
Abstract
The association between subclinical hypothyroidism (SCH) and metabolic syndrome (MetS) is a matter of debate. In this study, we aimed to examine the risk of MetS in SCH through a systematic review and meta-analysis. A systematic search of published literature up to September 2015 was conducted. General population studies were included if they had considered SCH as the independent variable. After data extraction, a meta-analysis was run to assess the odds ratio (OR) of MetS and its components between subclinical hypothyroid and euthyroid groups. Only studies employing Adult Treatment Panel III (ATP III) criteria for MetS were included in the meta-analysis. In the SCH group, female gender was more prevalent [OR = 1.65, 95% confidence interval (95% CI) 1.29–2.13]. Meta-analysis showed no significant difference in MetS prevalence between SCH and euthyroid individuals (OR = 1.13, 95% CI 0.95–1.34). However, the prevalence of central obesity (OR = 1.43, 95% CI 1.04–1.96) was significantly higher in the SCH group. On the other hand, hypertriglyceridemia was more prevalent in the female-only SCH subgroup. In conclusion, although we found some MetS components to be more prevalent in SCH, the prevalence of MetS as defined by ATP III criteria was not increased in SCH. Considerable heterogeneity observed may have influenced the results on MetS components.
Introduction
S
On the other hand, metabolic syndrome (MetS), which is a constellation of certain cardiometabolic risk factors, has increasingly become the focus of a number of studies examining the cardiovascular consequences of SCH. However, evaluating MetS as an outcome is affected by its various definitions. The substantial disagreement over MetS diagnosis 8 has resulted in several clinical criteria being suggested; the two major criteria by the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) and the International Diabetes Federation (IDF) are among them. Remarkably, the key difference between the two is the definition of central obesity, which is in turn a mandatory component in the IDF criteria. Nevertheless, a joint interim statement has been proposed by the IDF and American Heart Association (AHA) in 2009, which agreed that central obesity—although not essential for diagnosis of MetS—must be defined according to population and country-specific definitions. 8
Previous studies, which have employed different MetS definitions and have been conducted in diverse populations with different ethnicity and iodine intake, have come to conflicting results. 4,9 However, one meta-analysis of cross-sectional data concluded that SCH might be associated with increased risk of MetS. 10 Yet, certain factors—including the MetS definition—might have affected these findings.
Therefore, we conducted an update systematic synthesis and meta-analysis of all available published data to examine the association between SCH and MetS, as well as its components.
Research Design and Methods
This systematic review and meta-analysis were run according to the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) 11 and the Meta-analysis of Observational Studies in Epidemiology (MOOSE) 12 statement.
Data sources and search strategy
We searched Cochrane, PubMed/MEDLINE, Web of Science, Scopus, and Iran Medex databases up to September 2015 to identify all related reported studies conducted in the general population. Our search terminology included “Subclinical hypothyroidism,” “TSH,” “Thyrotropin,” “Thyroid function test,” “Metabolic syndrome,” and “Insulin resistance.” In addition, all references from the included articles and relevant reviews were manually searched for eligible studies.
Inclusion criteria and study selection
Three reviewers (A.E., M.E.K., and M.M.) independently screened the titles of the search results and identified relevant studies. Among them, the reviewers independently verified eligible studies based on inclusion criteria. Our inclusion criteria entailed (1) studies of a general otherwise healthy adult population and (2) studies that define the status of MetS in groups of SCH and euthyroid subjects. Disagreement between reviewers was resolved by consensus.
Data extraction
Data extraction was performed independently by two reviewers (A.E. and M.E.K.). For each included study, the following information was collected: (1) type of study; (2) study population; (3) SCH criteria; (4) MetS criteria; (5) number of subjects with MetS in SCH and euthyroid groups; and (6) number of subjects possessing each component of MetS in SCH and euthyroid groups.
Quality assessment
We employed the Strengthening The Reporting of Observational Studies in Epidemiology (STROBE) 13 guidelines to examine the quality of the studies. Two reviewers (M.E.K. and A.E.) independently assessed the quality of studies. The checklist included the adequacy of study design, recruitment of samples, ascertainment of SCH, and control of confounding variables such as age, sex, and body mass index (BMI).
To assess the risk of bias, we took advantages of the AHRQ guideline for cross-sectional and case–control studies. 14
Statistical analysis
The primary outcome was the risk of MetS in SCH subjects [assessed by calculating the odds ratio (OR) with 95% confidence interval (95% CI)]. The secondary outcome was the OR for MetS components between the SCH and euthyroid groups.
I 2 was measured to assess heterogeneity. Considering diversity of the included studies, a random-effects (RE) model was used. To minimize possible heterogeneity, only studies that defined MetS based on ATP III criteria entered the meta-analysis. Metaregression was run to assess the possible causes of heterogeneity. Subgroup analysis for the primary outcome was performed according to gender, geographical regions, and study design (cross-sectional vs. case–control). We also examined the female subgroup for MetS components. Publication bias was assessed by Begg's test. Analysis were carried out using Stata/SE 11.1 15 and RevMan 5.3. 16 Statistical significance was set at P < 0.05 and 95% CIs were quoted throughout.
Results
Study selection
A total of 106 studies were identified through database search. After excluding nonrelevant studies, 43 studies were reviewed by abstracts, from which 23 studies were selected for full text review. Another 12 studies were excluded due to the reasons listed in Figure 1. The remaining 11 studies were selected for systematic review; among them, 8 studies were included in the meta-analysis (Fig. 1).
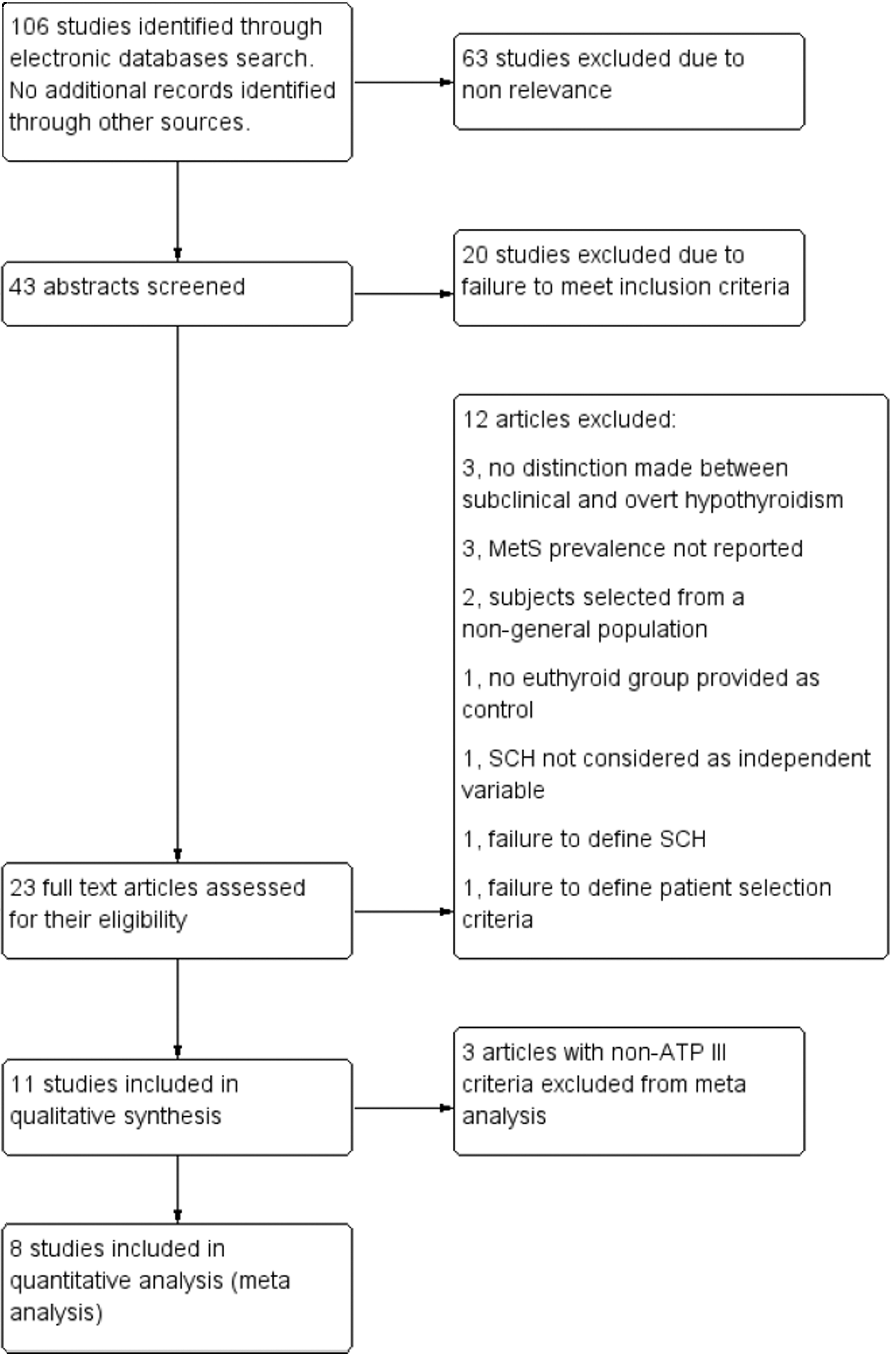
Study flow diagram.
Characteristics of the included 11 studies
A total number of 34,517 subjects (46.27% women) were included. The SCH group comprised 2529 subjects and the euthyroid group consisted of 31,988 individuals. From the 11 examined studies, 2 had a case–control design and 9 had a cross-sectional design (among them 1 had a cohort phase as well). The studies' sample size ranged from 92 (Luboshitzky et al. 17 ) to 10,350 (Nakajima et al. 18 ). Two studies (Ramezani et al. 19 and Luboshitzky) were limited to women. The study by Nakajima et al. had reported their results separately for men and women. The mean age ranged from 34.4 (Ramezani) to 73.6 years (Waring et al. 20 ) (pooled mean age 49.7 years).
Nine studies had used ATP III criteria for MetS definition, with two of them taking advantage of adapted criteria for specific populations (Ramezani
19
and Wang
21
). Nakajima's study applied modified ATP III-based criteria that mandated central obesity as an MetS component and thereby was excluded from the meta-analysis. Liu C et al.
9
employed IDF definition and Lai Y et al.
4
applied China Diabetes Society (CDS) criteria to define MetS (both studies were left out from the meta-analysis) (Table 1 and Supplementary Table S1; Supplementary Data are available online at
ATP III, adult treatment panel III report; CVD, cardiovascular diseases; IDF, International Diabetes Federation; MetS, metabolic syndrome; SCH, subclinical hypothyroidism; TSH, thyroid-stimulating hormone.
SCH was defined in all studies except one. Hergenc's work 22 had made no distinction between SCH and overt hypothyroidism, but considering the reported TSH mean ± SD in the hypothyroid group (7.54 ± 1.60 mIU/L), we came to the conclusion to include their study in the meta-analysis for MetS risk. Prevalence of MetS ranged from 10.11% in the euthyroid group (Nakajima) to 43.5% in the SCH group (Hergenc).
Mean TSH in SCH groups ranged from 5.26 (Wang) to 11.5 mIU/L (Erdogan et al. 23 ). In euthyroid groups, mean TSH ranged from 1.12 (Hergenc) to 1.9 mIU/L (Luboshitzky).
The MetS prevalence by ATP III criteria was found to be 25.96% and 24.49% in SCH and euthyroid groups, respectively.
Meta-analysis
Analysis of the eight studies employing ATP III criteria revealed that compared with the euthyroid group, a higher proportion of female gender was observed among the SCH individuals (OR = 1.65, 95% CI 1.29–2.13). TSH levels and age were significantly increased in the SCH group (weighted mean difference [WMD] = 6.45 mIU/L, 95% CI 4.84–8.06, and WMD = 1.75, 95% CI 0.54–2.97, respectively).
Our meta-analysis showed no significant difference in MetS prevalence between SCH and euthyroid groups (OR = 1.13, 95% CI 0.95–1.34, P = 0.171, I 2 = 37.8%) (Fig. 2). Begg's test results detected no significant publication bias (P = 0.118) (Fig. 3).

Forest plot of association between subclinical hypothyroidism and metabolic syndrome.
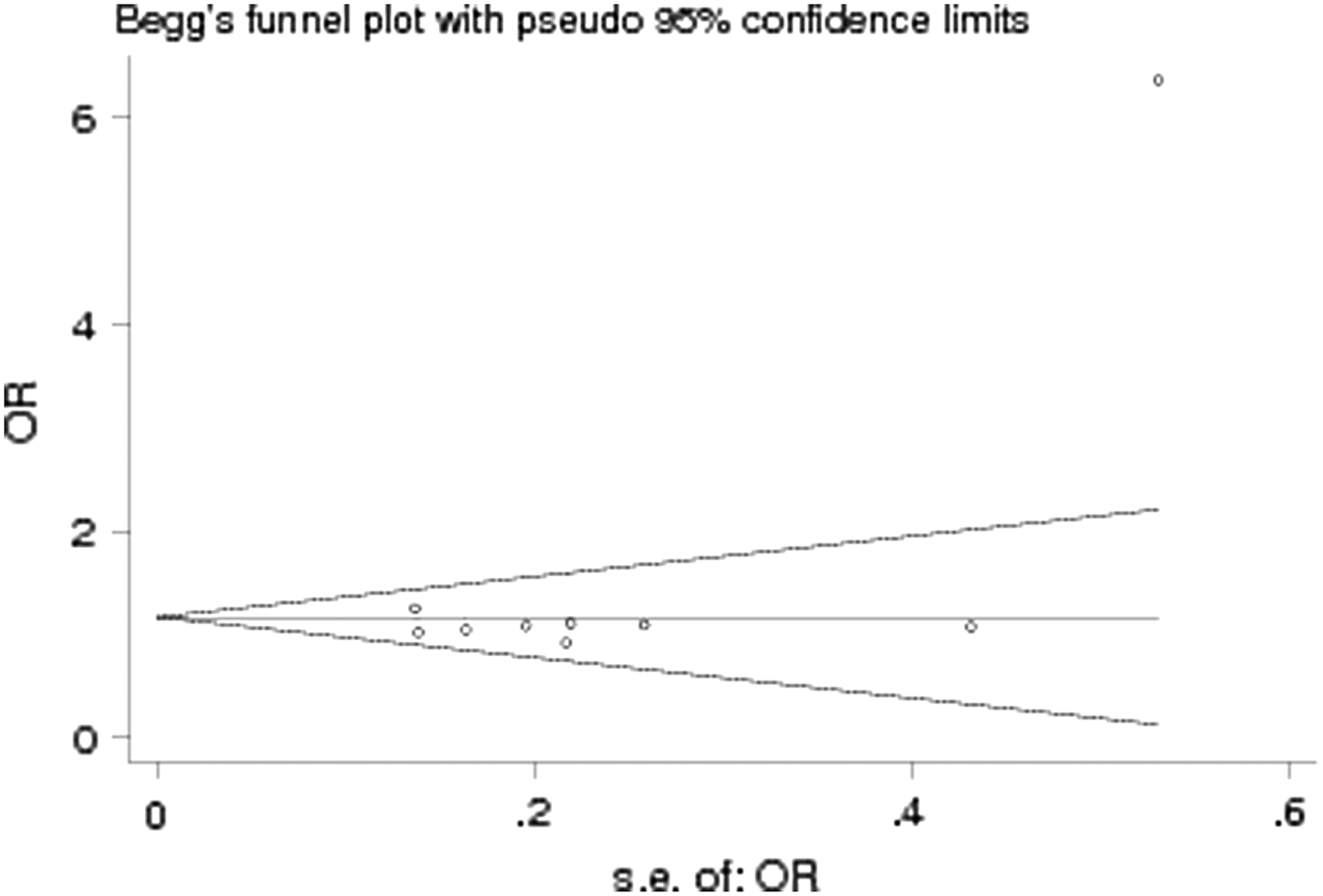
Begg's funnel plot showing no significant publication bias.
Analyzing results of the studies that had addressed the MetS components separately showed that prevalence of central obesity was significantly higher in the SCH group. However, significant heterogeneity was detected (OR = 1.43, 95% CI 1.04–1.96, P = 0.029, I 2 = 68.2%). We observed no significant difference in hyperglycemia, hypertriglyceridemia, low high-density lipoporotein cholesterol (HDL-C), HTN, and BMI between the comparing groups (Table 2). Assessing the possible causes of heterogeneity, metaregression showed that differences in TSH level (P = 0.50), age (P = 0.25), and gender (P = 0.45) between the two comparing groups had no significant relationship with increased odds of central obesity in the SCH individuals.
Including studies by Erdogan, Garduno-Garcia, Luboshitzky, Ramezani, and Wang.
95% CI, 95% confidence interval; HDL-C, high-density lipoporotein cholesterol; OR, odds ratio.
Subgroup and sensitivity analysis
Subgroup analysis was performed based on gender, geographical regions, and study design (Table 3).
Meta-analysis confined to female-only participants revealed that there is no statistically significant difference in the risk of MetS between the comparing groups (OR = 2.28, 95% CI 0.34–15.10). On the other hand, the difference between SCH and euthyroid groups in this subgroup was statistically significant for BMI (WMD = 0.95, 95% CI 0.19–1.70, I 2 = 0%, P = 0.014) and hypertriglyceridemia (OR = 1.66, 95% CI 1.13–2.43, I 2 = 11.0%, P = 0.009). The prevalence of HTN was significantly increased in the SCH group if only employing the fixed-effects model (FE: OR = 1.89, 95% CI 1.13–3.16, I 2 = 36.2%, P = 0.016; RE: OR = 1.97, 95% CI 0.97–4.02, P = 0.063). The results for central obesity, hyperglycemia, and low HDL-C showed no statistically significant difference between the groups. Data for men could not be extracted, except in Nakajima's study, thus no meta-analysis for the male subgroup was conducted. No significant results were observed in either cross-sectional or case–control subgroups. In addition, analyzing geographically based subgroups returned no significant results.
Sensitivity analysis indicated that omitting each study had no substantial effect on the pooled OR (Supplementary Table S2).
Risk of bias
In cross-sectional studies, the risk of bias was estimated to be low in most indices of the AHRQ guideline. However, in case–control studies, the risk of bias appeared to be mostly unclear. In cross-sectional studies, the highest risk of bias was due to failure of about 30% of studies to rule out any impact from an unintended exposure. Failure to account for important confounding/modifying variable and failure to appropriately handle missing data composed the highest risk of bias in case–control studies (Supplementary Figs. S1–S4).
Discussion
In this meta-analysis, we examined the relationship between SCH and MetS, as well as its components, in a general population. Our study found no significant increase in MetS odds in SCH individuals. However, we observed greater prevalence of central obesity in subjects with SCH.
Previously, a meta-analysis by Ye et al. had examined the relationship between SCH and MetS. 10 This study, which was limited to cross-sectional studies published up to 2012, reported the risk of MetS to be higher in the SCH group (OR = 1.20, 95% CI 1.05–1.36). However, the authors did not apply a uniform MetS definition for their data synthesis. Moreover, one of the studies included in the Ye et al. meta-analysis (Lai CC et al. 24 ) comprised subclinical hyperthyroid subjects as its control group. The main differences between our study and Ye et al.'s meta-analysis (both in structure and results) are depicted in Supplementary Table S3.
Findings on MetS components
Examining the risk of MetS components in SCH, we found the difference in central obesity to be statistically significant (OR = 1.43). Interestingly, our results on central obesity and BMI were not consistent. This might further emphasize the importance of central obesity—and not merely increased BMI—in possible metabolic alterations of SCH.
The effect of SCH on lipid profile has been vastly examined by other studies. Nevertheless, the results have been inconsistent. 25 The National Health and Nutrition Examination Survey (NHANES) III study showed that in individuals older than 40 years, the HDL-C level has been lower in the SCH group. 22 In addition, the European Prospective Investigation in Cancer and Nutrition-Norfolk prospective population study reported that SCH individuals had increased total cholesterol and triglyceride (TG), but lower HDL-C levels than the euthyroid group. However, the latter was only observed in women. 26 Accordingly, one meta-analysis by Liu X-L et al. 7 reported the TG level to be significantly higher in the SCH group (WMD = 13.19 mg/dL, P < 0.001). They found no significant difference in the HDL-C level between SCH and euthyroid groups (WMD = −0.50 mg/dL, P = 0.481). For both analyses, substantial heterogeneity was reported (I 2 = 90.9% and 73.2%, respectively). Variation in basic specifications (e.g., age, gender, ethnicity, smoking, and insulin resistance) of population examined in these studies might attribute to these contrary findings. For example, Liu's studied individuals were older than ours and the proportion of female gender was also higher in their population (55.2 years vs. 49.7 years and 59.9% vs. 46.3%, respectively). Interestingly, a Cochrane review of thyroid hormone replacement in SCH has shown that there was no significant treatment effect on HDL-C and TG levels. 25
Contrary to our results, two meta-analyses have previously shown the systolic blood pressure (SBP) level to be higher in the SCH group. 5,27 Cai et al. have also reported significantly increased diastolic blood pressure (DBP) levels in the SCH group. 5 Again, it is speculated that alteration in underlying specifications of the studies populations might explain the inconsistency in blood pressure results observed.
In our study, the SCH and euthyroid groups were significantly different in gender proportion. The meta-analysis of female-only studies revealed that while the odds of MetS in the SCH group did not differ significantly from euthyroid individuals, women with SCH have higher BMI and increased prevalence of hypertriglyceridemia. Interestingly, odds of central obesity in this female-only subgroup did not statistically differ between the two comparing groups. Nevertheless, since no similar meta-analysis was conducted for male subjects, any conclusion drawn from these findings regarding association between gender and MetS components should await further investigations.
Previous investigations have suggested gender-specific pathophysiological differences in the MetS. Lipid accumulation patterns differ between men and women, and premenopausal women are more prone to peripheral obesity than central obesity. Besides, there are evidences that confirm while, among the MetS components, high SBP and DBP appear to be more important factors in men, elevated waist girth and low HDL-C impose a more significant effect on women. 28
Analyzing MetS and its components in the male subgroup, Nakajima et al. reported no differences between euthyroid and SCH groups (OR = 1.01, 95% CI 0.69–1.48). Besides, they showed that free T4 levels were significantly lower in women with SCH than in the male subgroup; a finding that might explain the different metabolic alterations in men and women with SCH. 18 Further gender- and age-matched studies are needed to verify the role of gender in association between SCH and the lipid profile.
Confining the meta-analysis to ATP III studies is one of the advantages of our study since including investigations with different MetS definitions might be considered as a potential flaw. Nevertheless, there are a sizable number of meta-analyses treating MetS with mixed definitions as the dependent or independent variable in the literature. 29 –32
Effect of MetS criteria in estimating the prevalence of MetS has been reported in various studies. One study has found the prevalence of MetS in Australia to be 20.9%, 18.4%, and 15.4% by WHO, ATP III, and EGIR criteria, respectively. 23 Should one assume that some MetS criteria are less sensitive than others to detect subtle metabolic changes by SCH remains a subject for further investigations.
Our results need to be interpreted within the context of the limitations we encountered. First, except one, the pool of relevant studies identified through our systematic search consisted of cross-sectional and case–control types. Therefore, the results might not assist in evaluating the causal relationship between SCH and MetS. Second, we did not have access to stratified ORs for age and gender in all studies. Keeping in mind the significant difference between our comparing groups in their mean age and gender, we are not able to exclude the effect of these confounding factors on our pooled effect size. Third, the heterogeneity observed in the included studies, especially when analyzing MetS components, was quite considerable. This substantial heterogeneity—which is a function of multiple factors, including various cutoffs for SCH definitions, concomitant use of medication, duration of SCH, smoking, and presence of antithyroid antibodies—urges us to interpret the results of this study with even more caution. Notably, our included studies have employed different exclusion criteria. While some have clearly excluded individuals with diabetes or cardiovascular diseases, others have not reported their exclusion criteria thoroughly. Thereby, we were not able to examine the effects of possible underlying cardiovascular conditions on our results.
In conclusion, our meta-analysis indicated that although central obesity is more prevalent in SCH individuals, MetS prevalence is not higher in this group. Moreover, we observed increased BMI and low HDL-C prevalence in women with SCH and no significant association between the TSH level, age, and gender and odds of central obesity in SCH. Prospective cohorts with adjusted groups for confounding factors mentioned above would be needed to provide more precise information.
Footnotes
Acknowledgments
The authors wish to thank Ms. Ameneh Ebrahimi and Ms. Zahra Emami (staff of Endocrine Research Center) for their kind assistance. The authors are particularly grateful to Dr. Mohammad Reza Rouhollahi for critical reading of the manuscript. They also express their gratitude to Dr. Tatyana Mityukova for kindly providing a copy of her original article, “Effect of Thyroid Status on the Development of the Metabolic Syndrome in People of Reproductive Age.”
Author Disclosure Statement
No conflicting financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.