
Abstract
Background:
To investigate the association between hyperuricemia and major adverse cardiac events (MACE) in patients with acute myocardial infarction (AMI).
Methods:
Consecutive patients admitted with AMI to the Coronary Care Unit at R. K. Khan Hospital (Durban, South Africa) between the years 2006 and 2014 were included. Demographic data, including clinical and biochemical information stored in an electronic database, were obtained from all patients.
Results:
A total of 2683 patients were studied, of whom 65% were males. The mean age of the participants was 57.1 ± 11.5 years, with 79% presenting with ST elevation myocardial infarction. Sixty-one percent were smokers, 59% had diabetes mellitus, 52% had hypertension, and 58% presented with a family history of premature coronary artery disease. Twenty-six percent (n = 690) had hyperuricemia, were older (59 ± 12.1 vs. 56.5 ± 11.2 years) and more likely to present with hypertension (P < 0.001), lower ejection fraction (P < 0.001), and higher median creatinine levels (P < 0.001). A significantly greater proportion of patients with hyperuricemia experienced MACE (45% vs. 30%, P < 0.001). In both sexes, considerable heterogeneity for risk factors and clinical events was noted in individuals with hyperuricemia. Multivariable analyses for risk factors associated with mortality suggest that hyperuricemia conferred a significantly increased risk of mortality after adjustment [odds ratio (OR) 1.7 (95% confidence interval 1.0–2.8); P = 0.042]. A significant increasing risk trend for MACE was observed for increasing tertiles of serum uric acid concentrations above normal (P < 0.001), particularly for cardiac failure (P < 0.001) and death (P = 0.006).
Conclusions:
Hyperuricemia is significantly associated with hypertension, renal dysfunction, MACE, and independently confers a higher risk of mortality in patients with AMI. Significant heterogeneity was found by gender for risk factors and clinical events in individuals with hyperuricemia. A graded increase was demonstrated in the risk of MACE, particularly for cardiac failure and death, by increasing tertiles of hyperuricemia.
Introduction
C
More recently, several large epidemiological studies have shown that hyperuricemia is associated with an increased incidence of CAD as well as an increased mortality in those with and without pre-existing CAD. 1,2 In humans, uric acid is the end product of purine metabolism due to the nonfunctioning uricase gene leading to elevated serum uric acid levels. 3 Proposed mechanisms for the increased risk in CAD in patients presenting with hyperuricemia include the development of hypertension and oxidative stress, 4,5 endothelial dysfunction, and its strong link with the metabolic syndrome. 6 However, it is unclear if hyperuricemia has a direct causal effect or is simply a marker for other known risk factors of CAD such as hypertension, dyslipidemia, and diabetes. These inconsistent results probably explain why hyperuricemia is currently not listed among conventional cardiovascular risk factors in the guidelines.
Furthermore, data are limited regarding the correlation between hyperuricemia and acute myocardial infarction (AMI), particularly with respect to the relationship of adverse cardiac events and increasing serum uric acid levels. This study therefore was undertaken to determine whether elevated serum uric acid levels are associated with an increased prevalence of major adverse cardiac events (MACE) in patients presenting with AMI in a South African setting.
Methods
This was a single-center study of consecutive patients admitted to the Coronary Care Unit (CCU) at the R. K. Khan Hospital (Durban, South Africa) with a diagnosis of AMI between 2006 and 2014. Patients were excluded if serum uric acid levels were unavailable or if they had unstable angina and gout (n = 162). Patients with gout were excluded because limited information is currently available concerning the impact of urate-lowering treatment on MACE. Furthermore, there is clear evidence of an association between the degree of hyperuricemia and the risk of gout, and these patients were not included in the analysis to eliminate any potential bias. The study was carried out according to the principles of the Declaration of Helsinki and approved by the local ethics committee. A total of 2683 patients were enrolled into the study. AMI was defined by prolonged chest discomfort, typical electrocardiographic changes, and elevated cardiac troponin T (cTnT) levels, as outlined by the Joint European Society of Cardiology/American College of Cardiology Committee. 7
Clinical assessment
Demographic data stored in an electronic database were obtained from all patients. Every patient underwent an initial clinical assessment that included clinical history, physical examination, and 12-lead surface ECG. In addition, anthropometric measurements, including body mass index and waist circumference, were used to define obesity. The central obesity threshold limits proposed by the International Diabetes Federation were used to define visceral obesity. 8 A detailed description of complications encountered during hospital admission, such as ventricular arrhythmias, complete heart block, cardiac failure, cardiogenic shock, recurrence of angina or myocardial infarction, and death, was recorded. Information was also obtained on angiographic results and revascularization procedures such as percutaneous coronary intervention and coronary artery bypass grafting (CABG) that were performed at another referral hospital. Patients who were eligible were thrombolysed with metalyse as a revascularization therapy.
Biochemical analyses
Blood samples for measurements of serum uric acid concentrations and other biochemical measurements were obtained intravenously from all subjects immediately after hospital admission. Analyses were carried out using standard methods. Hyperuricemia was defined as a serum uric acid level ≥0.43 mmol/L (7.22 mg/dL) based on the recommendation of the South African National Health Laboratory Chemistry Expert Group. 9 Furthermore, we subdivided uric acid values ≥0.43 mmol/L into tertiles to assess whether an increasing degree of hyperuricemia was associated with increased risk of MACE. Given the relatively small number of patients above the conventional cutoff for hyperuricemia, tertiles were used to maximize the power and comparison with other covariates to illustrate any relevant response. Total cholesterol, triglycerides (TGs), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C) were measured 48 hrs after admission following a 9–12-hr overnight fast. Troponin T was measured on the Elecsys 2010 (Roche Diagnostics) and the test was considered positive at a cutoff value >0.03 ng/mL. 10
Statistical analyses
Data were processed and analyzed using Stata 13.0 (StataCorp 2013; Stata Statistical Software: Release 13; StataCorp LP, College Station, TX). Continuous variables were summarized using mean and standard deviation or median and interquartile range (IQR) if the data were skewed/asymmetrical. Differences in mean of continuous variables by outcome (i.e., hyperuricemia status) were assessed using Student's t-test. If a variable was not normal, then the Wilcoxon rank sum test result was presented. Association between outcome and categorized explanatory variables/risk factors was assessed using a Pearson chi-squared (χ2) test. If any cell count in the cross-tabulation contained fewer than five expected observations, then Fisher's exact test was employed instead. Bivariate and multivariable-adjusted logistic regression was used to assess the association of explanatory variables (including hyperuricemia) with mortality in the presence of other potential confounders/risk factors. A P value of <0.05 was considered statistically significant.
Results
A total of 2683 patients with AMI were retrospectively studied, of whom 65% were males (Table 1). The mean age of the participants was 57.1 ± 11.5 years with 79% of patients presenting with ST elevation myocardial infarction (STEMI), while 21% had non-ST elevation myocardial infarction (NSTEMI). Overall, 61% of individuals were either previous or current smokers, 59% had a history of diabetes mellitus and hypertension (52%), and 58% presented with a family history of premature CAD. The median serum uric acid levels for the study cohort were 0.4 mM (IQR 0.3–0.4) or 6.72 mg/dL (IQR 5.0–6.7).
HDL-C, high-density lipoprotein cholesterol; IQR, interquartile range; LDL-C, low-density lipoprotein cholesterol; NSTEMI, non-ST elevation myocardial infarction; SD, standard deviation; STEMI, ST elevation myocardial infarction.
Twenty-six percent (n = 690) of patients were found to have hyperuricemia (Table 2). Patients with hyperuricemia were older (59 ± 12.1 vs. 56.5 ± 11.2 years) and were significantly more likely to present with hypertension (62% vs. 49%, P < 0.001), previous myocardial infarction (16% vs. 11%, P = 0.002), lower ejection fraction on echocardiography (51% vs. 54%, P < 0.001), decreased median serum hemoglobin [13.5 grams/dL (IQR 11.7–15.2) vs. 14.1 grams/dL (IQR 12.7–15.3), P = 0.001], median HDL-C values [0.9 mM (IQR 0.8–1.1) vs.1.0 mM (IQR 0.8–1.1), P = 0.002], and higher median creatinine levels [111 μM (IQR 93–148) vs. 88 μM (IQR 75–103), P < 0.001], compared with those with normal serum uric acid.
CABG, coronary artery bypass grafting; PCI, percutaneous coronary intervention.
Analysis of MACE showed that in patients with hyperuricemia, a significantly greater proportion of patients experienced MACE (45%) compared with those with normal levels (30%, P < 0.001). This was particularly evident for cardiac failure (24% vs. 14%, P < 0.001), death (14% vs. 7%, P < 0.001), cardiogenic shock (8% vs. 4%, P < 0.001), ventricular arrhythmias (6% vs. 3%, P = 0.004), complete heart block (4% vs. 2%, P < 0.001), and atrial fibrillation (5% vs. 3%; P = 0.002). Of the1062 patients who had coronary angiograms performed, no correlation was observed between the two study groups with respect to angiographic severity of disease and coronary revascularization.
Risk factors associated with hyperuricemia stratified by gender are reported in Table 3. A significant heterogeneity between genders was noted. In both sexes, hyperuricemia was correlated with increasing age (females, P < 0.001; males, P = 0.002), hypertension (P < 0.001), lower ejection fraction (P < 0.001), reduced median hemoglobin levels (females, P < 0.001; males, P = 0.003), increased median creatinine values (P < 0.001), and MACE (P < 0.001), which included complete heart block (females, P = 0.001; males, P = 0.013), cardiogenic shock (P = 0.001), cardiac failure (P < 0.001), and death (P < 0.001). In males, previous myocardial infarction (P = 0.005), increased median TG (P = 0.005), and atrial fibrillation (P = 0.009) occurred more frequently, while in contrast, low median HDL-C (P = 0.003), recurrence of myocardial infarction (P = 0.018), ventricular arrhythmias (P = 0.013), and CABG (P = 0.028) were found significantly more often in females.
A multivariable analysis for all factors associated with mortality by logistic regression analysis is shown in Fig. 1. In addition to cerebrovascular accident [odds ratio (OR) 5.4, 95% confidence interval (CI) 2.6–11.1; P < 0.001], cardiogenic shock [OR 5.4 (95% CI 3.4–8.4); P < 0.001], ventricular arrhythmias [OR 2.6 (95% CI 1.5–4.5); P < 0.001], cardiac failure [OR 2.4 (95% CI 1.6–3.8); P < 0.001], complete heart block [OR 2.4 (95% CI 1.2–4.8); P = 0.013], recurrence of myocardial infarction [OR 1.9 (95% CI 1.2–3.1); P = 0.008], age ≥65 years [OR 1.9 (95% CI 1.4–2.6); P < 0.001], Killip class ≥2 [OR 1.7 (95% CI 1.0–2.7); P = 0.034], and hyperuricemia also conferred a significant risk of mortality [OR 1.7 (95% CI 1.0–2.8); P = 0.042].
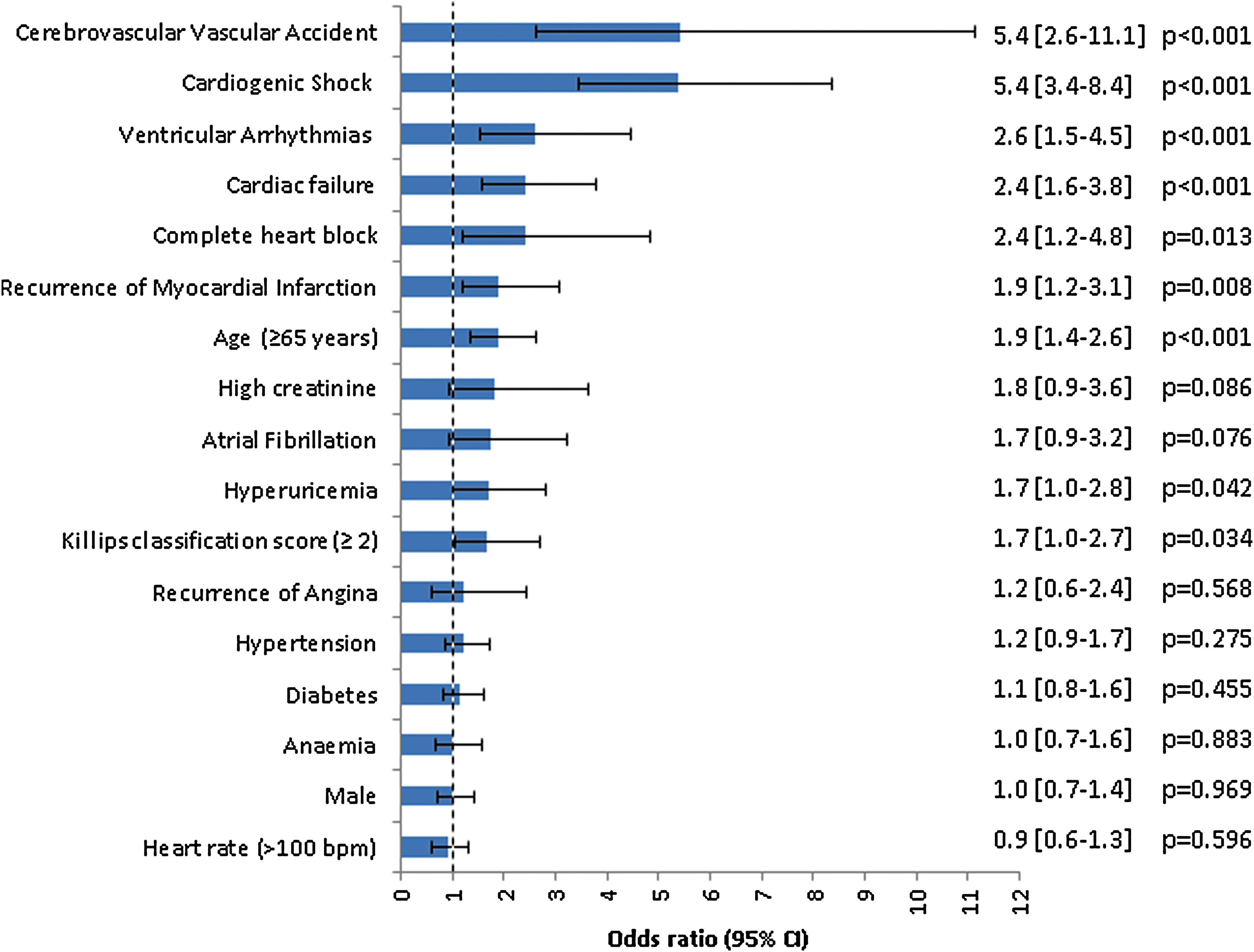
Multivariable logistic regression analysis of clinical and laboratory parameters associated with mortality.
MACE associated with different levels of serum uric acid above normal are presented in Fig. 2. Patients were categorized into three different tertiles (T) of hyperuricemia, T1 [0.43–0.46 mM or 7.22–7.73 mg/dL, n = 245 (9.1%)], T2 [0.47–0.52 mM or 7.90–8.74 mg/dL, n = 231 (8.6%)], and T3 [≥0.53 mM or ≥8.91 mg/dL, n = 214 (8%)]. A significant increasing risk for MACE was shown for increasing tertiles of serum uric acid concentrations above normal T1 [OR 1.4 (95% CI 1.1–1.19); P = 0.017], T2 [OR 1.9 (95% CI 1.4–2.5); P < 0.001], and T3 [OR 2.7 (95% CI 2.0–3.6); P < 0.001], particularly with respect to cardiac failure T1 [OR 1.5 (95% CI 1.0–2.1); P = 0.026], T2 [OR 1.7 (95% CI 1.2–2.4); P = 0.002], and T3 [OR 3.0 (95% CI 2.2–4.2); P < 0.001], and death T1 [OR 1.4 (95% CI 0.9–2.3); P = 0.134], T2 [OR 2.4 (95% CI 1.6–3.6); P < 0.001], and T3 [OR 3.1 (95% CI 2.1–4.5); P < 0.001]. Although a significant risk was observed for ventricular arrhythmias, atrial fibrillation, complete heart block, and cardiogenic shock across all three tertiles of hyperuricemia, a similar increasing risk trend was not evident.
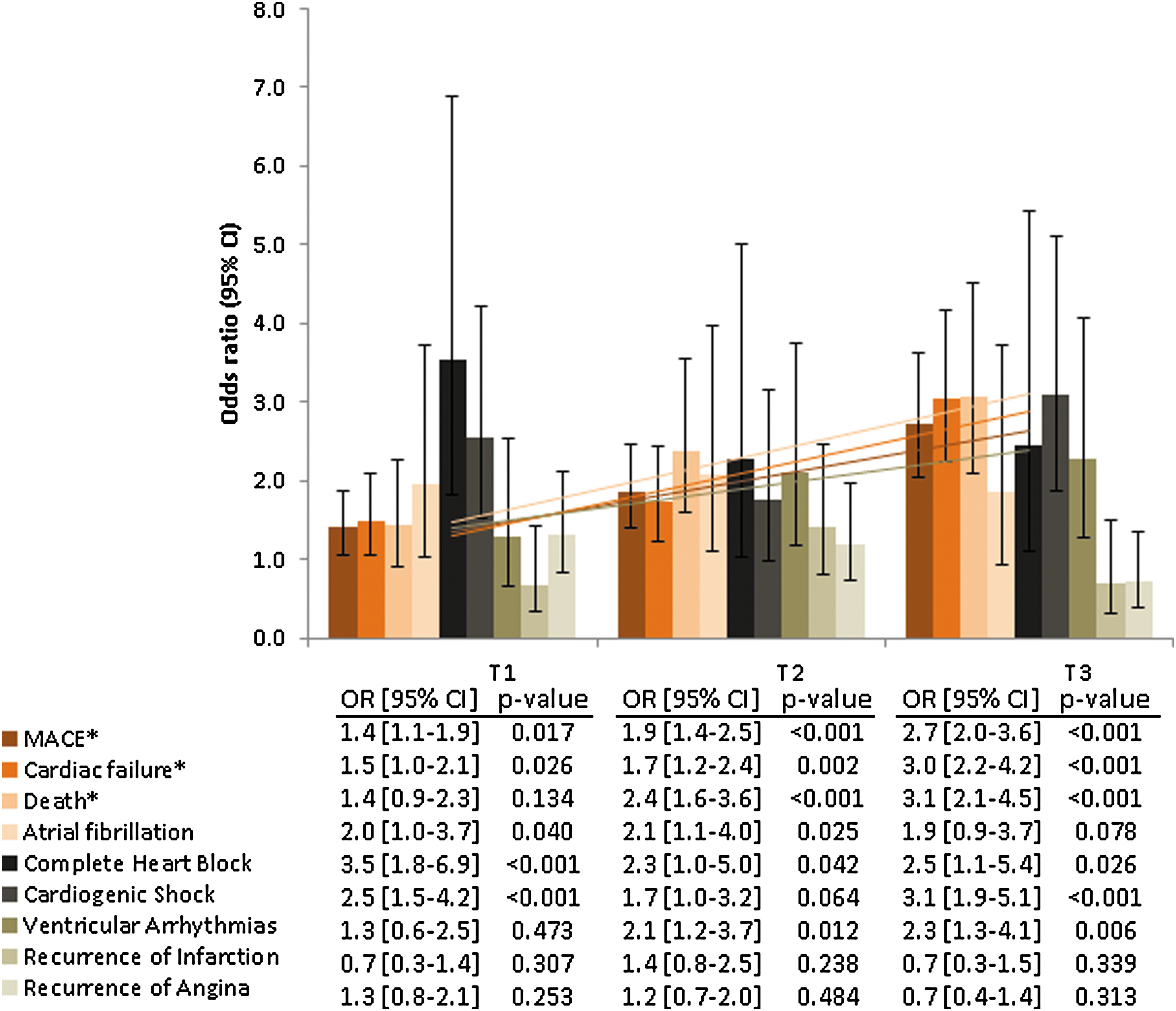
Major adverse cardiovascular events according to specific categories of serum uric acid levels above normal.
Discussion
In this single-center observational study, we examined the association of hyperuricemia and MACE in 2683 patients presenting with AMI. Patients presented at a young age (57.1 ± 11.5 years) and were characterized by the presence of multiple traditional risk factors for AMI.
Twenty-six percent of subjects were found to have hyperuricemia. Of note is that these patients were older and significantly more likely to have hypertension (P < 0.001), lower ejection fraction (P < 0.001), and higher median serum creatinine levels (P < 0.001), compared with those with normal serum uric acid concentrations. Our data are in agreement with previous reports, 11,12 which showed that hyperuricemia is associated with an increased risk of incident hypertension, independent of conventional risk factors. The proposed mechanisms whereby hyperuricemia may induce a rise in blood pressure include renin–angiotensin–aldosterone-dependent arteriolopathy and interstitial fibrosis and glomerulosclerosis with albuminuria. 13,14
A number of cross-sectional studies have demonstrated a link between urate levels and decreased renal function or microalbuminuria, but the interpretation is difficult. 15,16 It has been shown that hyperuricemia accelerates renal progression by inducing systemic and glomerular hypertension, endothelial dysfunction, and progressive renal scarring. 17 Similarly, we also observed a significant interaction between hyperuricemia and elevated serum creatinine levels. These observations, however, still do not resolve the issue of whether hyperuricemia is more a risk factor for the onset of renal disease or its progression.
The findings of the present study showed that a greater proportion of patients with hyperuricemia experienced MACE (45%) compared with those with normal values (30%, P < 0.001). These results concur with previous studies, which reported a significant increase in the risk of coronary events with abnormal serum uric acid levels. 1,18,19 Several potential mechanisms support the role of hyperuricemia as a risk factor for ischemic cardiovascular events. Hyperuricemia contributes to the development of hypertension, 20 increases levels of inflammatory markers, 21 impairs glucose metabolism, 22 and exerts oxidative effects on adipocytes, 23 all of which either independently or in combination contribute to atherosclerosis.
When risk factors and clinical events associated with hyperuricemia were stratified by gender, significant heterogeneity was found between both sexes. However, in males, previous myocardial infarction (P = 0.005), low LDL-C (P = 0.017), increased TGs (P = 0.005), and atrial fibrillation (P = 0.009) occurred more frequently, while low HDL-C (P = 0.003), recurrence of myocardial infarction (P = 0.018), ventricular arrhythmias (P = 0.013), and CABG (P = 0.028) were found significantly more often in females. Although some of these sex differences in our patients with AMI require further research, our data, nevertheless, are consistent with a meta-analysis of 16 observational studies that examined the association between hyperuricemia and CAD. 18 In their subgroup analyses, these authors also found significant heterogeneity in the relative risk for CAD in both men and women presenting with hyperuricemia.
Following multivariable logistic regression analyses of clinical and laboratory parameters associated with mortality, in addition to cerebrovascular accident (P < 0.001), cardiogenic shock (P < 0.001), ventricular arrhythmias (P < 0.001), cardiac failure (P < 0.001), complete heart block (P = 0.013), recurrence of myocardial infarction (P = 0.008), age ≥65 years (P < 0.001), and Killip class ≥2 (P = 0.034), hyperuricemia also conferred a significantly higher risk of mortality (P = 0.042). This study, similar to other publications, also recognized hyperuricemia as a good predictor of death in patients with AMI. 24,25 Yan and Lui Zhang reported in their systematic review of 5686 patients that high uric acid levels were found to be associated with an increased risk of in-hospital mortality in individuals with AMI. 26 They suggested that xanthine oxidase activity and uric acid synthesis increased under myocardial ischemia. What still remains to be confirmed by future research, however, is whether serum uric acid could be an independent predictor of mortality in patients with AMI, similar to cardiac biomarkers such as brain natriuretic peptides and troponins.
More importantly, when we examined the relationship between MACE and different tertiles of serum uric acid concentrations above normal, a significant increasing risk trend was observed for increasing tertiles of hyperuricemia and MACE (P < 0.001). This was particularly evident for cardiac failure (P < 0.001) and death (P = 0.006). Although a significant risk was found for other adverse events, including ventricular arrhythmias, atrial fibrillation, complete heart block, and cardiogenic shock across all three tertiles of hyperuricemia, no similar increasing risk trend was detected. While large epidemiological studies have shown that hyperuricemia is closely associated with an increased incidence of CAD and its complications such as cardiac failure and death, our data suggest that this risk is further increased for patients in the highest tertile of hyperuricemia compared with those in the lowest tertile.
Limitations
Several potential limitations to this study need acknowledgment. This was a single-center retrospective study, but this shortcoming was minimized by using standardized methods for data collection, while the large study population allowed for greater statistical power. Only 1062 patients underwent coronary angiographic studies and therefore these data should be interpreted with caution. This is due to the fact that patients are referred to another hospital with long waiting lists for cardiac catheterization, and a large number of patients declined intervention or did not have coronary angiograms performed because of other co-morbidities.
Conclusions
Our findings affirm that hyperuricemia is significantly associated with hypertension, worsening renal function, MACE, and independently confers a higher risk of mortality in patients with AMI. In addition, significant heterogeneity was found between both sexes for risk factors and clinical events associated with hyperuricemia. Finally, our study demonstrates a graded increase in the risk of MACE, particularly with respect to cardiac failure and death by increasing tertiles of hyperuricemia.
Footnotes
Acknowledgment
The authors thank Ms. S. Ramdas for the typing of the manuscript.
Author Disclosure Statement
No conflicting financial interests exist.