
Abstract
Background:
Interleukin (IL)-18 in synergy with IL-12 is critical in the initiation and progression of Th-1-type responses. IL-18 and IL12 elevation has been associated with atherosclerosis, and their interaction is hypothesized to partly be driven by glucose. We aimed to explore if simultaneous elevation of IL-18 and IL-12, as related to glucose levels, would influence the prognosis in coronary artery disease (CAD).
Method:
Patients (n = 1001) with angiographically verified stable CAD were investigated (78% men, mean age 62 years, 20% current smokers). IL-18 and IL-12 were measured by conventional ELISA methods. High fasting glucose (FG) was defined as the 75 percentile, that is, >6.2 mmol/L.
Results:
After 2-year follow-up, 100 cardiovascular endpoints (fatal and nonfatal acute myocardial infarction, unstable angina, and stroke) were recorded. Subjects with simultaneous (not separate) levels in upper tertiles of both markers were at higher risk of cardiovascular events, compared to subjects in lowest tertile of both (odds ratio = 1.70, 95% confidence interval 1.11–2.61, adjusted P = 0.016), with no influence of high FG. Hyperglycemia associated with higher IL-18 levels (adjusted P = 0.009) and IL-12 levels was considerably lower in current smokers (adjusted P < 0.001).
Conclusion:
Simultaneous elevated circulating levels of IL-18 and IL-12 increased the event rate after 2 years in CAD patients, independent of hyperglycemia.
Introduction
T
IL-18 is produced as an inactive precursor of 24 kDa and is processed by Caspase-1 into the biologically active protein of 18 kDa. 6 IL-18s' intracellular signaling through its heterodimeric IL-18 receptor is partly dependent upon the presence of IL-12. 7
IL-12 is a heterodimeric cytokine composed of two different disulfide-linked peptides, p35 and p40. 8 P40 is involved in IL-12 receptor binding, and p35 is necessary for signal transduction. The two subunits have to be synthesized and dimerized into the biologically active IL-12p70 protein within the same cell.
Previous studies have reported elevated circulating levels of IL-12 and IL-18 in type 2 diabetes mellitus (T2DM) and in metabolic syndrome (MetS). 9,10 Levels of fasting glucose (FG) were shown to be the only MetS component that independently associated with the expression of IL-18 in adipose tissue, 11 indicating glucose to be the driver of the link between IL-18 and MetS. IL-18 and FG levels also showed synergistic effects in cardiovascular risk prediction. 12 In T2DM patients, the production of IL-12 was also observed to be increased in lipopolysaccharide-stimulated peripheral blood mononuclear cells (PBMCs) treated with glucose. 13 Both markers are involved in the pathogenesis of atherosclerosis, 14 and the IL-18/IL-12 synergy has been reported to promote inflammatory responses in the lung. 15
IL-18 has been associated with acute coronary syndrome and worse outcome in patients with coronary artery disease (CAD), 16,17 whereas limited data exist on IL-12 and the combined elevated levels of IL-12 and IL-18 in atherosclerosis and CAD, although IL-12 has been associated with arterial stiffness in healthy individuals. 14
We have previously reported on the association between IL-18 and future clinical events in patients with stable CAD. 18 We aimed in the present study to explore the importance of simultaneously elevated levels of IL-18 and IL-12 for the prognosis in stable CAD patients. We hypothesized that a potential synergy between the markers would increase the risk of new cardiovascular (CV) events, especially in the presence of hyperglycemia.
Materials and Methods
Study population
The present observational investigation is a substudy of the ASCET trial,
19,20
in which 1001 patients with angiographically verified CAD were included in the time period from 2003 to 2008 (97% Caucasians, 78% men, 20% current smokers, mean age 62 years). A flow diagram shows the enrollment of patients to the main study and number of clinical endpoints (Fig. 1). Smoking habits were recorded as current smokers or not, and ex-smokers were included as nonsmokers if they had quit smoking ≥3 months ago. Patients were followed for a minimum of 2 years and the primary endpoint was the first event of fatal and nonfatal acute myocardial infarction (AMI), unstable angina pectoris, ischemic stroke, or death. Evaluation of endpoints was performed by an endpoint committee without access to the laboratory data. The study was performed according to the Declaration of Helsinki and approved by The Regional Committee of Medical Research Ethics in South-Eastern Norway. All subjects provided their written informed consent to participate. The ASCET study is registered at the Website;
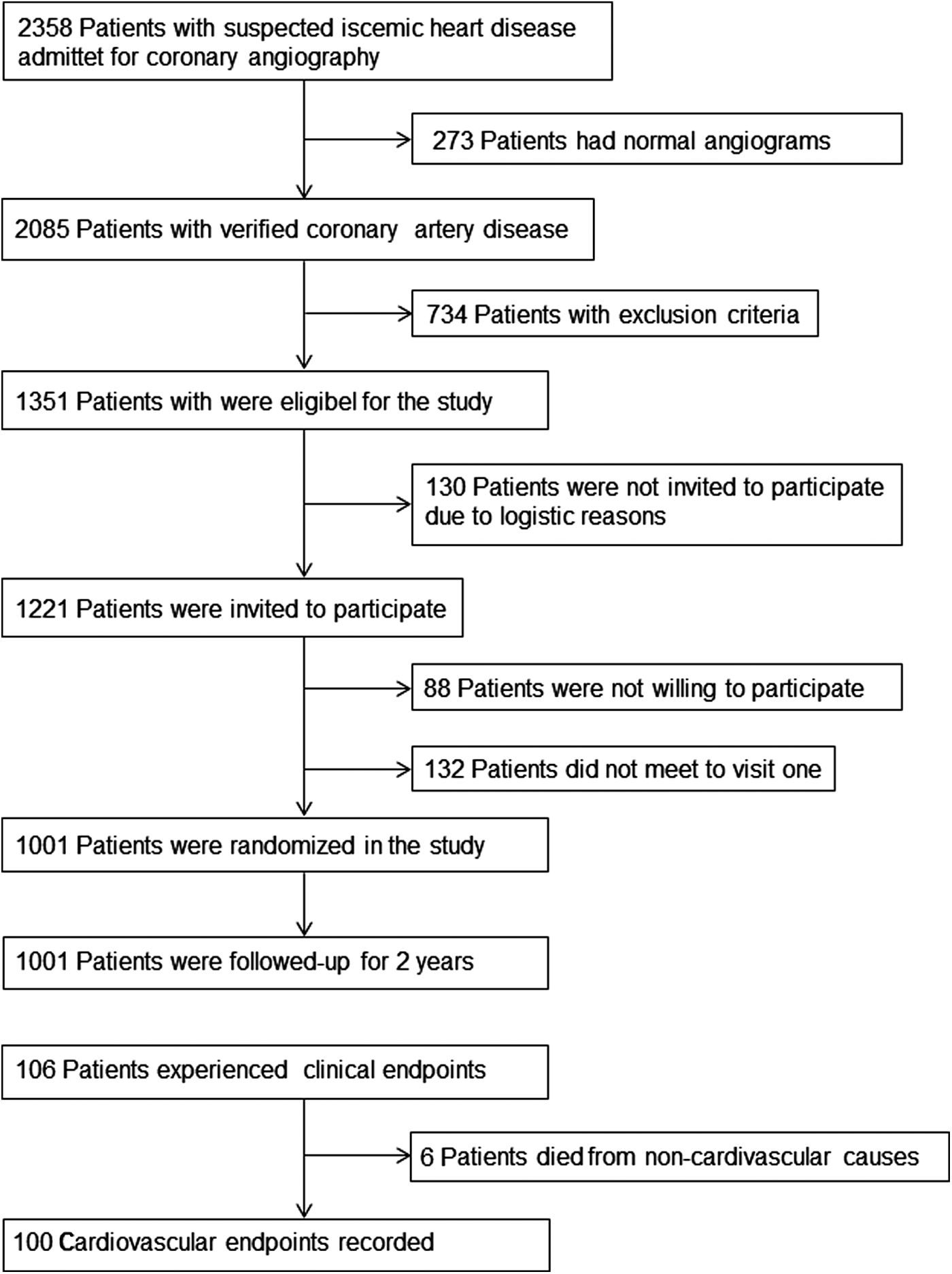
Flow diagram showing enrollment of patients to the main study and number of clinical endpoints.
Laboratory methods
In fasting condition, between 8.00 and 10.00 a.m., blood samples were collected at entrance into the ASCET study. Routine analyses were performed by conventional methods. Serum was prepared by centrifugation within 1 hr at 2.500g for 10 min and kept frozen at −80°C until analysis of the actual markers. IL-18 and IL-12 were analyzed by the following methods: Human IL-18, Medical Biological Laboratories, Naka-ku Nagoya, Japan, and Human IL-12 p40/p70 (Invitrogen), respectively, the latter measuring both the heterodimer (p70) and single p40 subunits of IL-12. Coefficients of variation for the analysis were 8.1% and 4.1%, respectively.
Statistics
For demographic variables, proportions or mean values [standard deviation (SD)] are given. Other variables are given as mean (SD) or medians (25 and 75 percentiles) as indicated. For group comparisons, independent t-test, Mann–Whitney, and Kruskal–Wallis tests, when appropriate, were used for continuous data. The chi-squared test was used for comparison of categorical data. The association between circulating markers and clinical events was analyzed by linear regression and skewed data were log transformed before entered in the model. Due to low number of new CV events, circulating levels of the main variables were divided into tertiles, and analyses of trends through tertiles of variables were performed with the chi-squared linear-by-linear test for identification of cutoff levels. Logistic regression models were performed to analyze for the associations between clinical events and categorized markers. The multivariate regression models were adjusted for age, gender, current smoking, and previous MI (relevant covariate as described in Table 1). The cutoff level for FG levels was set to the 75 percentile (6.2 mmol/L) to define hyperglycemia. Spearman's rho was used in the correlation analysis. All statistical analyses were performed by SPSS 21.0 (SPSS, Inc., Chicago, IL). A two-tailed probability test of 0.05 or less was considered statistically significant.
Values are mean (SD) or number (proportions) if not otherwise stated. P-values are chi-squared test for categorical variables and t-test and Mann–Whitney test for continuous variables, referring to differences between patients with and without endpoints.
Median levels (25, 75 percentiles).
Figure in bold shows statistical significance.
ACE, angiotensin converting enzyme; ARB, angiotensin receptor blocker; BMI, body mass index; CCB, calcium channel blocker; CV, cardiovascular; FG, fasting glucose; HDL, high-density lipoprotein; LDL, low-density lipoprotein; SD, standard deviation.
Results
After 2 years, 106 clinical events were recorded; AMI (n = 36), UAP (n = 33), stroke (n = 28), and deaths (n = 9). Six patients died from noncardiovascular causes and were excluded from data analysis in the present investigation (Fig. 1). At a 2-year follow-up, minimal changes were observed in clinical characteristics, including lipid values and FG levels. No changes in the frequencies of hypertension and current smokers were recorded, whereas 13 patients had developed T2DM at the final visit, however, equally distributed according to occurrence of new clinical events. Characteristics of the population according to occurrence of CV endpoints (n = 100) are presented in Table 1, showing statistical differences in the presence of previous MI.
Levels of IL-12 and IL-18 as related to CV events and hyperglycemia
Levels of IL-12 were not associated with CV events and were not differently distributed according to T2DM and MetS (data not shown). However, we observed considerable lower IL-12 levels in current smokers, compared to nonsmokers as follows: 56.8 pg/mL [95% confidence interval (CI) 37.5–88.4] vs. 96.6 pg/mL (95% CI 66.1–141.9), P < 0.0001 both in univariate analysis and when adjusted for age, gender, and previous MI. Smoking was therefore additionally adjusted for in the regression analyses.
To analyze for simultaneously elevated levels of IL-18 and IL-12 for the prognosis in stable CAD patients, circulating IL-18 and IL-12 levels were divided into tertiles (Ts); (IL-18: T1 ≤ 212.5, T2 > 212.5–293.1, T3 ≥ 293.1 and IL-12: T1 ≤ 68.2, T2 > 68.2–115.2, T3 ≥ 115.2, all pg/mL; Fig. 2A). The categorized markers were further dichotomized between T1 and T2/3, due to IL-12 profile through Ts, and analyzed according to number and percentages of CV events. Subjects simultaneously in upper Ts of both markers were at higher risk of CV events (P = 0.017 univariate model) with an adjusted odds ratio (OR) of 1.70, 95% CI 1.11–2.61 (P = 0.016), compared to the lowest T of both (Fig. 2B). Analyzed separately, the upper Ts (T2/T3) of IL-18 and IL-12, compared to T1, were not associated with CV events (P = 0.10 and P > 0.2, respectively; Fig. 2B).

Ts of IL-18 and IL-12 as related to number of CV endpoints. White bars; T1, gray bars; T2, black bars T3
To explore the influence of hyperglycemia on circulating IL-18 and IL-12, levels of FG were dichotomized at the 75 percentile and further analyzed in groups of low (≤6.2 mmol/L) and high (>6.2 mmol/L) FG. In the total population (n = 1001), 238 patients presented with high FG. FG levels per se were not differently distributed, as related to events. IL-18 levels were significantly elevated in patients with high versus low FG (Table 2) and in patients suffering CV events, compared to patients without CV events, however, only at low FG (univariate model P = 0.025, P = 0.030 adjusted; Fig. 3A). No significant associations were observed for IL-12, as related to FG levels or new CV events (Table 2 and Fig. 3B, respectively). In the tertile analyses, the association between risk of CV events and combined elevated IL-18 and IL-12 levels increased in patients with low FG (univariate model P = 0.010) with an adjusted OR of 1.90, 95% CI 1.15–3.15 (P = 0.012) (Fig. 2C), however, abolished in patients with hyperglycemia.
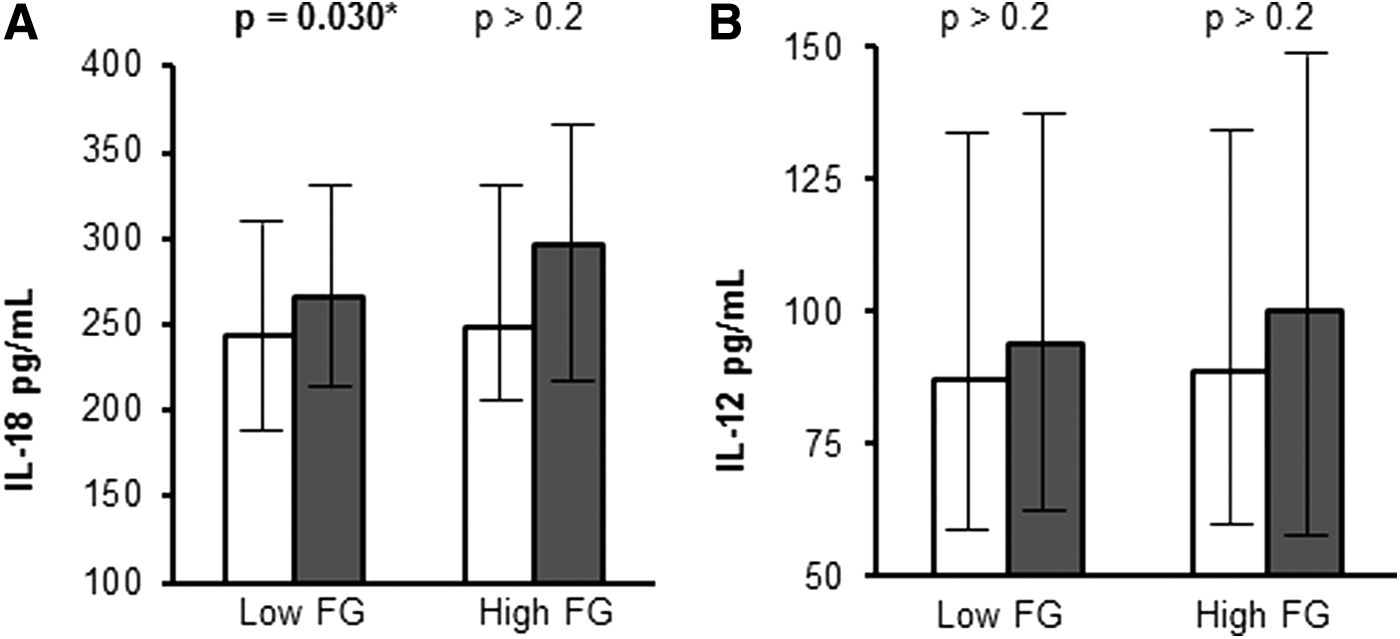
Circulating IL-18
Low FG ≤6.2, high FG >6.2 pg/mL.
Adjusted for current smoking, age, gender, and previous myocardial infarction. Figure in bold shows statistical significance.
IL, interleukin.
Correlation analysis
Circulating IL-18 and IL-12 were weakly, but significantly correlated (r = 0.18, P < 0.001), however, stronger correlated in subjects suffering new CV events and in patients presenting with hyperglycemia (r = 0.28, P < 0.01, both), and in the presence of T2DM (r = 0.30, P < 0.001). Glucose levels were only weakly correlated to IL-18 (r = 0.10, P = 0.001), whereas no correlation to IL-12 was observed (P > 0.2).
Discussion
Combined elevated levels of IL-18 and IL-12 were significantly associated with worse prognosis in CAD, and we observed that patients in simultaneously upper tertiles of both markers presented with higher risk of CV events. In patients suffering a new clinical event, the correlation between IL-18 and IL-12 was strengthened. As both markers induce IFN-γ, the downstream effects and the importance of their synergy should be considered, as a stronger proinflammatory Th1 response might be expected. Recently, it was reported an increased Th1 and suppressed Th2 response, measured by serum cytokine levels, in patients with diabetic CAD. 21 Furthermore, the production of IL-18, IL-12, and IFN-γ by different immune cells was reported to contribute to atherosclerotic plaque progression. 22 Moderate to low FG, rather than hyperglycemia, increased the synergistic effect of the markers, as related to CV events in the present study. This could be due to the low number of events in the hyperglycemia group and Type II statistical error, or that the importance of the markers' circulating levels is masked by other risk-conferring factors present in hyperglycemia. In addition, the optimal treatment of diabetic individuals and the moderate FG levels of defined hyperglycemia might also explain the lack of association in this subgroup.
Hyperglycemia per se has been associated with endothelial dysfunction and elevation of proinflammatory cytokines, chemokines, and proatherogenic mediators. 23 We observed significantly elevated levels of IL-18 in patients with high FG. The interaction between IL-18, glucose levels, and CV events has previously been reported. 12 Circulating levels of IL-18 were also significantly elevated in our population in subjects suffering new events, as previously reported. 18 However, in contrast to our hypothesis, when analyzed in subgroups of low and high FG, the association was only significant with low FG, which could be discussed by the aforementioned assumptions. IL-12 levels were not significantly influenced by glucose levels and were not higher in patients with T2DM and in patients suffering new CV events in the present investigation. In contrast, IL-12 serum concentrations have been reported to be elevated in a limited number of patients with T2DM, compared to CAD patients and healthy controls, and also in newly diagnosed T2DM. 9,24 Furthermore, in vitro studies showed upregulation of IL-12 in PBMCs isolated from healthy subjects and in mouse macrophages treated with glucose. 25,26 The discrepancy between these in vitro studies and our in vivo observation may reflect the source for IL-12 production in specific cell research versus cumulated secretion from all possible cell types included in the measured IL-12 serum levels. As we observed numerical elevation of IL-12 levels as related to clinical events, other factors rather than hyperglycemia might be involved in its elevation. Aspirin treatment has been reported to decrease IL-12 production, 27 which could have masked an eventual IL-12 elevation in patients with high FG in our study. As all patients were on aspirin treatment at baseline in the present trial, this has not been corrected for.
The observed pronounced reduction in circulating IL-12 levels in current smokers has to our knowledge not previously been reported, although described in bronchoalveolar lavage, 28 in gingival crevicular fluid in patients with periodontitis, 29 and further in in vitro studies. 30 The observed reduced IL-12 levels in current smokers fit with reported impaired immunity in airways of cigarette smokers. 31,32 As cigarette smoking associates with progression of atherosclerosis, it is unlikely that the observed attenuated circulating IL-12 levels modify this process.
The low number of CV events in our study limits the results, and power calculation was primarily designed for the main ASCET study. 19 Thus, further subgroup analysis has not been performed concerning the presence of T2DM and MetS in relation to new CV events. Our observation should therefore preferentially be further explored.
In conclusion, hyperglycemia seemed not to influence the synergy between IL-18 and IL-12, however, their interaction associated with worse prognosis in our CAD population. These results may add information on the interplay between these important proinflammatory markers, which may have an impact on novel therapeutic strategies.
Footnotes
Acknowledgments
The authors thank medical laboratory technologists Vibeke Bratseth and Sissel Åkra for blood sampling handling in the ASCET trial.
Funding
The Norwegian Council for Cardiovascular Diseases (main study) and Stein Erik Hagen Foundation for Clinical Heart Research, Oslo, Norway (present study). These funding sources were not involved in the research and preparation of the article.
Author Disclosure Statement
No competing financial interests exist.