
Abstract
Background:
In contrast to the definition of metabolic syndrome (MetS) in adults, there is no standard definition of MetS in pediatric populations. We aimed at assessing the differences in the prevalence of MetS in children and adolescents aged 9–17 years using four different operational definitions for these age groups and at examining the associated variables.
Methods:
A total of 675 children and 1247 adolescents attending public schools in Bogota (54.4% girls; age range 9–17.9 years) were included. The prevalence of MetS was determined by the definitions provided by the International Diabetes Federation (IDF) and three published studies by Cook et al., de Ferranti et al., and Ford et al. In addition, we further examined the associations between each definition of MetS in the total sample and individual risk factors using binary logistic regression models adjusted for gender, age, pubertal stage, weight status, and inflammation in all participants.
Results:
The prevalence of MetS was 0.3%, 6.3%, 7.8%, and 11.0% according to the definitions by IDF, Cook et al., Ford et al., and de Ferranti et al., respectively. The most prevalent components were low high-density lipoprotein cholesterol and high triglyceride levels, whereas the least prevalent components were higher waist circumference and hyperglycemia. Overall, the prevalence of MetS was higher in obese than in non-obese schoolchildren.
Conclusions:
MetS diagnoses in schoolchildren strongly depend on the definition chosen. These findings may be relevant to health promotion efforts for Colombian youth to develop prospective studies and to define which cut-offs are the best indicators of future morbidity.
Introduction
C
The diagnosis of MetS in children and adolescents depends de facto on the chosen definition, with higher rates of MetS identification when insulin is part of the definition and when child-specific cut-off points for metabolic indicators are used. 6 Ford and Li 7 published a systematic review on 27 publications about MetS in children and adolescents. In these 27 publications, 40 unique definitions of MetS were used, generally following adaptations of the definitions provided by the World Health Organization (WHO), 8 the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III), 9 the European Group for the study of Insulin Resistance (EGIR) 10 adult guidelines, and the International Diabetes Federation (IDF). 11 Other definitions have included more liberal cut-off points, such as the ones proposed by de Ferranti et al., 12 Cook et al., 4 and Ford and Li, 7 as well as other components to evaluate, such as obesity, as in Agudelo et al. 5
Currently, there is no gold standard definition of MetS in children and adolescents; however, a description of the prevalence of MetS according to the few proposed pediatric definitions is necessary for different populations around the world. 13 MetS develops progressively with age according to changes in puberty, and its prevalence increases with obesity. 14 Additionally, in children and adolescents, low-grade systemic inflammation has been shown to be associated with MetS. 15 Because persistently increased inflammation in youth may provide an early warning for later risk of cardiovascular disease, it is important to precisely characterize the relationship between this inflammation, excess weight, and MetS in pediatric populations. However, few studies in low- and middle-income countries 16 have investigated cardiovascular risk factors in youth. 17,18 Such early detection would enable the introduction of targeted interventions that are aimed at reducing cardiometabolic risk in youth and subsequent morbidity. By applying definitions to our preexisting dataset of Latin American youth, we aimed at assessing the differences in prevalence of MetS in adolescents aged 9–17 years in Bogota, Colombia, using four different definitions for this age group and at examining the associated variables.
Materials and Methods
The schoolchildren selected for this study participated in the FUPRECOL study (in Spanish ASOCIACIÓN DE LA
Study population
FUPRECOL study assessments were conducted during the 2014–2015 school year. The sample consisted of children and adolescents (n = 4000 boys and n = 4000 girls) aged 9–17.9 years. In a subgroup of 2775 schoolchildren, parameters of biomarkers were also assessed, and a more comprehensive health and lifestyle assessment was conducted. From this subgroup, 1922 schoolchildren (54.4% girls, n = 675 children and n = 1247 adolescents) had valid data for the anthropometric and blood parameter assessments and were, consequently, included in this study. All schoolchildren were of a low-middle socioeconomic status (SES, 1–3 on the scale of 1–6 defined by the Colombian government) and were enrolled in public elementary and high schools (grades 5 through 11) in the capital district of Bogota, in the Cundinamarca Department in the Andean region. This region is located at ∼4°35′56″N 74°04′51″W and at an elevation of ∼2625 m (min: 2500; max: 3250) above sea level. Bogota is considered an urban area, with ∼7,862,277 inhabitants. 22 Exclusion factors included a clinical diagnosis of cardiovascular disease or diabetes mellitus 1 and 2, pregnancy, use of alcohol or drugs, and not having lived in Bogota for at least 1 school year. Exclusion from the study was made effective a posteriori, without the students being aware of their exclusion to avoid any undesired situations.
Measurement anthropometrics
Anthropometric variables were measured by a Level 2 anthropometrist who was certified by the International Society for the Advancement of Kinanthropometry (ISAK) in accordance with the ISAK guidelines. 23 Variables were collected at the same time in the morning, between 7:00 and 10:00 a.m., after an overnight fast. Subjects’ body weight was measured when they were in underwear and did not have shoes on, using electronic scales (Tanita® BC544) with a low technical error of measurement (TEM = 0.510). Height was measured using a mechanical stadiometer platform (Seca® 274; TEM = 0.019). BMI was calculated as the body weight in kilograms divided by the square of the height in meters. Waist circumference was measured at the midpoint between the last rib and the iliac crest using a tape measure (Ohaus® 8004-MA; TEM = 0.086). Fat mass percentage was estimated using a BC-418 bioimpedance analysis system (Tanita Corp. ; TEM = 0.639). The mean of two readings obtained in the morning was used; the measurements were conducted under controlled temperature and humidity conditions after urination and a 15-min rest, with children shoeless and in fasting condition. The obesity phenotype was determined according to the cut-offs used to define BMI percentiles by the International Obesity Taskforce (IOTF). 24
Resting blood pressure
After the tests and blood draw, diastolic blood pressure (DBP) and systolic blood pressure (SBP) were determined as the average of two measurements separated by a 5-min interval, with the child resting for at least 5 min before the first measurement. Children were seated in a quiet, calm environment with their right arm in a semi-flexed position at heart level. Blood pressure was measured automatically using the Tanita® BC544 (Tanita; TEM = 0.598).
Pubertal stage
Sexual maturation was classified based on Tanner staging, 25 which uses self-reported puberty status to classify participants into five stages (I to V). 26 The volunteers individually entered an isolated room where they categorized the development of their own genitalia (for boys), breasts (for girls), armpits (for boys), and pubic hair (for both genders) using a set of images exemplifying the various stages of sexual maturation. The data were recorded on paper by the FUPRECOL evaluators.
Biochemical assessments
Blood samples were collected between 6:00 and 8:00 a.m. by two experienced pediatric phlebotomists after at least 12 hr of fasting. Before sampling, fasting was confirmed by the child and his or her parents. Blood samples were obtained from an antecubital vein, and analyses were subsequently completed within 1 day of collection. The levels of TG, total cholesterol (TC), cholesterol linked to high-density lipoproteins (HDL-C), and glucose were measured using colorimetric enzymatic methods with a CardioChek analyzer (CC; Polymer Technology Systems, Inc.). The fraction of cholesterol linked to low-density lipoproteins (LDL-C) was calculated using the Friedewald formula. 27 High-sensitivity C-reactive Protein (CrP) was obtained using the turbidimetric method with uikRead 101 (both Orion Diagnostica).
Diagnosis of MetS
The prevalence of MetS and its components were evaluated according to four definitions provided by Cook et al., 4 de Ferranti et al., 12 Ford and Li, 7 and IDF. 11 The IDF defines MetS as the presence of abdominal obesity plus two other components, whereas the other four groups of authors defined it as the presence of three or more components out of five possible components that combine the criteria and cut-off points of the WHO 8 and the National Cholesterol Education Program Adult Treatment Panel III. 9 The characteristics and cut-off points for the diagnosis of MetS are provided in Table 1.
BMI, body mass index; DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; IDF, International Diabetes Federation; MetS, metabolic syndrome; SBP, systolic blood pressure.
Ethics statement
The Review Committee for Research on Human Subjects at the University of Rosario (Code No. CEI-ABN026-000262) approved all of the study procedures. A comprehensive verbal description of the nature and purpose of the study and its experimental risks was provided to the participants and their parents/guardians. This information was also sent to parents/guardians by mail. Written informed consent was obtained from parents and subjects before participation in the study. The protocol was in accordance with the latest revision of the Declaration of Helsinki and current Colombian laws governing clinical research on human subjects (Resolution 008430/1993 Ministry of Health).
Statistical analysis
The results are presented as the mean (standard deviation) or relative frequency as a percentage. Differences between sex and/or pubertal stage were assessed by analysis of variance (ANOVA) with the use of Bonferroni's correction for post hoc multiple comparisons when significant differences were found. The prevalence of MetS was calculated for each definition in the total sample by gender, age, pubertal stage, weight status, and inflammation; the associations between these factors were conducted by the chi-squared test (χ2). Finally, models were considered using definitions of MetS as the dependent variable, and the explanatory variables were individual risk factors. The models were adjusted for gender, age, pubertal stage, weight status, and inflammation. Variable selection for the logistic regression models was also guided by the bivariate analyses. All analyses were conducted using IBM SPSS 21 (SPSS, Inc.). The level of statistical significance was established at P < 0.05.
Results
The descriptive characteristics of the participants are presented in Table 2. The ANOVA analysis showed that girls had higher values of BMI and fat mass than boys, whereas men had higher levels of abdominal obesity. Regarding cardiometabolic risk factors, boys had higher SBP and glucose levels than girls, whereas women showed higher levels of HDL-C, LDL-C, TC, and TG (P < 0.05). Lastly, no significant differences were found between sexes in the TG/HDL-C ratio or CrP levels.
Data are shown in mean (SD). Significant between-sex differences (ANOVA one-way test or χ2).
LDL-C, cholesterol linked to low-density lipoproteins; TC, total cholesterol; TG, triglycerides; CrP, C-reactive protein.
Table 3 describes the study population in terms of the anthropometric variables and prevalence of MetS. The prevalence of MetS was 0.3%, 6.2%, 7.8%, and 11.0% according to the definitions by IDF, Cook et al., Ford et al., and de Ferranti et al., respectively. Few youth fulfilled the five MetS criteria (0.2% using the definitions of Cook et al. and Ford et al.; 0.6% using the definition of de Ferranti et al.; and 0.1% using the definition of IDF). Also, 42.6% (Cook et al.), 30% (de Ferranti et al.), 36.2% (Ford et al.), and 53.4% (IDF) met no criteria at all.
Data are shown in % (n).
Based on gender, in boys, the prevalence of high blood pressure (all definitions), fasting glucose, and low HDL-C levels (all definitions) were significantly higher; whereas high TG levels were more prevalent in girls. Moreover, obese youth had higher prevalence rates in all components by different cut-off points. Lastly, no significant differences were found between pubertal stage-specific cut-off points for MetS components, except in waist circumference (WC) (definition of de Ferranti et al.) and high blood pressure (definitions of Cook et al., Ford et al., and de Ferranti et al.) (Table 4).
Significant difference between groups with the same letter (test χ2).
% (n).
WC, waist circumference.
Finally, Fig. 1 shows the odds ratios (OR) of the relationship between MetS prevalence and individual risk factors (the definition of IDF was not included because of the limited number of subjects who met the criteria). Adjusted analysis suggests that obesity (all definitions) and children aged 9–12 years old (the definition of Ford et al.) were more likely to have prevalence of MetS.
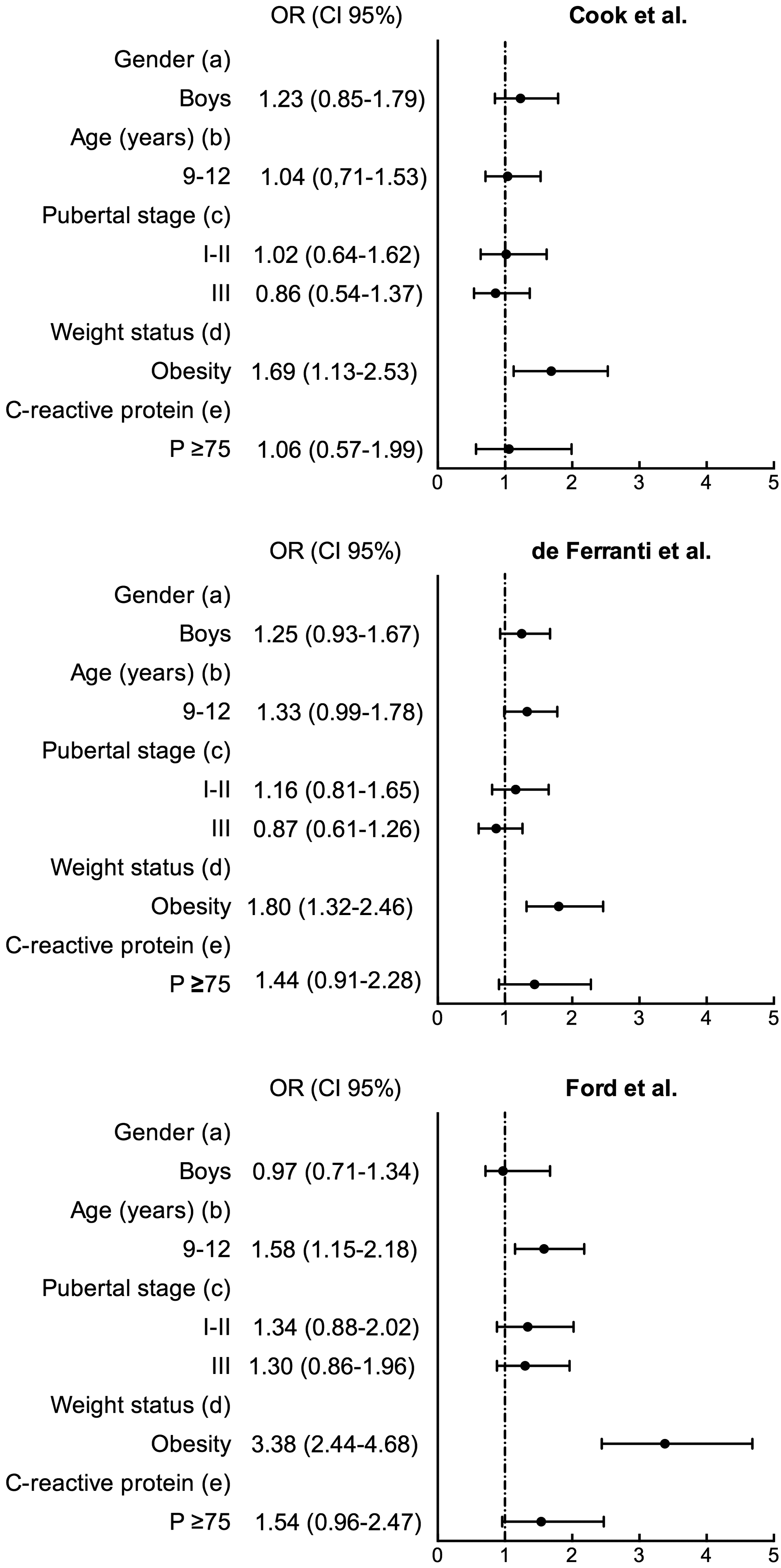
Factors associated with prevalence of metabolic syndrome in Colombian children and adolescents. Reference groups were girls, 13–17 year olds, normal-weight youths, and <75 percentile of C-reactive protein. OR, odds ratios; CI, confidence interval.
Discussion
The use of different definitions has led to significant discrepancies in the overall MetS prevalence in youth and also hinders comparisons across studies. Our study revealed that the prevalence of MetS ranged between 0.3% and 11.4% depending on the definition employed. The most prevalent components were low HDL-C and high TG levels. Additionally, obesity predicted higher prevalence of MetS in all definitions.
Comparing our results with a similar Colombian study on adolescents from Medellin, the prevalence was generally similar, with a slightly higher prevalence in the definitions of Cook et al. (6.2% vs. 3.8% in adolescents from Medellin) and Ford et al. (7.8% vs. 4.1% in adolescents from Medellin). 5 The number of children and adolescents who were diagnosed with MetS was significantly lower according to the definition of IDF, whereas the definitions of de Ferranti et al. 12 and Ford and Li 7 identified the highest prevalence. The IDF criteria use a cut-off that is usually used in adults, which may explain their lower estimate of MetS prevalence. For example, one of the lowest prevalence in our sample was achieved in blood pressure, which uses a cut-off used in adults (SBP ≥130 mmHg or DBP ≥85 mmHg) and does not use cut-off points according to age, sex, and height like the rest of the definitions.
In our population, between 30.0% and 53.4% had none of the five metabolic risk factors. Additionally, confirming the findings of other Latin studies, regardless of the definition used, the most prevalent components of MetS were hypertriglyceridemia and low HDL-C, and the least frequent were hyperglycemia and high WC. 13,28 On the other hand, a study that included Latino adolescents residing in the United States showed a greater prevalence of high waist circumference and low HDL-C, 29 which would suggest that the environmental characteristics of each population may account for the differences between the findings. 30 Also, studies reported that although WC is a good measure of visceral adiposity, it seems less reliable for detecting variations related to puberty and race/ethnicity, 31 and no normative values exist for children and adolescents.
Evidence suggests a higher prevalence of MetS in older children compared with younger children. 32 Our results conflict with most of the prevailing epidemiologic evidence, as children (9–12 years) had a higher prevalence of MetS than adolescents (13–17 years) using the definition of Ford et al. Confirming our results, another study on Mexican youth reported a higher prevalence in the group of individuals aged 7–14 years compared with the prevalence in 15–24 year olds. Additionally, Reinehr et al. 33 found that the relationship between age and MetS was only observed in boys and not girls. The findings of the present study could be due to the group of 9–12 year olds who had a higher prevalence of overweight and obesity (6.3%) than the group of 13–17 years (2.8%).
Published studies have shown that obesity (particularly abdominal obesity) and its related co-morbid conditions are the most predominant correlates of cardiometabolic risk, regardless of the definition used; it is not surprising that the increasing prevalence of MetS is consistent with the dramatic increase in obesity among youths. 32 Our results found that youth with obesity were more likely to have prevalence of MetS compared with their non-obese peers, independent of the definition. These findings confirm studies that suggest that each component of the MetS worsens with increasing obesity in this age group. 34 However, MetS is not simply a consequence of obesity; it should be noted that lean individuals also had at least one risk factor (6.2% to 7.7%). As suggested by Falkner et al., 35 the presence of one metabolic risk factor should prompt screening for additional clinical abnormalities. Therefore, not only the obese population but also the lean young population should be included in policies for early detection and prevention of MetS.
Finally, most studies on youth have not conclusively confirmed that CrP is associated with cardiovascular disease risk factors, 36 especially if corrected for BMI. 37 A study in 403 Chinese children revealed that higher levels of CrP were related with MetS and lipid metabolism, 38 but the relationship weakened when the analysis was adjusted for BMI. In this way, Weiss et al. 34 reported that CrP levels did not correlate significantly with either insulin resistance or the MetS, suggesting that an underlying inflammation may be an additional factor contributing to adverse long-term cardiovascular outcomes in this population. Our findings showed that a higher level of CrP did not predict MetS in any definitions after adjusting for age, gender, pubertal stage, and weight status. Therefore, the present results together with other studies may suggest that inflammation, as assessed by CrP, is not an independent parameter related to MetS.
The present study was limited by the lack of data regarding ethnicity, physical activity, physical fitness, and family history of cardiometabolic disease, which could have enabled more robust adjustments. A second limitation of this study was that it is a cross-sectional design that does not establish evident cause–effect relationships. The third limitation was that no measurements were taken of other components of metabolic health, such as diet (micronutrient and macronutrient intake in particular) and birth weight, which may contribute to cardiometabolic risk factors. The strengths of our study include that it presented a possible first evaluation of a population of schoolchildren and that it used a multivariate analysis to verify independence in the evaluated associations.
In summary, our study suggests that the prevalence of MetS differs depending on the proposed definitions. Additionally, the results showed the importance of obesity as a determinant of pediatric MetS in Colombian youth independent of the pubertal stage and inflammation in all definitions. However, although the prevalence of MetS was higher in obese individuals, it is also necessary to include non-obese peers in policies that target the early detection and prevention of MetS.
Footnotes
Acknowledgment
The FUPRECOL Study was carried out with the financial support of Instituto Colombiano para el Desarrollo de la Ciencia y la Tecnología “Francisco José de Caldas” COLCIENCIAS (contract no. 671-2014 Code 122265743978).
Author Disclosure Statement
No conflicting financial interests exist.