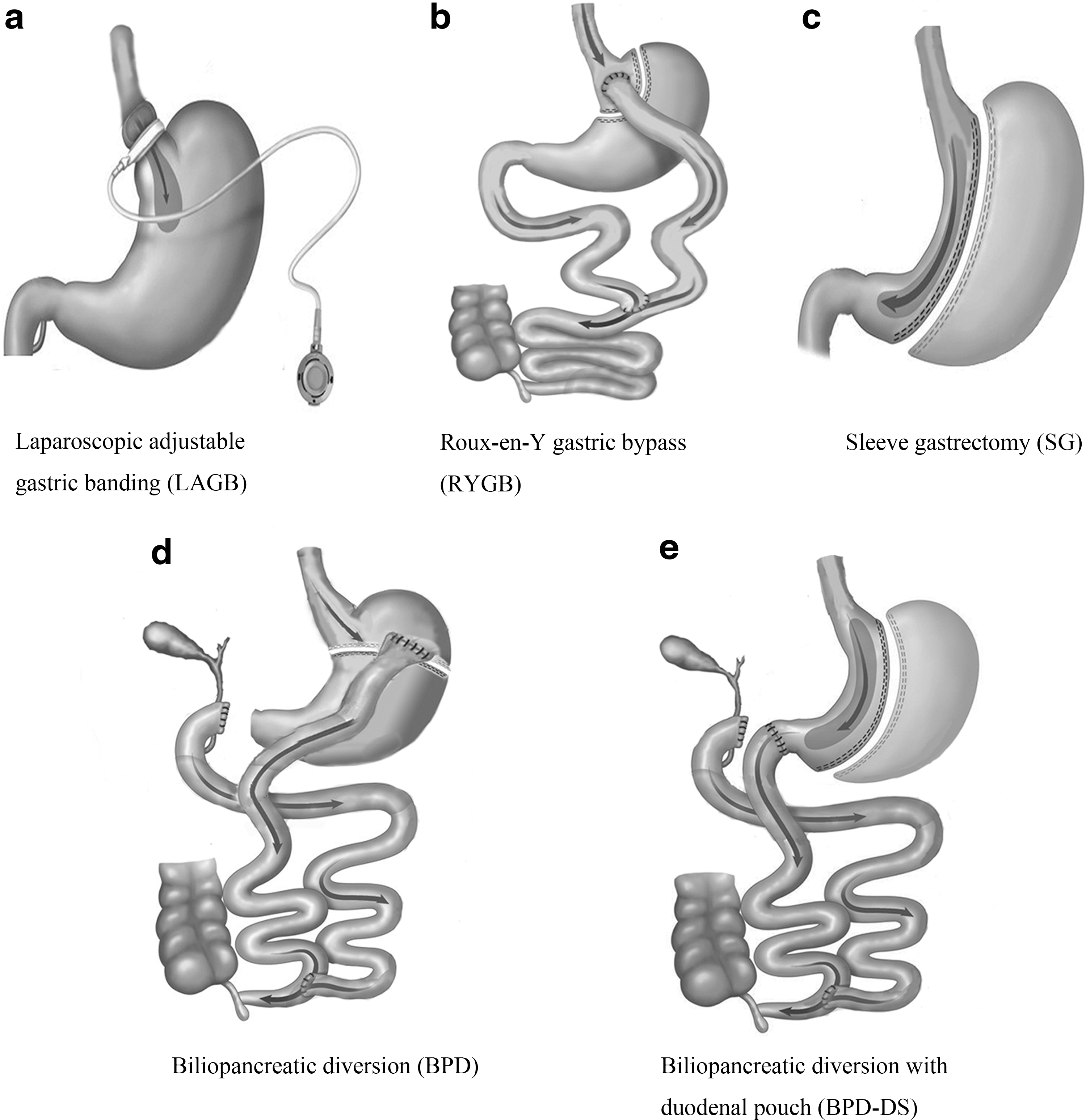
Common types of bariatric surgery.
RYGB was the most largely performed bariatric/metabolic procedure, and now most RYGB is performed laparoscopically. The standard gastric bypass procedure consists of: (1) Creation of a small (15–30 mL) isolated gastric pouch using an endoscopic surgical stapler; (2) dividing the small bowel 30–40 cm from the ligament of Trietz to create the Roux and biliopancreatic limb, (3) reconstruction of the gastrointestinal tract by connecting the distal end of the divided bowel (Roux limb) to the pouch, creating a gastrojejunostomy, and (4) anastomosing the biliopancreatic limb about 100–150 cm distal to the gastrojejunostomy (Fig. 1b). During a meal, the gastric pouch quickly fills to create a sensation of satiety. Food in the gastric pouch enters the jejunum via the Roux limb, and the length of the biliopancreatic limb, which is inversely related to the length of the Roux-Y-limb, determines the degree of malabsorption. 21
SG was the most recently introduced bariatric surgery technique and has already gained a broad consensus on its efficacy and safety. In fact, SG is a technically simple procedure with a low complication rate and negligible long-term nutritional deficiencies. A partial gastrectomy, which removes the greater curve of the stomach, is done leaving a 100- to 150-mL tubular gastric conduit based on the lesser curvature of the stomach (Fig. 1c). It can be performed alone or as part of a staged procedure in which BPD-DS is performed after initial weight loss has occurred. 31
Regarding BPD/BPD-DS, Scopinaro first performed the BPD in 1976. This operation combines removal of two-thirds of the stomach (distal gastrectomy) with a long intestinal bypass–biliopancreatic limb and alimentary limb anastomosis 50 cm from the ileocecal junction, and includes cholecystectomy and liver biopsy (Fig. 1d). This operation induces controlled malabsorption without potential side effects caused by bacterial overgrowth and indiscriminate malabsorption associated with the jejunoileal bypass, which is now completely abandoned. Hess modified the procedure with a variant that he called the “duodenal switch” in 1986, and Gagner first performed it laparoscopically in 1999. Instead of performing a distal gastrectomy, a “sleeve gastrectomy” along the vertical axis of the stomach (volume of remnant 70–150 mL) was proposed; it preserves the pylorus and initial segment of the duodenum, which is then anastomosed to a segment of the ileum, similar to the BPD, to create the alimentary segment (common channel 100 cm) (Fig. 1e). Preservation of the pyloric sphincter is designed to be more physiological. The SG decreases the volume of the stomach and also decreases the parietal cell mass, with the intent of decreasing the incidence of ulcers at the duodeno-ileal anastomosis. These procedures produce selective malabsorption by limiting food digestion and absorption to a short, common ileal segment. 34
With rapid developments in laparoscopic instrumentation in the early 1990s, a series of successful laparoscopic bariatric procedure were first performed in 1993, including laparoscopic gastric band, VBG, and RYGB. 35 Bariatric surgery is now largely performed laparoscopically, except in cases of technical reasons. Rates of conversion to open procedures are in the range of 0–5.7%, with the highest rates seen in the most complex malabsorptive procedures or revisional surgeries. 36 The single-access techniques have been reported for different kinds of laparoscopic bariatric operations. Early case studies suggest that despite longer operative times, single-access bariatric surgery is more acceptable to the patient with equivalent weight loss and similar complication rates. 37,38 With development of the da Vinci platform by Intuitive Surgical, the use of robotics in bariatric surgery has been evolving as an option to standard laparoscopic operations, and the number of procedures has been growing over the last decade. 39 Although there is a lack of high-level evidence, primary results from robotic-assisted bariatric surgery are comparable with traditional laparoscopic surgery. Studies suggest that the technical advantages of robotic surgery result in clinical value for procedures of advanced complexity, such as RYGB and revision bariatric surgery. 40
Effect of Bariatric Surgery on Metabolic Syndrome
Efficacy
Bariatric surgery has been shown in multiple studies to provide substantial durable weight loss and improve or cure many of the symptoms of metabolic syndrome, including T2DM, hypertension, sleep apnea, and hyperlipidemia. It was documented that metabolic syndrome resolution rates were high after bariatric surgery, ranging from 66% to 84%. 41,42 In a retrospective study carried out by the Mayo Clinic, 180 patients undergoing RYGB and 157 patients were enrolled in a weight reduction program. After a mean follow-up of 3.4 years, all components of metabolic syndrome improved in the surgical group and the number of patients with metabolic syndrome decreased by 58%, whereas in the nonsurgical group metabolic syndrome prevalence decreased by 10%. The relative risk reduction for metabolic syndrome was 0.59 with bariatric surgery. 41 Nugent et al. showed that regardless of the type of laparoscopic bariatric surgery, significant improvements were noted in metabolic syndrome, and patients meeting ATP III criteria decreased form 39.2% to 10% at the follow-up, accompanied with improvement of all components of metabolic syndrome. 43 Ikramuddin et al. conducted a 12-month, two-group unblinded randomized trial, which set a composite goal of glycated hemoglobin (HbA1c) less than 7.0%, low-density lipoprotein cholesterol less than 100 mg/dL, and systolic blood pressure less than 130 mmHg. All 120 patients received the intensive lifestyle–medical management protocol. Sixty patients were randomly assigned to undergo RYGB; 28 (49%) participants in the surgical group and 11 (19%) in the lifestyle–medical management group achieved the primary end points. 44 In a meta-analysis with 6587 patients, the investigators concluded that 12–24 months after surgery, a BMI reduction of 5 corresponded to a T2DM reduction of 33%, hypertension reduction of 27%, and hyperlipidemia reduction of 20%. 45 Medication use for T2DM, hypertension, and dyslipidemia also declined significantly following surgery. The clinical and economic benefits of reduced medication requirements should be considered when making decisions about the effects of bariatric surgery. 46
The predictors for resolution of metabolic syndrome after surgery are controversial. Most studies have affirmed that the resolution of metabolic syndrome depends more on the amount of excess weight lost (EWL) than on other parameters, 41 but there are other factors that affected the remission of metabolic syndrome. In a study including 4088 patients, 57% were diagnosed as having metabolic syndrome before bariatric operations; metabolic syndrome was resolved in 46% of these patients after surgery. Laparoscopic RYGB procedures, younger age, race/ethnicity, and lower BMI at the time of surgery were all significant predictors of metabolic syndrome resolution. 47 Faria et al. showed in multivariable analysis that the severity of the dysglycemia and the duration of obesity-independent variables related to the remission of metabolic syndrome were independent variables related to the remission of metabolic syndrome, the severity of the dysglycemia, and the duration of obesity. 42
Some studies compared the effect of different bariatric techniques on metabolic syndrome (Table 2). Gracia-Solanas et al. compared the remission rate of metabolic syndrome in patients who received BPD, modified BPD, VBG, or laparoscopic RYGB and concluded than the best technique to resolve metabolic syndrome was the modified BPD with 7 years follow-up; however, it should only be considered in superobese patients due to its high morbidity. 48 Pontiroli et al. showed that BPD was more effective than LAGB on BMI, but disappearance of diabetes, hypertension, and metabolic syndrome was similar with BPD and with LAGB, and no new cases observed. 49 Inabnet et al. searched The National Database for the American Society for Metabolic and Bariatric Surgery Centre of Excellence Program for patients with metabolic syndrome that were undergoing bariatric surgery between 2007 and 2010. Among 186,576 research-consented patients, 23,106 (12%) were diagnosed with metabolic syndrome. Of this group, 62% underwent RYGB, 32% had LAGB, 4.5% had SG, and only 1.5% had BPD-DS. BPD-DS had the best effect on the resolution of co-morbidity with the greatest incidence of adverse outcomes. However, the superior safety profile of LAGB banding was at the expense of decreased remission rate of co-morbidity of metabolic syndrome. 50
Long term: Follow-up>2 years.
LAGB, laparoscopic adjustable gastric banding; RYGB, Roux- en-Y gastric bypass; SG, sleeve gastrectomy; BPD, bioliopancreatic diversion; BPD-DS, BPD with duodenal pouch; EWL, excess weight lost; T2DM, type 2 diabetes mellitus
Safety
The data demonstrate that morbidity and mortality associated with bariatric surgery have steadily declined over the past several years. Such improvements have been largely attributed to the widespread use of minimally invasive laparoscopic techniques. Bariatric surgery is safe when performed by skilled surgeons. Patients treated by high-volume surgeons and hospitals had lower 30-day mortality rates and lengths of hospitalization than low- and medium-volume surgeons and hospitals. Mortality is decreased when bariatric surgery is performed by surgeons at hospitals that do more than 100 procedures per year. 51 The 30-day mortality for bariatric surgery ranges from 0.1% to 2% and total late mortality (30 days to 2 years) is approximately 0.35%. 52 –54 In a large meta-analysis by Chang et al., a total of 164 studies (37 randomized clinical trials and 127 observational studies) and 161,756 patients were included. The mortality rates within 30 days and after 30 days were 0.08% and 0.31%, respectively, in randomized clinical trials. The complication rate was 17%, and the reoperation rate was 7%. 55
Complications of bariatric surgery can be defined as early or late, and there is a wide range in the reported complication rates. While infrequent, early complications include anastomotic leak, bowel perforation, hemorrhage, bowel obstruction, anastomotic stricture, and deep venous thrombosis/ pulmonary embolism; band migration, band erosion, and infections of the adjustment port are special complications of LAGB. 56 Vomiting is frequent after bariatric surgery, and examination and appropriate radiological studies should be taken to screen for stricture, stoma stenosis, or herniation. Diarrhea is reported in up to 40% following bariatric surgery; however, the etiology is unclear and treatment is based on appropriate dietary modification and antidiarrheal pharmacotherapy. Deficiencies of iron, vitamin B12, folate, and fat-soluble vitamins can occur after bariatric surgery and are best described in RYGB, BPD, and BPD-DS. The risk of nutritional deficiencies depends on postoperative weight loss, the surgical procedure performed, and patient compliance with follow-up. 34
Body weight
The primary target for treating all components of the metabolic syndrome is weight loss and long-term maintenance. Compared with conventional (nonsurgical) treatment, bariatric surgery effectively induces substantial and persistent weight loss and improvement or resolution of co-morbidities and decreases all causes mortality. 57 The SOS study is the first long-term, prospective, controlled trial to provide information on the effects of bariatric surgery, with which follow-up periods that varied from 10 to 20 years. The mean changes in body weight after 2, 10, 15, and 20 years were 23%, 17%, 16%, and 18% in the surgery group respectively, and 0%, 1%, 1%, and 1% in the control group respectively. 58 In the meta-analysis of Chang et al., BMI loss within 5 years after surgery was persistent in the range of 12–17 for observational studies. For random control studies, the year-1 % EWL was 60%, year-2 %EWL was 71%, and year-3 %EWL was 57%. For observational studies, %EWL values were 46%, 64%, and 67% in the first 3 years. 55
Evidence suggests that different surgical procedures generate different effects on weight loss. RYGB was more effective in weight loss but associated with more complications. LAGB had lower mortality and complication rates, yet the reoperation rate was higher and weight loss was less substantial than RYGB; EWL was 76% with RYGB versus 48% with LAGB in a high-quality study. 55,59 High-quality postoperative care can improve weight loss after LAGB, with results comparable to RYGB. 60 SG appeared to be more effective in weight loss than LAGB and comparable with RYGB at 36 months postoperatively. 61 BPD-DS results in greater weight loss but higher complication rates than RYGB, and weight loss was more sustained after BPD-DS than RYGB in superobese patients; the %EWL was 63% for RYGB and 84% for BPD-DS at 3 years postsurgery. 62,63
Weight loss usually reaches a maximum at 12–18 months postoperatively, and some weight regain is common thereafter. In the SOS study, approximately, 20% of the patients regained all their lost weight within 1–3 years. 64 Freire et al. found that weight regain was seen in 56% of the patients, and weight regain increased significantly with time after surgery, reaching to 14.7% (up to 2 years), 69.7% (from 2 to 5 years), and 84.8% (over 5 years), respectively. 65 The cause of this weight regain remains poorly understood. Psychological factors, including food urges and low levels of well-being, have been implicated but not yet substantiated. 66
Type 2 diabetes mellitus
The impact of surgery on T2DM was noted by Scopinaro as early as 1986 and detailed by Pories and co-workers in 1995. 22 Clinical and laboratory manifestations showed that T2DM resolved or improved in the great majority of patients after bariatric surgery. Bariatric surgery is associated with high rates of remission of T2DM, as demonstrated by Buchwald et al. Their meta-analysis included 135,246 patients in 621 studies; 78.1% of obese diabetics had complete diabetes resolution after a bariatric surgical procedure, and 86.6% showed improvement or resolution of the disease. More specifically, 95.1% of patients had T2DM resolution after BPD-DS, 80.3% after RYGB, 79.7% after VBG, and 56.7% after LAGB. The results are similar with previous reports. 67,68 In a meta-analysis by Inabnet et al., among 23,106 operated obese patients with metabolic syndrome, the 1-year remission rate for diabetes was 28% for LAGB, 52% for sleeve gastrectomy, 62% for RYGB, and 74% for BPD-DS. 50
In recent years, several randomized trials studying the effectiveness of bariatric surgery in T2DM have been reported. Mingrone et al. performed a trial in which obese adults with T2DM greater than 5 years and baseline HbA1c greater than 7% were randomized to intensive medical therapy, RYGB, or conventional BPD. After 2 years follow-up, T2DM remission occurred in no patients in the medical therapy group versus 75% in the RYGB group and 95% in the BPD group. 69 Schauer et al. studied 150 obese diabetic adults given either intensive medical therapy, RYGB, or laparoscopic sleeve gastrectomy (LSG) procedures and followed for 1 year. The primary end point, improvement of HbA1c to less than 6%, was achieved in 12% of the intensive medical therapy group, compared to 42% and 37% of the RYGB and SG groups, respectively. 70 Ikramuddin et al. compared RYGB and intensive medical therapy for control of co-morbid risk factors; control for T2DM, HDL-C, and hypertension was achieved in 28 (49%) participants in the surgical group and 11 (19%) in the medical management group. 44 Consistent with previous observational studies, these randomized studies show that obese patients with uncontrolled T2DM undergoing medical therapy plus bariatric surgery demonstrated superior glycemic control to medical therapy alone in the short term.
The mechanisms of the favorable effects of bariatric procedures on glucose metabolism are not well understood. Interestingly, euglycemia and normal insulin levels occur within days after surgery, long before any significant weight loss. 71 Additional evidence of weight-independent mechanisms of T2DM control derives from observations that bypass surgical procedures induce higher rates of T2DM remission than restrictive forms of bariatric surgery or nonsurgical interventions, despite equivalent weight loss, consistent with the study comparing the results of RYGB and dieting. 72 Consequently, weight loss and T2DM control might be considered two separate outcomes of gastrointestinal surgery, which means that improvement of glycemia is not necessarily secondary to weight loss. Two hypotheses have been proposed to explain the effect on glucose homeostasis following bariatric surgery. The “hindgut hypothesis” holds that diabetes control results from the expedited delivery of nutrient chime to the distal intestine, enhancing a physiologic signal that improves glucose metabolism. The alternative “foregut hypothesis” argues that the exclusion of the duodenum and proximal jejunum from the transit of nutrients may prevent secretion of a putative signal that promotes insulin resistance and T2DM. 73
Theoretically, in metabolic syndrome patients with IFG or impaired glucose tolerance, weight reduction and/or increased physical activity will delay or prevent the onset of T2DM. 74 In the SOS study, compared with nonsurgical interventions, surgery decreased the risk of developing diabetes by more than three times at the 10-year follow-up. 64 At the 15-year follow-up, incidence rates of T2DM were 28.4 and 6.8 cases per 1000 person-years in the control and surgery group, respectively, and bariatric surgery reduced the long-term incidence of T2DM by 78% in obese patients as compared with usual care. 75
Results of recent studies evaluating the role of bariatric surgery for treatment of poorly controlled T2DM patients with BMI<35 kg/m2 showed a 90–100% remission rate after RYGB in those with diabetes duration of less than 5 years. 76,77 Other meta-analysis showed overall 66–84% diabetes patients with BMI<35 kg/m2 had remission with bariatric surgery. 78,79 Although there is wide scientific evidence that bariatric procedures for patients with a BMI of 30–35 kg/m2 and diabetes are associated with greater short-term weight loss and better intermediate glucose outcomes compared with nonsurgical treatments, it is still insufficient to reach conclusions about the appropriate use of bariatric surgery in this population until more data about long-term outcomes and complications of surgery are available. 79
Hypertension
Hypertension is one of the commonest co-morbidities associated with obesity. Obesity and insulin resistance are associated with development of a particularly resistant form of hypertension. The development of resistant hypertension in individuals with metabolic syndrome can be attributed to a number of factors, including proinflammatory cytokines, inappropriate activation of the renin–angiotensin system, vasoconstriction from increased sympathetic nervous system activation, and dysregulation in adipokine production and secretion. Several components of the metabolic syndrome are associated with indirect or direct markers of adrenergic overdrive. 80
Many studies have demonstrated that weight loss lowers blood pressure. In general, a decrease of 1% in body weight leads to a 1 mmHg decrease in systolic blood pressure (SBP) and a 2 mmHg decrease in diastolic blood pressure (DBP). 81 Significant reduction in blood pressure can be seen within 1 month after surgery, and bariatric surgery substantially improved and/or resolved hypertension in most patients (37–53%) or reduced the need for antihypertensive agents (18–36%). 82,83 Buchwald et al. showed a significant reduction in hypertension in the total patient population and across all surgical procedures; 61.7% of hypertensive obese patients showed postoperative resolution, and 78.5% showed resolution or improvement. 68 In a meta-analysis involving 52 studies and 16,867 obese patients, a significant decrease in cardiovascular risk factors, including hypertension, diabetes, and hyperlipidemia, was shown. Mean SBP reduced from 139 to 124 mmHg and DBP from 87 to 77 mmHg. Also a 40% relative risk reduction for 10-year coronary heart disease risk was observed. 84
Reported rates of hypertension resolution differed across studies depending on the procedure. After LAGB, resolution rates of hypertension ranged between 48% and 62.95%; after LSG, between 78% and 93.8%; after RYGB, between 65% and 90.7%; and after BPD-DS in supermorbid obese patients, resolution rates were greater than 68%. 82 Moreover, bariatric surgery effectively resolved hypertension in elderly patients. Although the EWL is less and both T2DM and hypertension are more common in patients aged over 60, there was a trend toward greater improvement of co-morbidities after laparoscopic RYGB compared with younger patients. 85 It is worth noting that patients with vitamin D deficiency, a common nutritional deficiency after RYGB, have significantly lower rates of resolution of hypertension compared with those with adequate vitamin D levels, and vitamin D supplementation resulted in resolution of hypertension. 86,87
Dyslipidemia
Dyslipidemia refers to high levels of low-density lipoprotein (LDL), TGs, and/or total cholesterol, as well as low HDL. Dyslipidemia is present in up to 50% of morbidly obese patients. It is a major modifiable risk factor in the development of atherosclerosis and coronary arterial disease and plays a role in excess morbidity and mortality in morbid obesity. 88
Several studies have reported significant improvement in lipid profiles after surgery. In the meta-analysis of Buchwald et al., hyperlipidemia, hypercholesterolemia, and hypertriglyceridemia were significantly improved across all surgical procedures at the 2-year follow-up. The percentage of patients with improved conditions was typically 70% or higher; the maximum improvements in hyperlipidemia were observed in the BPD-DS (99.1%) and RYGB groups (96.9%). In the total population, total cholesterol, LDL, and TGs decreased by an average of 0.86, 0.76, and 0.90 mmol/L, respectively. 68 The SOS study showed that at 2 and 10 years after bariatric surgery, patients exhibited an improvement in hypertriglyceridemia and HDL levels compared with conventionally treated matched controls. These benefits were less marked at 10 than at 2 years, but remained significant. 64
All different types of bariatric operations have been shown to improve the lipid profile, but the effect of RYGB on dyslipidemia is more impressive compared with LABG or SG. One year after LAGB, mean TGs concentration decreased by 23% and mean total cholesterol decreased by 3.3%. 89 SG results in improvement or resolution rates of more than 70% in most studies. 90,91 At 12 months after RYGB for obese patients with hyperlipidemia, a 66% EWL was associated with a 31% decrease in LDL-C levels, a 39% increase in HDL-C levels and a 63% decrease in TGs; and 82% of patients who were on lipid-lowering medications preoperatively did not require medications. 92 By causing malabsorption of fats to reduce enterocolic circulation and reabsorption of cholesterol, both RYGB and BPD lead to a marked improvement in lipid profile. 93 Taken together, these studies suggest that bariatric surgery not only allows for sustained weight loss, but also is a treatment option for dyslipidemia in morbidly obese individuals.
Conclusion
Metabolic syndrome represents the clustering of several risk factors and is an important predictor of CVD disease and diabetes needing early medical intervention. Obesity is only one symptom of an underlying medical condition rather than a separate disease. Bariatric surgery is significantly effective not only regarding the long-term reduction of body weight, but also for the resolution or improvement of obesity co-morbidities. These beneficial effects not only depend on long-term weight loss, but also on endocrinal changes induced by gastrointestinal surgery. The model of care for metabolic and diabetes surgery should be consistent with the goals of treating metabolic illnesses, and that model should have a broader multidisciplinary structure than that of traditional bariatric surgery to include diabetes expertise and diabetes educators, etc. Surgery as an additional therapy to existing treatment could therefore be considered to be the optimal treatment for patients with metabolic syndrome and morbid obesity. 30
Evidence suggests that the earlier the intervention the better the resolution of co-morbidities. Patients with metabolic syndrome and co-morbidities associated with morbid obesity should be promptly referred for consideration for bariatric surgery earlier in the disease process if they are surgical candidates. 82 The choice of operative technique may influence the outcomes. It seems that the higher the risk of bariatric surgical procedures, the greater the improvement in co-morbidities. The variations between the different types of bariatric surgeries in terms of effectiveness in weight loss, T2DM, and metabolic syndrome remission as well as short- and long-term complications need to be taken into account on an individual basis when making decisions to employ bariatric surgery. The goal of individualizing bariatric treatment and prediction of response remains challenging. Developments in instruments and surgical techniques, including single access, natural orifice approaches, and less-invasive endoluminal bariatric techniques, may offer further benefit in terms of patient acceptability. 94
Footnotes
Author Disclosure Statement
No competing financial interests exist.