
Abstract
Background:
Asian Indians have markedly increased mortality due to coronary artery disease (CAD). Impaired endothelial function has been linked to an increased risk of acute cardiovascular events. We tested the hypothesis that endothelial function was attenuated in Asian Indians and Caucasians.
Methods:
We studied 14 Asian Indians [mean age: 30 ± 6 years; mean body mass index (BMI): 25 ± 3 kg/m2] and 11 Caucasians (mean age: 30 ± 5 years; mean BMI: 26 ± 2 kg/m2). All 25 subjects were healthy men and nonsmokers without any history of CAD or diabetes and were not taking medications. Endothelial function was evaluated by ultrasound measures of flow-mediated dilatation (FMD) and endothelium-independent nonflow mediated vasodilatation (NFMD) of the brachial artery, in the morning immediately after awakening (6 a.m.) in a fasting state.
Results:
Mean age, BMI, apnea–hypopnea index, heart rate, and blood pressure were similar in both groups (P = >0.05). When correcting for body surface area, brachial artery diameter was not different between the two groups (2.1% ± 0.3% vs. 2.2% ± 0.4%; P = 0.29). FMD and NFMD were similar in Asian Indians and Caucasians (5.9% ± 4.1% vs. 5.7% ± 2.6%, P = 0.70; 16.4% ± 8% vs. 14.8% ± 4.1%, P = 0.58, respectively).
Conclusion:
Endothelial function in Asian Indian men is not attenuated in comparison to Caucasian men.
Introduction
A
Endothelial dysfunction is considered an early marker of atherosclerosis and has been linked to cardiovascular events. 12 –17 There are limited data on endothelial function measures in Asian Indians despite their increased CAD burden. 18,19 A recent study demonstrated that Asian Indian patients with erectile dysfunction had a higher prevalence of severe and diffuse angiographic CAD and lower mean brachial artery flow-mediated dilatation (FMD). 20 However, these vascular function measures may reflect existing structural vascular damage. We sought to compare endothelial function in healthy Asian Indian versus Caucasian males to determine whether there is any functional discrepancy between the two groups.
Materials and Methods
The study was approved by the Institutional Review Board at Mayo Clinic, Rochester. Study participants signed an informed written consent to participate.
We studied 14 Asian Indians, mean age: 30 ± 6 years; mean body mass index (BMI): 25 ± 3 kg/m2, and 11 Caucasians, mean age: 30 ± 5 years and mean BMI: 26 ± 2 kg/m2. All 25 subjects were healthy men and nonsmokers without any history of CAD or diabetes mellitus and were not taking medications. All participants were instructed to abstain from alcohol and caffeine for 24 hr before the study.
Polysomnography
To exclude potential confounding effects of obstructive sleep apnea (OSA) on our studies of endothelial function, all subjects underwent attended overnight comprehensive polysomnography (PSG) at the Clinical Research Unit (CRU) for evaluation of sleep disordered breathing and to obtain objective evidence of adequate sleep efficiency. The PSG monitoring system (Compumedics E-Series; Compumedics, Abbotsford, VIC, Australia) included standard physiologic parameters, such as electroencephalography, electro-oculography, electromyography, electrocardiography, and thermistor, and transduced nasal pressure and oral airflow measurements. Respiratory measures of chest and abdominal movements were recorded using respiratory inductance plethysmography. Oxygen saturation was recorded using pulse oximetry. All studies were manually scored by an experienced registered PSG technologist. The disordered breathing events were scored in accordance with guidelines from the American Academy of Sleep Medicine (AASM) standards. 21 Apnea–hypopnea index (AHI) measures the frequency of obstructive events, both apneas and hypopneas. An AHI of greater than five events an hour suggests the presence of OSA.
Measurements of endothelial function
Ultrasound measurements of FMD and endothelium-independent nonflow medicated vasodilatation (NFMD) of the brachial artery were obtained to evaluate endothelial function. 22,23 To minimize any diurnal effects, effects of food intake, or other variability on function, all measurements were obtained during the early morning at 6 a.m. after awakening, and while in a fasting state.
Using the Acuson Ultrasound machine (Acuson Computed Sonography) with a 6 MHz linear transducer, images of the right brachial artery in the longitudinal plane above the antecubital fossa were obtained. The artery was scanned at the exact same location in each subject. Timing of diastole was determined with the use of continuous ECG recording. Before each measure, we ensured that subjects were rested and supine for 10 min. FMD was induced by inflating the forearm cuff to 50 mmHg over the systolic blood pressure or to 200 mmHg for 5 min, which was then released. About 1 to 1.5 min after deflation of the cuff, the arterial diameter was assessed. A second image of the artery was obtained after a 10-min recovery period. NFMD was induced by a sublingual dose of nitroglycerin tablet (0.4 mg). Imaging of the brachial artery was obtained continuously for 4 min.
Diameter measurements
Brachial artery diameter was measured at the onset of the R wave. A total of five measurements were obtained from three cardiac cycles and the average value was measured. All studies were performed by experienced investigators. While investigators who acquired the images could not be blinded, investigators who conducted the off-line analysis of the images were blinded to group ethnicity. These individuals analyzed the measurements manually offline, with an intraobserver reproducibility of 95% and interobserver reproducibility of 93%.
Statistical analysis
Data are summarized as mean ± standard deviation (SD) for continuous variables. The percent changes in brachial artery FMD were compared using the Kruskal–Wallis test. Data were analyzed using JMP version 7 (SAS Institute, Inc., Cary, NC). Two-tailed P-values <0.05 were considered statistically significant.
Results
The baseline characteristics, age, BMI, waist-to-hip ratio, percentage body fat, and systolic and diastolic blood pressures, were similar between Asian Indian and Caucasian men (Table 1), as were brachial artery diameter and brachial artery diameter index (Table 2). No subject was found to meet diagnostic criteria for a sleep-related disorder. The mean AHI in the Asian Indians was similar to that observed in the Caucasians (1.2 ± 1.4 vs. 0.6 ± 0.8 events/hr, respectively, P = 0.31).
AHI, apnea–hypopnea index; BMI, body mass index; DBP, diastolic blood pressure; HR, heart rate; SBP, systolic blood pressure.
The percent changes of brachial artery diameter during FMD and NFMD were similar in both groups (Figs. 1 and 2).
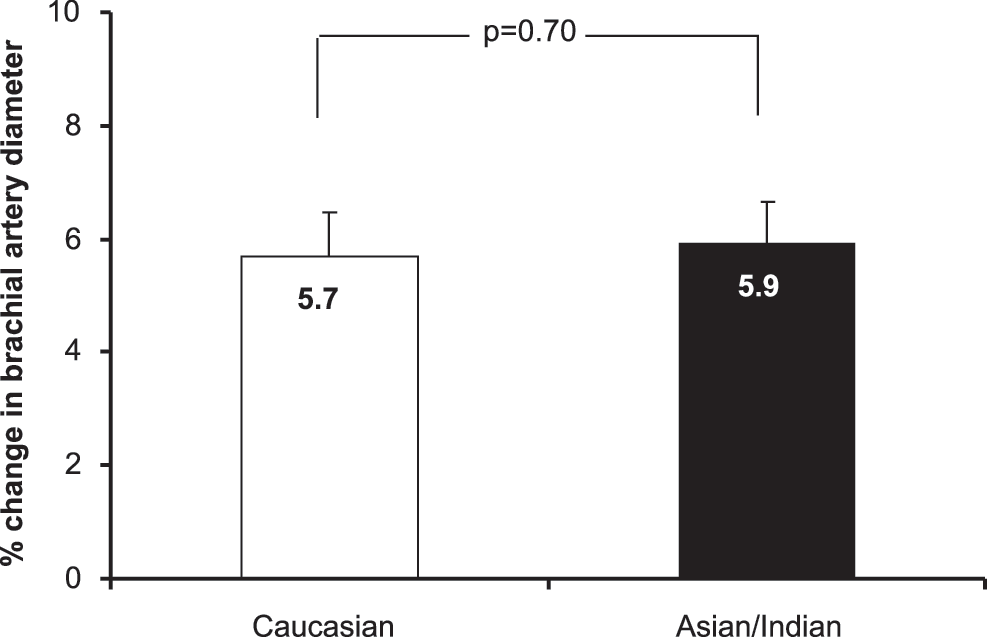
Flow-mediated vasodilatation in Caucasian versus Asian Indian men.
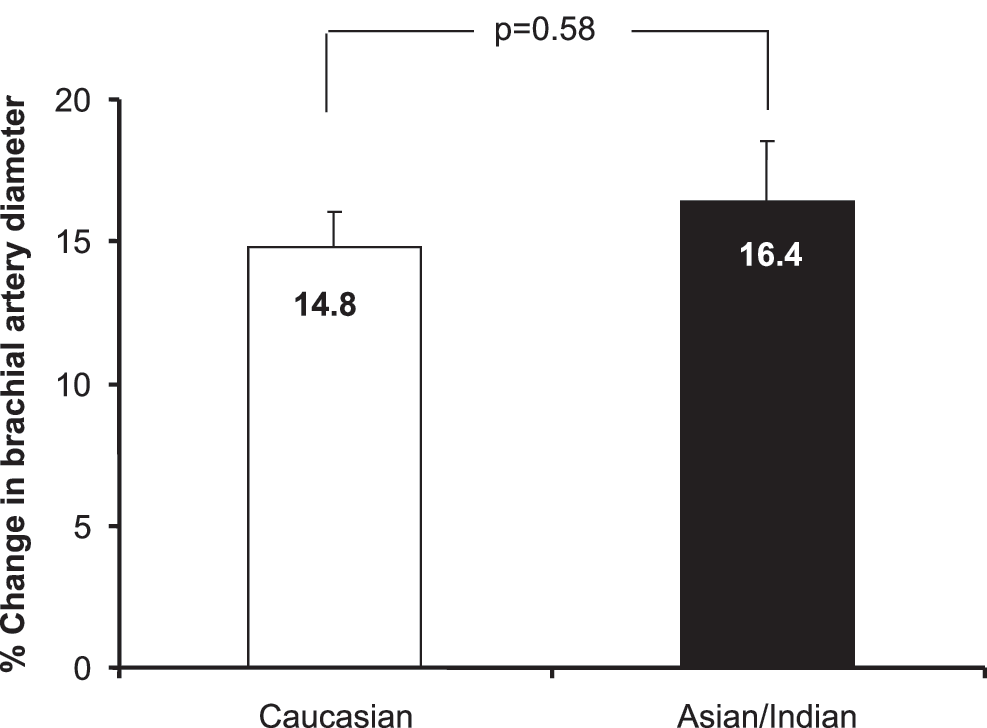
Nonflow mediated dilatation in Caucasian versus Asian Indian men.
Discussion
In this study, measurements were taken in the early morning in a fasting state after overnight PSG so as to avoid any “influence” of diurnal variation or food intake on endothelial function. Despite several previous reports that endothelial function is reduced in Asian Indians in comparison to Caucasians, we observed no differences between our two matched groups. 18,19,24 To our knowledge, this is the first study to suggest that endothelial function is not reduced in Asian Indian men, a group that is at significantly increased CAD risk.
Our findings are not in agreement with prior studies that demonstrated endothelial dysfunction in an Asian Indian population. For instance, Chambers et al. (1999) reported impairment of endothelial function in healthy Asian Indians living in the United Kingdom in comparison to Caucasians. Unlike the group of Asian Indians included in our study, the Chamber's cohort resided in the United Kingdom for a mean of 27 years, which would allow further lifestyle adaptation. In addition, they had a greater waist-to-hip ratio, a marker of central obesity that may have contributed to the endothelial dysfunction. These results were confirmed by Murphy et al., in a population of South Asian men living in the United Kingdom. 25 This study also reported reduced number and function of endothelial progenitor cells in South Asian men. Reduced endothelial progenitor cells (EPCs) have been found in patients with established CAD and are suggested as predictive of future cardiovascular events. 25 It has also been shown that cutaneous endothelial function is reduced in Asian Indians compared to Caucasians. 19 The cohort from India in this study had been in the United States for 6 months, and it is plausible that these findings may reflect effects of diet and lifestyle in India and that differences in endothelial function may not be present in Asian Indians living in the United States for an extended period.
Therefore, potential explanations for the differences in our findings versus earlier studies include first that in our sample of Asian Indian men, all had resided in the United States for at least 2 years. Diet and lifestyle directly influence endothelial function. 26 –30 Over these 2 years, the Asian Indian men's diet and lifestyle would be more comparable to that of the Caucasian control subjects. In addition, the Asian Indian men could have started exercising while in the United States, which could influence endothelial function. Second, we studied healthy subjects, free of any known disease and no medications. Thus, we excluded any potential confounding influences of co-morbidities, such as CAD, on our measurements of endothelial function. In addition, to the best of our knowledge, our study is the first to include an overnight PSG. Since OSA is highly prevalent in Asian Indian men, and since OSA is an important cause of endothelial dysfunction, undiagnosed sleep apnea may be an important contributor to any findings of endothelial dysfunction. 31 –33 Since previous studies did not include an overnight PSG evaluation, we cannot be certain that the differences in endothelial function that were reported may in fact reflect the presence of sleep apnea.
Third, several groups have previously documented smaller vessel size in Asian Indian men using quantitative angiography. 34 –37 Using ultrasound measures, we show a small brachial artery diameter in Asian males. However, when we corrected for body surface area, Asian Indian men's brachial artery diameter was not different than that in Caucasian men.
The present study has several limitations. We studied only healthy relatively young Asian Indian and Caucasian men living in the upper Midwest United States. Due to the small sample size and specific location, we cannot generalize our findings given the mixed genetic pool in the Asian subcontinent. For instance, a prior study reported impaired endothelial function in Sikhs living in the west of London. 18 Furthermore, our results cannot be extended to elderly individuals or patients with CVD or women. Finally, we did not assess inflammation biomarkers and coagulation factors, so we cannot exclude the possibility that the Asian Indians may have an early stage of endothelial dysfunction that could not be detected by the standard FMD technique.
In conclusion, in the absence of co-morbid cardiac or metabolic disease or sleep apnea, endothelial function in young healthy Asian Indian men was not different than in closely matched Caucasian men. Therefore, impaired endothelial function is not in and of itself a likely contributor to the increased cardiovascular risk in Asian Indian males.
Future Directions
Future studies that include elderly individuals, women, and patients with cardiovascular disease may be helpful to obtain better insight into the increased risk of cardiovascular events in Asian Indians. In addition, lifestyle factors, such as diet and exercise, as well as inflammatory biomarkers and coagulation factors, should be assessed to better understand the pathophysiological mechanisms that may play a role in the development of cardiovascular disease in this patient population.
Funding Support
This study was supported by NIH grant HL-65176 and also by UL1 TR000135 from the National Center for Advancing Translational Sciences (NCATS). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
Contributions of Authors
The authors contributed significantly to the study and take full responsibility for the integrity and accuracy of the data. All authors have revised the article critically and agreed to the article as written.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.