
Abstract
Background:
Metabolic syndrome is increasingly common in U.S. adolescents and has been linked to cognitive dysfunction. Purpose of this study is to explore associations between metabolic syndrome and cognitive impairment in U.S. adolescents using population-based data.
Study Design:
Participants included adolescents aged 12–16 years who participated in the National Health and Nutrition Examination Survey (NHANES) III. The main outcome measures included assessments of cognitive function using Wide Range Achievement Test-Revised (WRAT-R) and Wechsler Intelligence Scale for Children-Revised (WISC-R) tools. The WRAT-R consisted of mathematics and reading tests. The WISC-R consisted of block design test, which measures spatial visualization and motor skills, and digit span test, which measures working memory and attention. Linear regression models were used to examine associations between metabolic syndrome and cognitive function. We used education levels of the family reference person, while controlling for education levels because of missing data.
Results:
Presence or absence of metabolic syndrome was tested in 1170 of 2216 NHANES III participants aged 12–16 years. Regression models showed that participants with metabolic syndrome scored an average 1.25 [95% confidence interval (CI) = −2.14 to −0.36] points lower in reading examination and an average 0.89 (95% CI = −1.65 to −0.13) points lower in digit span examination, compared to those without metabolic syndrome. In addition, components of metabolic syndrome—elevated systolic blood pressure and increased waist circumference (WC)—were associated with impaired working memory/attention, and higher fasting glucose and increased WC were associated with poorer reading test scores.
Conclusions:
Metabolic syndrome was associated with impaired reading, working memory, and attention among adolescents.
Introduction
M
In the late 1980s, Reaven 6 proposed the name “Syndrome X” for the cluster of pathophysiological findings, including hypertension, dyslipidemia, and impaired glucose control that often precede cardiovascular disease (CVD) and type 2 diabetes mellitus (T2DM), and hypothesized that it may be a risk factor for these conditions. This hypothesis was modified by others who established that insulin resistance is the key pathological finding in Syndrome X and hence coined the term “insulin resistance syndrome.” 7 “Metabolic syndrome” was used by the World Heart Organization, the International Diabetes Federation, and the National Cholesterol Education Program Third Adult Treatment Panel to identify patients at increased risk for CVD and T2DM. It includes the cluster of five risk factors—high blood pressure, increased waist circumference (WC), decreased high-density lipoprotein cholesterol (HDL-C), increased triglycerides (TG), and hyperglycemia. 8
Many studies have associated metabolic syndrome with Alzheimer's disease, vascular dementia, depression, and other neuropsychiatric disorders in the elderly population. 9 However, to our knowledge, only one study researched the relationships between metabolic syndrome and functional and structural central nervous system impairment in adolescents. 10 In addition, large-scale population-based studies exploring associations between metabolic syndrome and cognitive impairments in children and adolescents are lacking. Therefore, this study explored associations between metabolic syndrome and cognitive impairments in the U.S. adolescent population.
Methods
Survey design
The National Center for Health Statistics, Centers for Disease Control and Prevention, periodically administers the National Health and Nutrition Examination Survey (NHANES) to collect nationwide population-based statistics about the health and nutritional status of the noninstitutionalized civilian population in United States. The NHANES collects data through household interviews, standardized physical examinations, and laboratory analyses of blood samples collected by specialized mobile examination centers. The third NHANES (NHANES III) conducted between 1988 and 1994 surveyed 33,994 participants aged 2 months and older from 89 randomly selected locations in United States. NHANES III followed a complex, stratified, multistage, probability sample design to ensure that the population from which data were collected reflected the general U.S. population characteristics after weighing for age, sex, level of education, and race/ethnicity. NHANES III was the last such survey to include cognitive testing. All the protocols for conducting NHANES III were approved by the Institutional Review Board of the National Center for Health Statistics, Centers for Disease Control and Prevention.
Study population
Of the 33,994 participants, 2216 were adolescents aged 12–16 years; 1940 of these were assessed for cognitive impairment using the Wide Range Achievement Test-Revised (WRAT-R), the Wechsler Intelligence Scale for Children-Revised (WISC-R), or both. Presence or absence of metabolic syndrome was tested in 1170 of these participants. This analysis was confined to those 1170 participants (Fig. 1).
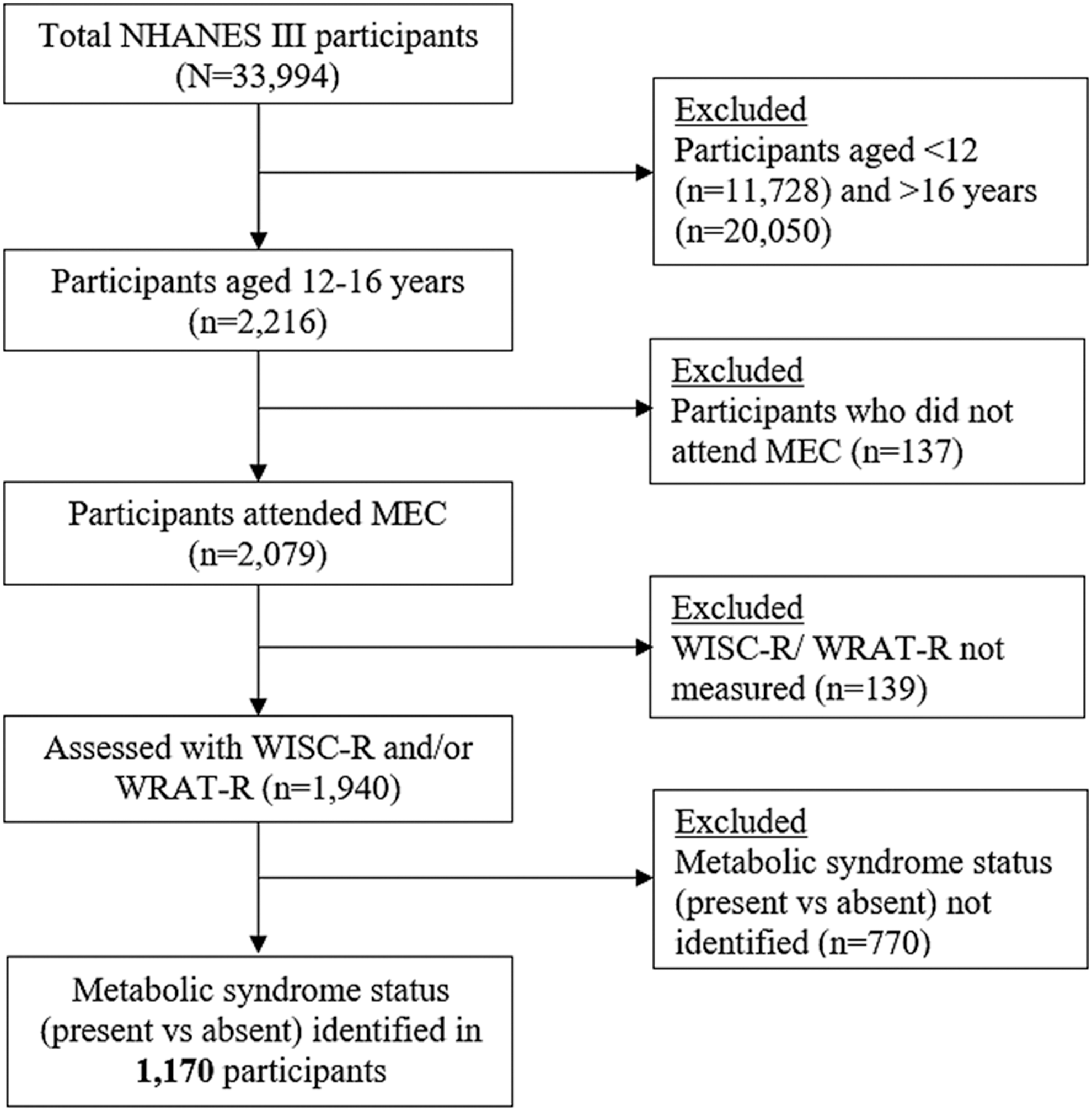
Derivation of the analysis sample.
Metabolic syndrome measurements
Family history, medical history, prescription medications, and other clinical information were obtained from reference persons during household interviews. Participants were assigned randomly to morning, afternoon, or evening sessions at the mobile examination centers. Participants assigned to morning sessions were asked to fast for 8 hrs, and those assigned to afternoon and evening sessions for 6 hrs. Procedures for determining fasting TG, HDL-C, and glucose levels have been described previously. 11 Blood pressure was measured on three occasions during the examinations. The means of the second and third measurements were used in our analyses. Height was determined using a stadiometer, and weight was measured using a self-adjusting scale (Mettler-Toledo, Inc., Columbus, OH). The WC measurements were made during minimal respiration to the nearest 0.1 cm using a nonstretchable tape at the midpoint between the bottom of the rib cage and the top of iliac crest.
Metabolic syndrome definition
Criteria for defining adolescents as having metabolic syndrome were based on cutoffs recommended by de Ferranti et al. 12 and included the following: HDL-C <50 mg/dL, except in boys aged 15–19 years, in whom the cutoff point was <45 mg/dL; WC >75th percentile for sex and age; systolic blood pressure (SBP) >90th percentile for sex, age, and height; TG ≥100 mg/dL; and fasting glucose ≥110 mg/dL. Participants were considered to meet the case definition for metabolic syndrome if they met three or more of the criteria above. This adolescent definition was similar to the Adult Treatment Panel III metabolic syndrome definition for U.S. populations. 12
Laboratory analyses
Serum TGs were measured enzymatically after hydrolyzation to glycerol (Hitachi 704 Analyzer; Hitachi, Tokyo, Japan). HDL-C was measured using a Hitachi 737 Analyzer (Boehringer-Mannheim Diagnostics, Indianapolis, IN). Fasting serum glucose concentration was measured using an enzymatic reaction (Cobas Mira assay; Roche, Basel, Switzerland). The interassay coefficient of variation was less than 4% for all the 6 years of the survey. 13
Cognitive function measures
Cognitive function in adolescent participants was measured using WRAT-R and WISC-R. The WRAT-R consisted of a mathematics and a reading test. 14 The mathematics test assessed the ability to perform mathematical calculations. The reading test assessed recognition, naming, and word pronunciation. Similarly, the WISC-R consisted of two sections that included a block design and a digit span test, 15 which measured perceptional and visuospatial reasoning skills and working memory and attention levels, respectively. All scores were recorded as continuous variables; higher scores in both tests indicated better performance.
Covariates
Covariates controlled in the analyses included age, sex, race/ethnicity, levels of education of family reference person, poverty-income ratio, body mass index (BMI), C-reactive protein (CRP), and environmental tobacco smoke exposure. Age was analyzed as a continuous variable. Sex was self-reported as male or female. Race/ethnicity was self-reported as non-Hispanic white, non-Hispanic black, Mexican American, or others. The family reference person's self-reported educational attainment was recorded as number of years of schooling. For our analysis, we categorized this variable into less than high school, high school graduate, and greater than high school. The poverty–income ratio (ratio of family income divided by the appropriate threshold income based on family size) was categorized into low (0–1.299), middle (1.300–2.999), and high (≥3.000). BMI was calculated in kilograms per meter square and categorized into normal BMI stratum (BMI <85th percentile), at risk for overweight (BMI = 85th–94th percentile), and overweight (BMI ≥95th percentile). 16 CRP was categorized as 0.0–0.3 mg/dL (normal) and >0.3 mg/dL (elevated). Environmental tobacco smoke exposure was reported as yes or no, depending upon the presence or absence of (a) smoker(s) in the household.
Statistical analyses
SAS version 9.4 (SAS Institute, Cary, NC) was used for statistical analysis. Appropriate weights, strata, and clusters were used to account for the complex study design of NHANES III. Descriptive statistics explored characteristics of participants based on the presence or absence of metabolic syndrome. Chi-squared tests and t-tests were used for statistical significance testing for categorical and continues variables. Chi-squared tests were also used to compare cognitive function among participants with and without metabolic syndrome. Mathematics, reading, block design, and digit span scores were compared among the various BMI and CRP categories.
Multiple linear regression models were used to examine associations between metabolic syndrome and its components, and WRAT-R and WISC-R scores. Both crude and adjusted associations were calculated. Covariates were selected based on published studies as well as relevance, and were tested for associations with metabolic syndrome status and cognitive measures using bivariate analyses and subsequently included in the adjusted model. All nonmissing values of the covariates were included for the analysis and P < 0.05 was considered statistically significant.
Results
Characteristics of participants
Weighted prevalence of metabolic syndrome in this sample was 10.4%. The mean age ± standard error (SE) was 14.1 ± 0.06 years; 50.0% of participants were male, 66.8% were non-Hispanic whites, 28.8% were in the lowest poverty–income ratio category, and 25.6% had family educational attainment below high school graduation. NHANES III participants with metabolic syndrome were significantly more likely to be non-Hispanic Whites, to be overweight, and to have higher CRP when compared to those without metabolic syndrome (Table 1).
Weighted to be representative of the U.S. general population.
P < 0.05, compared with Non-MetS.
MetS, metabolic syndrome; SE, standard error; BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic pressure; TC, total cholesterol; TG, triglycerides; HDL, high-density lipoprotein; LDL, low-density lipoprotein; FSG, fasting serum glucose; CRP, C-reactive protein; WRAT-R, Wide Range Achievement Test-Revised; WISC-R, Wechsler Intelligence Scale for Children-Revised.
Cognitive measures
Participants with metabolic syndrome had significantly lower scores in reading and digit span than those without metabolic syndrome (Table 1). There were no significant differences between males and females with respect to mathematics, reading, and digit span scores. However, females scored lower in block design score compared to males.
BMI and cognitive impairment
Overweight participants had significantly lower scores in mathematics, reading, and digit span tests compared to participants in the normal and/or at risk for overweight BMI categories (Table 2). Overweight participants scored significantly lower in mathematics testing, compared to normal weight participants (P = 0.04). Overweight participants also scored significantly lower in the reading test, compared to participants who were normal weight (P < 0.001) and at risk for overweight (P < 0.001). Similarly, overweight participants scored significantly lower in the digit span test, compared to normal weight participants (P = 0.01) and participants at risk for overweight (P = 0.025). Although overweight participants scored lower in block design tests compared to normal weight and at risk for overweight participants, the difference was not statistically significant.
P < 0.05, compared with normal category.
P < 0.05, compared with at risk for overweight category.
CRP and cognitive impairment
Participants with elevated CRP had significantly lower scores in reading tests (mean ± SE = 7.44 ± 0.43) compared to those with normal CRP (mean ± SE = 8.44 ± 0.21, P = 0.043). Participants with elevated CRP had lower scores in mathematics, block design, and digital span tests, but the differences were not statistically significant. Among participants with metabolic syndrome, multivariate adjusted linear regression showed that participants with elevated CRP scored 1.94 [95% confidence interval (CI), −2.95 to −0.94] points lower in digit span test compared to those with normal CRP. Similar associations were not found among participants without metabolic syndrome.
Metabolic syndrome and its components and association with cognitive impairment
Regression models to assess associations between metabolic syndrome and WRAT-R/WISC-R scores showed that participants with metabolic syndrome scored 1.25 (95% CI, −2.14 to −0.36) points lower in reading examination and 0.89 (95% CI, −1.65 to −0.13) points lower in digit span examination than those without metabolic syndrome in models adjusted for covariates (Table 3).
Adjusted for age, sex, race/ethnicity, family education level, poverty-income ratio, and smoke exposure (except for the model for digit span).
P < 0.05.
CI, confidence interval.
Participants with WC >75th percentile for sex and age scored 0.79 (95% CI, −1.43 to −0.15) points lower in reading examination and 0.72 (95% CI, −1.41 to −0.03) points lower in digit span examination, compared to those with WC ≤75th percentile for sex and age in models adjusted for covariates (Table 4). Similarly, participants with SBP >90th percentile for sex, age, and height scored 1.11 (95% CI, −1.79 to −0.43) points lower in digit span examination, compared to those with SBP ≤90th percentile for sex, age, and height in models adjusted for covariates. Participants with fasting glucose ≥110 mg/dL scored 2.91 (95% CI, −5.45 to −0.38) points lower in reading examination, compared to those <110 mg/dL in models adjusted for covariates.
Adjusted for age, sex, race/ethnicity, family education level, poverty–income ratio, smoke exposure (except for the model for Digit Span), and BMI (except for the model for WC).
P < 0.05.
Discussion
To the best of our knowledge, this is the first population-based study to examine the association between metabolic syndrome and cognitive impairment in adolescents in a large representative U.S. sample. We found that metabolic syndrome was associated with impaired reading and working memory/attention scores. Several specific components of metabolic syndrome were also associated with certain cognitive deficits. Elevated SBP was associated with impaired working memory/attention and increased WC was associated with both impaired reading and working memory/attention. In addition, we also found that higher fasting glucose was associated with poorer reading test scores.
It is unclear whether the associations observed in this study indicate that metabolic syndrome contributes to cognitive impairment, although the results of this study are consistent with similar reports of cognitive dysfunction in older patients with metabolic syndrome. 17 Insulin resistance—a documented correlate of metabolic syndrome and reduced glucose tolerance—may be implicated in the association between cognitive impairment and metabolic syndrome. 6,18 In a cross-sectional study among obese adolescents with T2DM, magnetic resonance imaging brain scans showed increased rates of hippocampal and prefrontal cortex atrophy in participants with insulin resistance. 19 This study explored anatomic evidence of cerebral damage, but did not report results of psychometric or cognitive assessments to quantify functional impairment. Our study complements this evidence of morphologic cortical abnormality with data related to cognitive function and supports the hypothesis that the cognitive impairment could be associated with changes in brain parenchyma related to insulin resistance. A study conducted among 53 adolescents with T2DM also reported impaired hypothalamic–pituitary–adrenal axis and other cerebral abnormalities. 20 Such abnormalities were associated with insulin resistance; this study also reported that adolescents with insulin resistance had weakened awakening cortisol response, smaller hippocampal volumes, and increased frontal lobe atrophy compared to those without insulin resistance. These findings implicate insulin resistance in cognitive dysfunction. However, we could not test this hypothesis because NHANES III measured serum insulin levels only in participants aged 20 years and above.
A number of studies have proposed alternative hypotheses that may explain the association we found between cognitive impairment and metabolic syndrome. Neuroinflammation, oxidative stress, abnormal brain lipid metabolism, and impaired vascular reactivity are currently being investigated. 21 Metabolic syndrome has been linked with several vascular factors such as intima-media thickness of carotid arteries, von Willebrand factor, and inflammatory markers like CRP levels among children. 22,23 Studies among older participants supported the link between inflammatory markers and cognitive impairment using cognitive function tests. In a Dutch study of 1183 elderly participants, inflammatory markers like CRP and α1-antichymotrypsin were associated with significant cognitive decline, as measured by Mini-Mental State Examination, Verbal Learning Test, Raven's Colored Progressive Matrices, and Alphabet Coding Task. 24
It has been suggested that the human brain activity increases neurotransmitter levels in activated areas, which in turn regulate the regional cerebral blood flow depending upon the oxygen needs of the tissue. 25 This phenomenon, known as functional hyperemia, is dependent upon a number of endothelial vasodilatory mechanisms 25 and is adversely affected by insulin resistance through impaired signal transduction pathways in endothelial and vascular smooth muscle cells. 26 In an experiment on Zucker Diabetic Fatty rats, insulin resistance impaired such endothelial functions, thereby delimiting the vasodilatory and functional hyperemic mechanisms. 27 A recent review 21 has proposed an integrated model in which insulin resistance, vascular reactivity, and obesity-associated inflammatory markers were grouped together and hypothesized to jointly impair functional hyperemia. This model also proposes that impaired vascular reactivity and impaired functional hyperemia could lead to improper clearance of metabolic waste and impaired metabolic functioning, potentially leading to irreparable damage of cerebral parenchyma. 21 Such damage could result in changes in cognitive performance as seen in this study.
In our study, we found that elevated SBP was associated with impaired working memory/attention scores. In a study 28 in 5077 children aged 6–16 years from the NHANES III population, it was found that children with increased SBP scored lower in the digit span component of WISC-R cognitive test, similar to our findings in older children. Several other studies have linked elevated SBP to neurocognitive impairment. 29 Possible mechanisms explaining these associations include defective cerebral vascular autoregulation, unrecognized lacunar infarcts, or cerebral atrophy and amyloid angiopathy. 30,31
Physical measures of obesity were also found to predict poor cognitive performance in our study. We found that increased WC, often correlated with increased BMI, 32 was associated with impaired reading vocabulary and working memory/attention scores. These findings were similar to the results in other studies that linked BMI in the overweight or obese strata with impaired neurocognitive functions. 33 Alternatively, in a study of 478 patients aged 6–19 years, there were no associations between BMI and cognitive performance in male participants, and lower BMI was associated with poor cognitive function in female participants. 34
Another component of metabolic syndrome, fasting glucose, was significantly associated with poor performance in the reading test. Similar to this finding, in a study of 67 children aged 5–16 years, 35 hyperglycemia was associated with poor scores on the General Information task of the Woodcock-Johnson III test of verbal intelligence. High serum glucose was also associated with hippocampal atrophy. 36 Cognitive impairment seen in hyperglycemia could be due to accumulation of advanced glycation end-products. 37
Certain limitations of this study should be considered when interpreting the results. Since the study is cross-sectional, we could not infer causality in the association between metabolic syndrome and cognitive impairment. In addition, we had to exclude participants with missing data, thus limiting our sample size. Nonetheless, the prevalence of metabolic syndrome in our study was similar to previous studies conducted among adolescents from NHANES III. Although we used the criteria defined by de Ferranti to identify adolescents with metabolic syndrome, other criteria exist for this population. It is possible that using such other criteria could have yielded different results. A major limitation of this study is the use of education levels of the family reference person, while controlling for education levels because of the large number of missing values in the education levels of the participants. Finally, the instruments used to measure cognitive performance should also be considered when interpreting the results. The reading component of WRAT-R measures the cognitive capacity of understanding letters and words, and is often used as a “reading ability” test, but may not directly measure reading comprehension. In this study, it was assumed that the reading component would be an acceptable proxy for reading comprehension; when letter recognition and word reading are affected, reading comprehension skills would likely decline as well.
Conclusions
Recent studies have shown that the prevalence of obesity and metabolic syndrome are very high among U.S. adolescents and in some populations, may be increasing. In this cross-sectional analysis, we found associations between metabolic syndrome, its components, and impaired cognitive performance, which are crucial for success in school and work. These results suggest that control of metabolic syndrome at an early age may reduce cognitive decline and improve cognitive function and quality of life in adulthood. Because metabolic syndrome appears to be reversible, it would be important to explore whether the adverse impact of metabolic syndrome on cognitive performance is reversible with weight loss and reversal of metabolic syndrome and its components.
Footnotes
Author Disclosure Statement
No competing financial interests exist.