
Abstract
Background:
Associations between metabolic syndrome (MetS) and chronic kidney disease (CKD) has not been extensively studied in elderly Asians, who in general have lower body mass index (BMI) than European populations.
Methods:
A cross-sectional analysis was conducted including 159 community-living elderly Japanese women. MetS was defined by the modified National Cholesterol Education Program Adult Treatment Panel III criteria, but using a BMI ≥25 kg/m2 instead of waist circumference and renal function was assessed according to the Kidney Disease Outcomes Quality Initiative CKD classification. Creatinine-based and cystatin C-based estimated glomerular filtration rate (eGFR) and the average of the two eGFRS were used.
Results:
Prevalence of CKD was much higher when creatinine-based eGFR was used than the prevalence obtained when cystatin-C based equations were used (46.5% vs. 12.6%, P < 0.001). Eighteen (11.3%) women met MetS criteria. Both the presence of MetS and the number of MetS components were associated with higher prevalence of CKD using the average eGFR (all P < 0.05) but not using creatinine-based (P = 0.86) and cystatin C-based (P = 0.12) eGFR alone. Lower average eGFR and higher prevalence of CKD using average eGFR were evident in even women with only one MetS component, 89% of whom had elevated blood pressure.
Conclusions:
Prevalence of CKD varied substantially depending on the used equation. In nonobese, elderly Japanese women, both the presence of MetS and the number of MetS components were associated with higher prevalence of CKD and elevated blood pressure may play an important role in these associations. These findings should be confirmed in studies employing more participants with MetS diagnosed using standard criteria (waist circumference instead of BMI).
Introduction
C
Studies suggest that cystatin C is less dependent upon diet and muscle mass than creatinine and it is assumed that it should provide more accurate GFR estimates, particularly in populations with reduced muscle mass, such as the elderly. 15,16 Recently, the average (eGFRaver) of creatinine-based and cystatin-C based eGFR (eGFRcys) has been reported to have greater precision and accuracy than the individual creatinine and cystatin C equations. 17 The eGFRaver provides the most precise and accurate GFR among people who have mildly decreased GFR (eGFRcreat of 60 to 74 mL/min/1.73 m2). 17 Further, it has been reported that the mortality risk was higher across all levels of decreased eGFR with cystatin C-based equations compared with creatinine-based equations. 18 However, as far as we know there is no report that studied kidney function employing average eGFR in the Asian elderly and hence that examined the relationship between CKD diagnosed using eGFRaver and MetS. Therefore, we evaluated these issues in community-living elderly Japanese women.
Methods
We examined 159 free-living elderly women whose details have been reported elsewhere. 19,20 They were residents in Nishinomiya City and were recruited as volunteers by local welfare commissioners from the city of Nishinomiya, Hyogo, Japan. Subjects with clinically diagnosed acute or chronic inflammatory diseases and cancer were excluded from the study. Although 43, 9, and 58 women (27.0%, 5.7%, and 36.5%, respectively) reported to be receiving statins, antidiabetic drugs, and antihypertensive drugs, respectively, detailed drug information was not available. Hypertension (58 women on antihypertensive medication and 46 women with systolic/diastolic BP ≥140/90 mmHg without medication) was found in 104 women (65.4%), whereas diabetes mellitus was found in 12 women (7.5%) [9 on antidiabetic medication and 3 with hemoglobin A1c (HbA1c) ≥6.5% without medication]. This research followed the tenets of the Declaration of Helsinki. The design of this study was approved by the Ethical Committees of Mukogawa Women's University and written informed consent was obtained from all participants.
Anthropometric indices and BP were measured after an overnight fasting. Thereafter, blood samples were obtained from the cubital vein. We evaluated routine chemical parameters, including glucose, insulin, liver enzymes, and complete blood count as previously reported. 20,21 HbA1c was measured by an immunoassay using an autoanalyzer (JCA-BM9030, JEOL Ltd.). Insulin resistance (IR) was evaluated using homeostasis model assessment (HOMA-IR). 22
Metabolic syndrome was defined using the modified criteria of the National Cholesterol Education Program Adult Treatment Panel III guidelines. 23 Because body mass index (BMI) is not inferior to waist circumference as a practical marker of the metabolic risk clustering in Japanese 24 and because BMI may be better than waist circumference for defining metabolic syndrome in Japanese women, 25 adiposity was defined using Asian criteria as BMI ≥25.0 kg/m2. 26 Elevated BP was defined as systolic/diastolic BPs of 130/85 mmHg or greater and/or current use of antihypertensive medicine. Hypertriglyceridemia was defined as a serum triglyceride level of 150 mg/dL or greater. Low high-density lipoprotein (HDL) cholesterol level was defined as less than 50 mg/dL for all participants are women. Impaired fasting glucose (IFG) was defined as fasting plasma glucose levels of 100 mg/dL or greater and/or current use of antidiabetic medicine. Metabolic syndrome was defined as the presence of three or more components. 23
Serum creatinine was measured enzymatically using an autoanalyzer (AU 5200, Olympus) and cystatin C by latex immunoassay using a commercially available kit (IatroCys-C, Mitsubishi Chemical Medience). Coefficients of variation of creatinine and cystatin were 1.0% at 0.71 mg/dL and 1.2% at 0.70 mg/L, respectively. The eGFR was calculated using the equation recommended by the Japanese Society for Nephrology. 27,28 The average (eGFRaver) of eGFRcreat and eGFRcys 17 were calculated in each participant and was used in analysis. CKD was defined as an eGFR of less than 60 mL/min/1.73 m2. 2
Data are presented as mean ± standard deviation unless otherwise stated. Due to deviation from normal distribution, serum levels of liver enzymes, insulin, and HOMA-IR were logarithmic transformed for analysis. Comparisons between the control and MetS groups were made with two-sample t-tests. The association of CKD and eGFR with the number of components of MetS and Ptrend were derived using Jonckheeree-Terpstra test or analysis of variance when appropriate. A two-tailed P < 0.05 was considered statistically significant. All calculations were performed with SPSS system 15.0 (SPSS Inc.).
Results
As previously reported, 19,20 participants were relatively healthy, community-living, ambulatory elderly women. Estimated GFRcreat (62 ± 14 mL/min/1.73m2) was substantially lower than eGFRcys (80 ± 20 mL/min/1.73m2, P <0.001), and hence, prevalence of CKD was much higher when using eGFRcreat than using eGFRcys (46.5% vs. 12.6%, P < 0.001). 0f 159 women, 31 (20.1%) had CKD using eGFRaver and 18 (11.3%) met MetS criteria. Among components of MetS, elevated BP was the most prevalent (122 women; 76.7%; hypertension in 104 women), followed by hypertriglyceridemia and obesity in 28 (17.6%) and 26 women (16.4%), respectively. Low HDL cholesterol and IFG were found in 23 (14.5%) and 19 women (11.9%), respectively, and BMI ≥30.0 kg/m2 in only 3 women (1.9%).
Women with as compared with without MetS had a higher prevalence of CKD using eGFRaver whereas no significant difference was found in prevalence of CKD with either eGFRcreat or eGFRcys between the two groups of women (Table 1). There was no significant difference in serum concentrations of creatinine and cystatin C, and three estimates of GFR. By definition, BMI, fasting glucose, and triglycerides were higher and HDL cholesterol was lower in women with MetS than in those without MetS. However, there was no difference in systolic and diastolic BP levels, and the percentage of women with hypertension (63% and 83%, respectively, P = 0.09) between women with and without MetS. Log alanine-aminotransferase, log gamma-glutamyltransferase, HbA1c, log fasting insulin and log HOMA-IR were higher in women with than those without MetS.
Data presented as mean ± standard devition or n, %.
ALT, alanine-aminotransferase; AST, asparate-aminotransferase; BMI, body mass index; BP, blood pressure; eGFR, estimated glomerular filtration rate; eGFRcreat, creatinine-based eGFR; eGFRcys, cystatin-C based eGFR; eGFRaver, average of eGFRcreat and eGFRcys; GGT, gamma-glutamyltransferase; HOMA-IR, homeostasis-model insulin resistance.
The number of participants with 0, 1, 2, 3, 4, and 5 components were 21 (13.2%), 80 (50.3%), 40 (25.2%), 16 (10.1%), 1 (0.6%), and 1 (0.6%), respectively. As the number of components of MetS increased (Fig. 1), the prevalence of CKD using eGFRaver increased from 4.8% in women without MetS component to 31.3% in those with 3 components of MetS. Both of the women with 4 or 5 components had CKD. As compared with women without component, the mean of eGFRaver decreased to the same extent among three groups of women with 1–3 components of MetS (Fig. 1). Therefore, differences in eGFRaver among the six groups were not significant (P = 0.138) when using Jonckheeree-Terpstra test. However, differences among 6 groups were highly significant when analysis of variance was applied (P = 0.009). Analysis of variance excluding 2 participants with 4 and 5 components showed no difference in eGFRaver among 4 groups with 0–3 components (P = 0.115), demonstrating no association between the number of MetS components and eGFRaver values. There was no difference in the prevalence of CKD using eGFRcreat and mean eGFRcreat among the six groups (Table 2). As the number of components of MetS increased, fat mass index, fasting glucose and insulin, and HOMA-IR increased. HbA1c and serum cystatin C were higher in women with 2 or more components than women with 1 or fewer MetS component (Table 2). Women with 1 or more MetS component had higher systolic and diastolic BP as compared with women who had none of MetS components. Elevated BP was found in 89%, 85%, and 94% of women with 1 component, 2 components, and those with MetS, respectively, and 75%, 73%, and 83%, respectively, had hypertension.
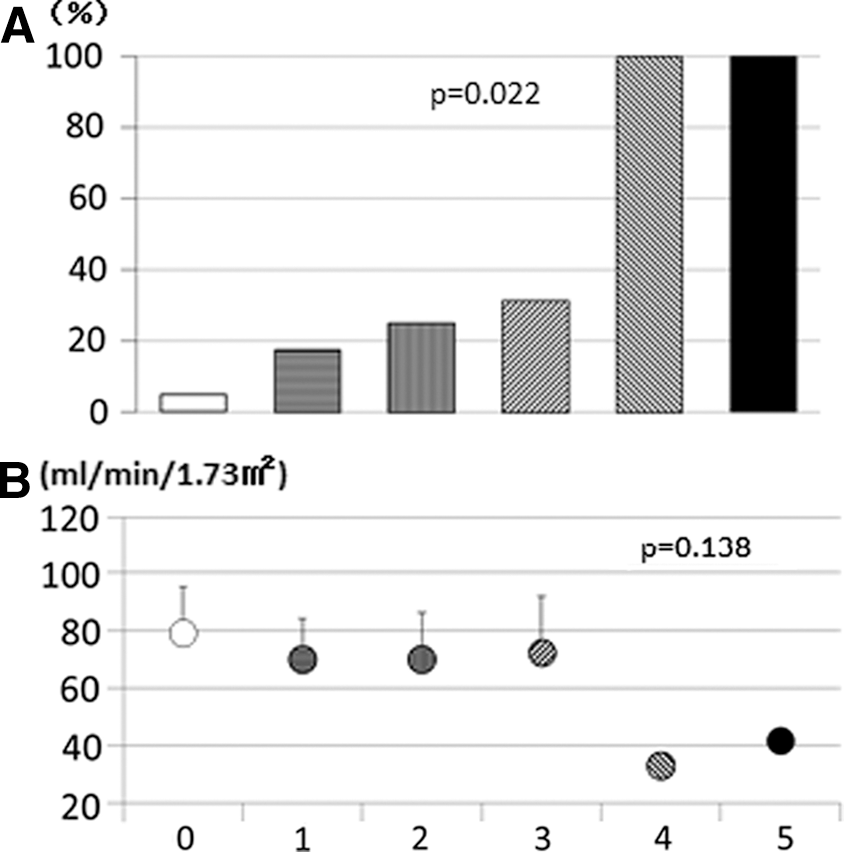
The prevalence of chronic kidney disease
Data presented as mean ± standard deviation or n, %.
Discussion
Prevalence of CKD varied substantially depending on the used equation in community-living, ambulatory Japanese elderly women; 46.5% of CKD prevalence using eGFRcreat was much higher than 12.6% of prevalence using eGFRcys. Both the presence of MetS and the number of MetS components were associated with the higher prevalence of CKD even in elderly Japanese women, who have the highest life expectancy in the world. 29 However, this was evident only when CKD was assessed by the average of eGFRcreat and eGFRcys. We confirmed graded relations between the number of clinical traits of MetS and the prevalence of CKD. It is noted that these findings were observed in community-living ambulatory elderly women in whom 65.4% had hypertension and only 7.5% had diabetes.
CKD prevalence was substantially higher when using eGFRcreat as compared with eGFRcys in Japanese elderly women. It is consistent with results from studies conducted in elderly Western individuals 31 –33 and has been a consistent feature in a systematic review. 34 In the present study, associations of the presence of MetS and the number of MetS components with the higher prevalence of CKD were found only when CKD was diagnosed using eGFRaver. These findings may be in line with the observation that hypertension was significantly associated with CKD progression using the combined cystatin C and creatinine equation but not using the creatinine equation in the Multi-Ethnic Study of Atherosclerosis. 35
The present study confirmed results of meta-analysis using 11 prospective observational studies in middle-aged people 36 and extended that both the presence of MetS and the number of MetS components were associated with the higher prevalence of CKD even in elderly Japanese women. Lower eGFR and higher CKD prevalence were evident in 80 women with only one MetS component, of whom 71 (88.8%) women had elevated BP; 60 had hypertension and 11 had high-normal BP, defined as systolic/diastolic BP of 130–139/85–89 mmHg. High-normal blood pressure has recently been reported to be an independent predictor of impaired renal function, defined as eGFR <60 mL/min/1.73 m2, in a population-based cohort of 1307 subjects free of diabetes, cardiovascular and renal disease. 37 Failure to detect significant association between the presence of MetS and the mean of average eGFR in the present study may be due to the small number of women with MetS. Failure to detect significant association between the number of MetS components and the mean of average eGFR may be due in part to the predominance of elevated BP over metabolic components (IFG, obesity, and dyslipidemia). Approximately 90% of women with one or more components had elevated BP.
Our study has several limitations. We are unable to determine either the direction of association or the causal pathway given the cross-sectional design of our study. The recruitment procedure may also have had an effect on the results. As participation was voluntary, women who pay more attention to their health may have been more likely to participate. Biochemical parameters, including cystatin levels, were measured only once. Although 43, 9, and 58 women (27.0%, 5.7%, and 36.5%, respectively) reported to be receiving statins, antidiabetic drugs, and antihypertensive drugs, respectively, detailed drug information was not available. These drugs may have substantial effects on serum cystatin C levels. 38 –40 In addition, a more direct measurement of GFR, such as inulin clearance, was not used in this study as a gold standard for comparison. We also lacked measures of urine albumin excretion. Finally, BMI in lieu of waist circumference was used for defining MetS, and participants were relatively small in number and were all females.
In conclusion, the present studies have demonstrated associations of the presence of MetS and the number of MetS components with higher prevalence of CKD in nonobese elderly Japanese women and suggest that elevated blood pressure may play an important role in these associations. These findings should be confirmed in studies employing more participants with MetS diagnosed using standard criteria (waist circumference instead of BMI).
Footnotes
Acknowledgments
We are indebted to all the participants for their dedicated and conscientious collaboration.
This study was supported by KAKENHI (21300260) of a Grant-in-Aid for Scientific Research (B) from Japan Society for the Promotion of Science.
Author Disclosure Statement
No competing financial interests exist.