
Abstract
Background:
Health care costs increase with the presence of metabolic syndrome and present a significant burden to companies throughout the world. Identifying effective behavioral programs within the workplace can reduce health care costs. We examined the effect of a voluntary worksite program on weight loss and metabolic syndrome.
Methods:
Participants (N = 3880, from 93 companies) volunteered within their workplaces to participate in a 10-week weight loss program (Naturally Slim) focused on self-monitoring, eating behaviors, understanding hunger signals, reducing refined carbohydrate and sugar intake, and increasing protein intake to 25%–30%. Primary outcomes included weight loss and metabolic syndrome prevalence. Secondary analyses examined the individual components of metabolic syndrome and a categorical analysis within each World Health Organization body mass index category.
Results:
Overall, women and men lost 9.4 (−4.8%) and 13.2 pounds (−5.8%), respectively. Each metabolic risk factor for both genders had a significant improvement but men exhibited the largest relative improvement for each risk factor. At baseline, 43% of women and 52% of men presented with metabolic syndrome, which was reduced to 30% in women and 26% in men (P < 0.001 for each) at the conclusion of the program. Secondary analysis demonstrated that individuals with greater baseline levels of metabolic dysfunction had larger metabolic improvements, similar benefits to risk factors across baseline body mass index categories, and the greater the weight loss, the greater the metabolic benefit.
Conclusion:
Our results demonstrate that a worksite program targeting core behavioral skills associated with weight loss is an effective strategy to reduce weight and improve the components of metabolic syndrome amongst at-risk employees.
Introduction
A
Findings from Diabetes Prevention Program reinforce the value of behavioral lifestyle programs that focus on reducing caloric intake and increasing regular physical activity. Specifically, the Diabetes Prevention Program has shown that as little as 4% weight loss obtained through physical activity and calorie reduction over 2.5 years reduces the risk for developing diabetes by 58% in high-risk individuals. 5,6 Equally important to the reduction in diabetes is the reduction in “precursor” risk factors before T2D becomes manifest. These risk factors include insulin resistance, overweight/obesity status, and MetS. In addition to being a risk factor for T2D, MetS is a well-recognized independent risk factor for cardiovascular disease, cancer and all-cause mortality. 7 Economically, these factors are important to employers as cost estimates range from $201–$644 per employee per year depending on obesity status (normal weight, overweight, obese) and may increase to ∼$4,720–$7,606 per person per year depending on the presence of varied MetS component features and concurrent diabetes. 8,9 Further, if T2D becomes manifest, individuals who also haveMetS are at a higher risk for respective morbidities and mortality compared with those without T2D. 10,11 Given the broad physiological benefits associated with exercise training, diet, and behavioral interventions, the continued advocacy for such measures is important for individuals presenting with or at risk for MetS.
Unfortunately, the prevalence of MetS is fairly high within various corporate environments, and most employers are directly responsible for at least part of the health care costs of their employees. 12,13 Worksites present a unique opportunity to introduce voluntary programs targeted toward weight loss and MetS. However, there are many barriers to delivering weight loss programs in the workplace including issues of privacy, competing time commitments, lack of suitable facilities, interruptions to the workday, access, and scalability. Identifying effective behavioral weight loss programs that can be utilized across large and geographically dispersed populations is of great public health importance and has been shown to reduce health care costs, improve employee mental health, and increase presenteeism and productivity. 14 –18
Methods
Participants
Herein we describe data obtained from a convenience sample of 93 employers comprised of 3,880 employees, presenting before and after participation in a voluntary, commercialized weight loss program offered within each company. Our study was reviewed by an ethics committee (Chesapeake Internal Review Board, Columbia, MD) and determined not to require internal review board oversight according to the tenets of the United States Department of Health and Human Services regulations, at Code of Federal Regulations Title 45 part 46 (Protection of Human Subjects). Data were fully de-identified and did not contain the names of the employees, their respective places of employment, or the city/state of their residence but did include age, gender, weight, and appropriate clinical lab measures, including blood work, waist circumference, and blood pressure.
Program
Employees volunteered within their workplace to participate in a 10-week corporate weight loss program composed of weekly lessons (Naturally Slim, Inc.). Overall, programming for our intervention was modeled after the Diabetes Prevention Program methodology that has been previously described. 19 In brief, lessons included elements found in standard behavioral health programs such as self-monitoring, goal setting, stimulus control, modification of eating habits, and problem solving, focusing on mindful, healthy eating and understanding hunger signals. While the program does not eliminate or focus on any specific food group or macronutrient, per se, it does emphasize reducing carbohydrate and sugar intake, particularly refined sugar and maintaining a protein intake of 25%–30% of total calories. Lessons are delivered using a web-based distance-learning platform where participants can watch their lessons via the Internet. Participants were also encouraged to partake in moderate intensity physical activity, primarily walking, according to the National Institutes of Health Consensus Development Panel on Physical Activity and Cardiovascular Health, yet data were not recorded to record their quantity of exercise. 20
Recruitment and risk factor assessment
Our data comes from a sample of convenience with neither a randomization nor a nonintervention control group. Participants were often made aware of the program through in-house emails and flyers. Employees could then apply for enrollment via the website. Many, but not all, employers limited participation to individuals with MetS. All participants performed a baseline risk factor screening inclusive of National Cholesterol Education Program Adult Treatment Panel III MetS component features. Due to the nature of worksite screening, follow-up visits were not always right after the last class. For the purposes of this analysis, follow-up visits occurred within 20 weeks of the program start. There was no minimal level of participation to be included this analysis, thus the potential range between baseline and follow-up testing was 1–20 weeks. The average time between baseline and follow-up examinations was 17.8 ± 10.1 weeks for the women and 19.6 ± 12.8 weeks for the men, respectively.
Statistics
Due to baseline differences in the prevalence in MetS between women and men, we opted to perform separate gender analyses and adjust for gender within the combined analyses. We initiated our analysis by computing the arithmetic mean and standard deviation of each variable. Mean and percent change was calculated, and general linear models were used to test for differences between genders. Results are presented as adjusted least-squares means and 95% confidence intervals. Pre- and post-prevalence of MetS and the associated risk factor components were tested using chi-squared tests, and within-group differences examined using McNemar's test. Categorical analyses were also conducted for which gender-adjusted least squares means and confidence intervals were calculated across categories using general linear models. Trend across groups was assessed using a standard regression model. In order to examine the potential benefit of the weight loss program across different levels of baseline weight, participants were categorized based on World Health Organization body mass index (BMI) categories. 21 To assess the benefit of the program across increasing levels of metabolic risk, we categorized individuals based on the number (0–5) of the MetS risk factors present at baseline. To assess the shape of the weight loss benefit curve, we examined changes in risk factors across levels of weight loss: none, 0%–3%, 3.1%–5%, 5.1%–7.0%, 7.1%–10.0%, and > 10% weight loss. All reported P values are two-sided. All analyses were performed using SAS version 9.4.
Results
We have presented the baseline and change data for the weight and the MetS risk factors in Table 1. The average age was 46.0 ± 10.1 years for women, and 46.1 ± 10.8 years for men. The mean BMI for the women (32.9 ± 6.1 kg/m2) and the men (32.0 ± 5.3 kg/m2) fell into the class 1 obese category. The men had worse metabolic profiles than the women. Following the intervention, women had a mean weight loss of 9.4 pounds (−4.8%), and the men lost 13.2 pounds (−5.8%). Both the relative and absolute weight loss was statistically greater in the men compared with the women. In categorical analysis, 56% of men lost at least 5% and 17% lost at least 10% body mass, while 46% of women lost at least 5% and 10% lost at least 10% of body mass. For the MetS risk factors [except high-density lipoprotein (HDL) in women], there was a significant improvement in both women and men, with the improvement being larger for each risk factor in men except waist circumference.
Data are mean ± standard deviation (SD) or 95% confidence interval (CI) for change at follow-up.
SI conversions: to convert pounds (lbs) to kg, divide by 2.2; for inches to centimeters, divide by 2.54. To convert blood values to mmol/L, multiply glucose by 0.555, triglycerides by 0.0113, and HDL by 0.0259.
BMI, body mass index; Circ., circumference; DBP, diastolic blood pressure; HDL, high-density lipoprotein; SBP, systolic blood pressure.
MetS and related components
We have presented the prevalence of MetS and each of the components at baseline and follow-up in women and men in Fig. 1. At baseline, 43% of women and 52% of men presented with MetS. After the intervention, 30% of women and 26% of men presented with MetS. All metabolic risk factors showed a significant improvement for men. We observed a similar response in women except for HDL cholesterol. Men also demonstrated a greater relative improvement for each risk factors compared with the women except for waist circumference.
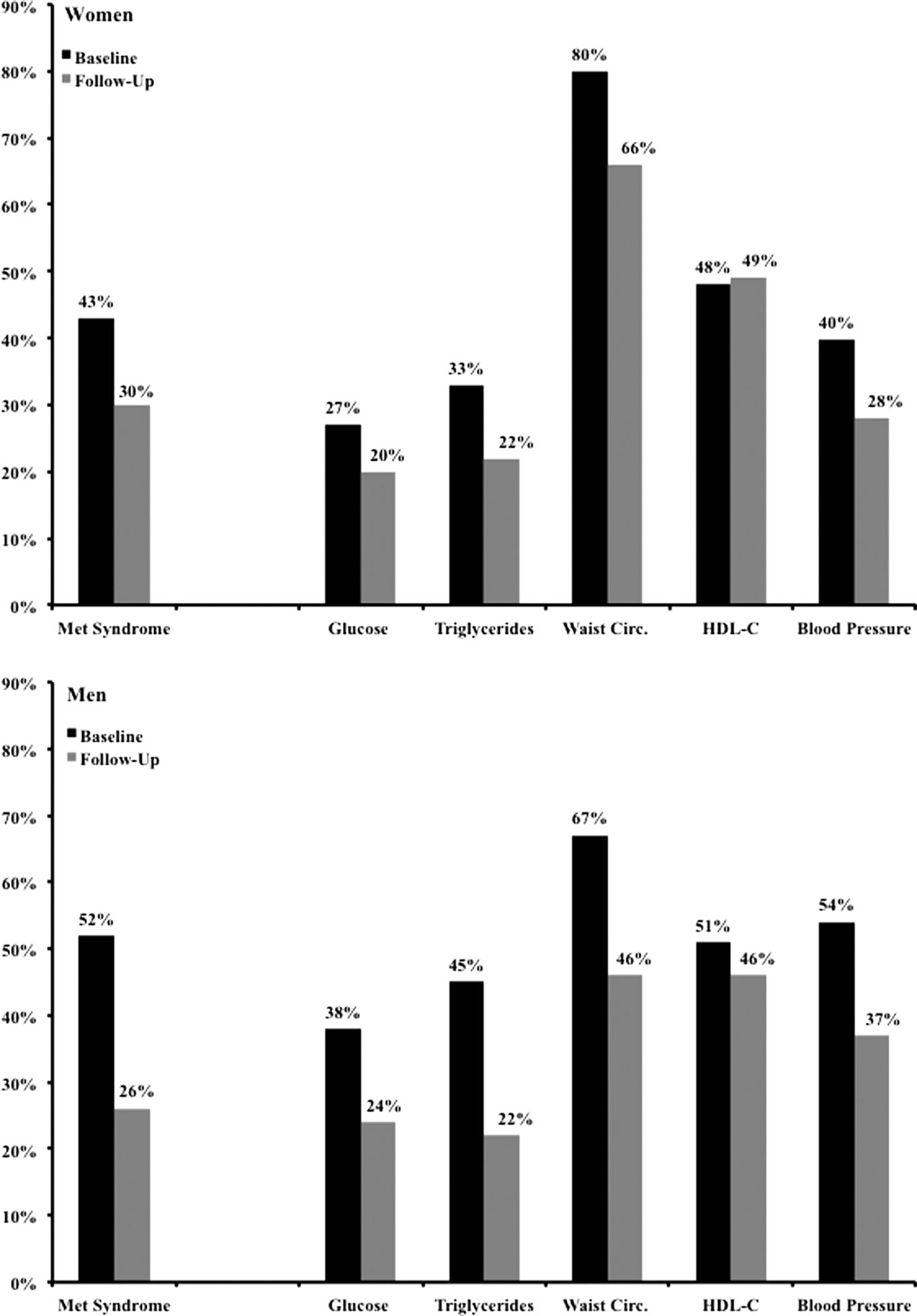
Data represent the percent reduction of metabolic syndrome and National Cholesterol Education Program Adult Treatment Panel III individual composite features for women (n = 2629) and men (n = 1251).
In order to examine the impact of baseline weight on changes in weight and metabolic risk factors, individuals were grouped based on baseline BMI and changes in weight and risk factors were examined within these standard weight classifications (Table 2). While the absolute mean weight loss was greater across level of baseline BMI (P trend < 0.001), the percent weight loss was not (P = 0.1). These data suggest that the relative weight loss was independent of baseline weight. Similarly, though there were significant within-group changes in glucose, triglycerides, systolic and diastolic blood pressure, these changes were not associated with baseline BMI category. While the changes in HDL cholesterol and waist circumference were statistically associated with baseline BMI, given the flat trend of the data, the clinical significance of this association is questionable. In general, the data from this analysis suggests that baseline weight does not significantly impact the magnitude of relative weight loss or the clinical benefit associated with weight loss with all groups benefitting equally.
Data are least squares means (95% CI) with adjustment for gender.
SI conversions: to convert lbs to kg divide by 2.2; for inches to centimeters, divide by 2.54. To convert blood values to mmol/L, multiply glucose by 0.555, triglycerides by 0.0113, and HDL by 0.0259.
To explore the magnitude of improvement of risk factors across level of metabolic dysfunction, we categorized participants based on number MetS risk factors present at baseline (Table 3). For mean weight and all metabolic risk factors there was a strong trend between the magnitude of improvement and number of MetS risk factors at baseline. There was, however, no trend for percent weight loss across the number of MetS risk factors, suggesting that the same percent weight loss has similar benefit across all levels of metabolic dysfunction. Table 4 summarizes the data for changes in metabolic risk factors by categories of percent weight loss and as expected, the greater the weight loss, the greater the clinical benefit. This was observed in all risk factors except HDL cholesterol in women.
Data are presented as least squares means (95% CI) with adjustment for gender.
SI conversions: to convert lbs to kg divide by 2.2; for inches to centimeters, divide by 2.54. To convert blood values to mmol/L, multiply glucose by 0.555, triglycerides by 0.0113, and HDL by 0.0259.
Data is presented as least squares means (95% CI) with adjustment for gender, except HDL in which men and women were analyzed separately. SI conversions: to convert lbs to kg divide by 2.2 and inches to centimeters (2.54). To convert blood values multiple glucose (0.555), triglycerides (0.0113), HDL (0.0259) to mmol/L.
Discussion
Our analysis demonstrates that a web-based behavioral program is effective in producing clinically meaningful weight loss, as well as substantial improvements to the MetS risk factors. The men in our cohort were heavier than the women at baseline and exhibited greater weight loss. Both genders exhibited significant improvements in MetS as well as various risk factors, with the men having greater improvements compared with the women. This may be due to the greater degree of baseline metabolic dysfunction coupled with a more weight loss observed in the men. An interesting finding is that baseline weight had a negligible effect on the percent weight loss and the absolute improvement in metabolic risk factors. In other words, individuals of all weight classes had similar clinical improvements. The strongest predictor of clinical benefit was degree of baseline metabolic dysfunction as those with the most MetS risk factors at baseline had the largest clinical improvement.
It is widely accepted that the most effective weight loss programs are conducted in person, with telephone-based programs ranking a close second in effectiveness. 22 –24 Neither of these strategies is scalable in a cost effective manner, particularly in the workplace. Utilizing a web-based learning platform allows participants to watch the weekly lessons at their convenience in a location of their choice, thus directly overcoming the workplace barriers of privacy, suitable facilities, interruptions to the workday, and access. 22,25 –28 In fact, we observed that most classes were watched in the evening at home. The use of a web-based learning platform allows for the inclusion of substantially more employees for a given budget compared with in-person or telephonic programs. This creates an opportunity to include the much larger population of the moderate risk individuals as opposed to focusing exclusively on the smaller number of high risk individuals. Given that 34% of Americans have MetS, strategies to increase the number of individuals treated is of both clinical and public health importance. 29
With greater frequency, companies are adopting preventive strategies for reducing obesity related diseases and healthcare costs. For example, Wang et al. (2006) reported that estimated annual healthcare spending rises with overweight and obese participants by ∼$120 per unit increase in BMI. 30 Similar findings have been shown that inpatient admissions, outpatient visits, professional claims, and prescription drugs were higher for obese patients, 31 as well as indirect costs associated with absenteeism and productivity. 32 In a large multiuniversity-based study examining 10,026 employees, obese employees were shown to have a 20% higher number of physician visits versus normal weight employees (16%) and 26% more emergency rooms visits. Overall, this equated to additional annual costs for overweight ($201) and obese ($644) employees versus normal weight employees. 8 The presence of MetS further complicates healthcare expenditures.
The estimation of healthcare costs relative to MetS depends on the number of component features present within each individual. Nichols and Moler (2011) reported that in a fully adjusted statistical model, hypertension ($550), obesity ($366), low HLD-C ($363), and high triglycerides ($317) were all significantly associated with higher annual health costs. The author's further report that impaired fasting glucose was not significantly associated with annual health care costs, yet the addition of qualifying each MetS component increased total annual healthcare burden in a stepwise fashion ranging from $3,641 to $5,843 for individuals with zero and five qualifying MetS features, respectively. 9 These annualized costs increased further with the development of diabetes, a fact that cannot be taken lightly given that the concurrent presence of MetS and diabetes also increases mortality risk with each additional MetS component. 10
Obesity and MetS typically stem from an obesogenic environment comprised of cultural, social, genetic, and socioeconomic factors. 33 Within each of these characteristics, the overconsumption of “junk” and fast foods that are high in refined sugars, coupled with physical inactivity is a consistent finding related to the cause of both. 34 Though the U.S. Department of Agriculture publishes dietary guidelines, most Americans fail to achieve these recommendations and show a pattern of continual increase in the consumption of refined grains coupled with a decrease in consuming whole grains, fruits, and vegetables. 35 Consequently, this food ingestion pattern associated with a “Western diet” has led to an increased risk for obesity, dyslipidemia, and insulin resistance. 36,37 For example, data from Framingham Heart Study has shown a positive association between an “empty calorie pattern” of eating and the prevalence of MetS as compared with a healthier eating pattern in obese women. 38 To the contrary, individuals consuming a diet consistent with a Mediterranean Diet and DASH diet demonstrate a lower risk of cardiovascular disease, obesity, insulin resistance, hypertension, and MetS. 39 –45 The success of both of these diets may be influenced by the glycemic load and index of the recommended foods given their emphasis on whole grains food consumption, which has been shown to decrease the prevalence of MetS compared with diets containing higher quantities of refined carbohydrates. 46 –48
Currently, National Cholesterol Education Program Adult Treatment Panel III guidelines recommend ingesting a diet composed of ∼15% protein, 50%–60% carbohydrate, and 25%–30% fat for individuals presenting with MetS. 7,29 Yet, other groups recommend altering macronutrient composition in favor of increasing protein and lowering carbohydrates. 49,50 Studies examining macronutrient manipulations in conjunction with low to moderate caloric intakes demonstrate favorable alterations in MetS risk factors. 51,52 These recommendations follow a partitioning of macronutrients similar to those originally proposed by Banting in 1869. 53 For example, Dansinger et al. (2005) reported that participants assigned to either the Atkins, Zone, Weight Watchers, or Ornish diets focusing on weight loss demonstrated similar overall metabolic improvements in cholesterol, various risk factors, and weight loss as long as participants were compliant to their respective diets. 51 Similar findings were also reported in overweight, premenopausal women following the same diets, as well as the addition of the LEARN (Lifestyle, Exercise, Attitudes, Relationships, and Nutrition) diet. 52
Several other diet studies have also shown when total energy intake is moderate in individuals with baseline metabolic dysfunction, that regardless of macronutrient partitioning, MetS risk factors especially fasting glucose, triglycerides and HDL cholesterol are improved. 51,52 It has been further demonstrated that a reduction in carbohydrate intake, even without weight loss in individuals with baseline metabolic dysfunction, significantly reduces metabolic risk concordant to reduced carbohydrate intake. 54 –58 The fact that many companies utilize MetS as their eligibility criterion resulted in a data set enriched with individuals with metabolic dysfunction. Thus, the large metabolic benefit with modest weight loss is not unexpected given the programs emphasis on reducing sugar and carbohydrate intake. While the long-term effects of such dietary strategies are still debated, a consistent finding amongst these reports is that adherence to various dietary and macronutrient manipulations appear to produce similar results. The strength of these findings demonstrates that there is adequate room for personal preference regarding diet composition if a moderate total energy intake is maintained. While these types of dietary interventions have gained in popularity, they still remain a point of contention amongst some medical, dietary, and public health communities. 59 –61 These programs may also have particular utility in light of the recent implementation of the Affordable Care Act. Cahalin et al. have reviewed key issues on this matter recently. 62,63
A limitation of our study is the lack of a control group and absence of dietary records denoting a change in dietary intake. While this is a concern, this criticism is tempered by the observation that numerous large behavioral and pharmaceutical weight-loss studies have observed that control groups typically demonstrate a 2% weight loss, and given our large sample size it is highly likely that the data for both women and men would have remained statistically significant. The short-term follow-up is also a concern, but given that this data was derived from the compilation of individual worksite initiatives and not as part of formal research study, the duration of follow-up was out of our direct control. While weight loss is important, weight loss maintenance is equally, if not more important. As such, we cannot generalize our findings nor make any meaningful conclusions about maintenance from this data set beyond the 10-week study period.
The major strength of our study is that we observed an inverse dose response between magnitude of percent weight loss and improvements in MetS risk factors using a voluntary, employer-based program. The primary benefit of such a program is that it is scalable to company needs, utilizing a computer interface in conjunction with individual counseling. Given the magnitude of weight loss and reduction in MetS prevalence among participating employees, future investigations should examine the “downstream” effects relative to company healthcare economic benefits.
Footnotes
Author Disclosure Statement
T.S. Church receives honoraria for lectures from scientific, educational, and lay groups. Dr. Church also has a book entitled Move Yourself: The Cooper Clinic Medical Director's Guide to All the Healing Benefits of Exercise. Dr. Church has received research funding from the American Heart Association and the National Institutes of Health as well as unrestricted research funding from Coca-Cola. He has overseen study sites for large pharmaceutical trials funded by Sanofi Aventis, Orexigen, Arena, and Amylin and is a member of the Jenny Craig Medical Advisory Board and has served as a consultant to Technogym, Trestle Tree, Vivus, Lockton-Dunning, and Neuliven Health. In addition, he serves as the senior medical advisor for Catapult Health.