
Abstract
Background:
Metabolic syndrome (MetS) and its components increase the risk of developing cardiovascular diseases, type 2 diabetes, and all-cause mortality. Reports on the trends of MetS and its components in longitudinal studies are scarce, especially in low- and middle-income countries. This study was designed to investigate the prevalence and trends of MetS and its components in a cohort of Iranian adults from 2001 to 2013.
Methods:
Participants were followed up for 12 years in a longitudinal population-based study of 6500 adults aged 35 years and older in 2001. Participants were randomly selected from three provinces in central Iran. Sociodemographic characteristics, anthropometry, blood pressure, and various biochemical indices were collected in 2001, 2007, and 2013. Secular trend and age-adjusted trend of MetS and its components were calculated from 2001 to 2013.
Results:
The standardized prevalence of MetS, hypertension, low high-density lipoprotein cholesterol (HDL-C), abdominal obesity, and diabetes/impaired glucose tolerance (IGT) increased over the 12 years (6.9%, 5.5%, 12.0%, 2.3%, and 18.7%, respectively), while the prevalence of hypertriglyceridemia decreased by 15.5% during this period. The prevalence of MetS, low HDL-C, and abdominal obesity were higher in females than males in all three phases. Moreover, the increases in the prevalence of these metabolic abnormalities were higher in the rural population than in the urban population.
Conclusions:
The present study underscored the increasing trends in MetS and most of its risk factors, thus, to prevent an increase in the cardiovascular risk factors, there is a need to improve lifestyle by education, screening, and treatment of abnormalities.
Introduction
M
Investigating the trend of MetS and its components is important to determine health policies, allocate community and health resources, and to promote measures to reduce trends of increasing prevalence. Most of the previous studies on the prevalence of MetS and its components used cross-sectional data, and limited reports using data extracted from longitudinal studies are available. This study was designed to investigate the trend of MetS prevalence and its components in a cohort of Iranian adults from 2001 to 2013. It also aimed to calculate the prevalence according to gender, age categories, and rural/urban residency.
Materials and Methods
Study design
This study was designed as part of the Isfahan Cohort Study (ICS) that started in 2001 through 2013. ICS is a longitudinal population-based study of 6500 adults 35 years and older at baseline (2001), from three provinces in central Iran. Multistage random sampling was used to select samples, which represent their society's distribution of age, genders, and residential area (urban/rural). More details about the ICS have been published elsewhere. 13 The current study was approved by Isfahan Cardiovascular Research institute (ICRI) and the Griffith University ethics committees.
Measurements
Following fasting blood sampling, blood pressure and anthropometric measurements and physical examinations were carried out. Weight, height, and waist circumference (WC) were measured by trained researchers. Blood pressure was taken twice in a sitting position and the mean value was computed. Global dietary index (GDI) of diet was calculated via questions from consumption of specific food groups, including sweets, hydrogenated oils, animal fats, red meat, fast foods, fruits, and vegetables. Smaller GDI shows better dietary behavior.
Serum triglycerides, total cholesterol (TC), and fasting blood sugar (FBS) were measured using the enzymatic method. 14 Serum HDL-C was determined after separation of very low-density lipoprotein and low-density lipoprotein cholesterol (LDL-C). 15 The Friedewald formula was used to calculate the LDL-C level. 16 All subjects provided informed written consent for their participation. The measurements were repeated in 2007 and 2013 for all participants using the same methods, however, participants were followed every 2 years by phone calls looking for the occurrence of fatal and nonfatal myocardial infarction or stroke or sudden cardiac death. 13
Definitions and criteria
MetS was identified based on the revised version of the ATP III criteria, adjusted by the American Heart Association (AHA) and the National Heart, Lung, and Blood Institute (NHLBI). Based on our previous study, 8 this diagnostic criterion was the best predictor of CVD in the studied population. According to this criterion, having three or more components, as listed below, is required for diagnosing MetS. 17 Impaired glucose: FBS ≥5.6 mmol/L (100 mg/dL) or being on hypoglycemic medication; abdominal obesity: men, WC ≥102 cm and women, WC ≥88 cm; elevated blood pressure: SBP/DBP ≥130/85 mmHg or being on blood pressure treatment; hypertriglyceridemia: triglyceride (TG) ≥1.7 mmol/L (150 mg/dL) or treatment; and low HDL-C: men <1.03 mmol/L (40 mg/dL) women <1.29 mmol/L (50 mg/dL). Combinations of MetS components were considered based on the presence of different components of MetS.
Statistical analysis
The difference of the characteristics between available participants and loss to follow-up individuals was examined by independent sample t-test. Variables are presented as the mean (standard deviation) or percentage. The mean value for each of the individual characteristics between the three phases was compared using generalized estimating equation (GEE). GEE is used for repeated measurements with missing values such as cohort data. 18 Analyses were stratified by gender, age, and residential area categories to consider their effect on the prevalence of MetS and its components. For age, participants were divided into five groups: 35–45, 45–55, 55–65, 65–75, and >75 years based on the age in 2001, 2007, and 2013 phases.
GEE was used to determine trends in the prevalence of MetS and its components from 2001 to 2013. To control the effect of aging on the trends of MetS and its components, age was adjusted in logistic regression, and through the following equation, prevalence was calculated.
19
where P is the probability of MetS or its components, β and βAGE are regression coefficients calculated from the data. Statistical analysis was carried out using SPSS statistical software package version 22 (SPSS, Inc., Chicago, IL).
Results
Available participants and loss to follow-up individuals were comparable in terms of gender (male: 48.6% vs. 48.7%; female: 51.4% vs. 51.3%), age (49.2 years vs. 51.3 years), and MetS (37.4% vs. 35.8%). Characteristics of individuals in 2001, 2007, and 2013 showed that both systolic and diastolic blood pressure significantly increased from 2001 to 2013. The increasing trends were also observed in FBS levels, WC, and BMI. On the contrary, decreasing trends were detected for TC, LDL-C, HDL-C, triglyceride, and physical activity (Table 1).
Data are presented as mean (standard deviation).
P < 0.05 compared with 2001 values.
P < 0.05 compared with 2007 values.
BMI, body mass index; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; WC, waist circumference.
When examining the trend, an upward trend was revealed for an overall prevalence of MetS (15.4% increase) and most of its components, including elevated blood pressure (18.2% increase), low HDL-C (14.4% increase), abdominal obesity (8.1% increase), and diabetes/IGT (26.5% increase), while the prevalence of hypertriglyceridemia decreased from 2001 to 2013 (16.9% decrease). Moreover, it has shown that the prevalence of MetS, elevated blood pressure, hypertriglyceridemia, and diabetes/IGT has been increased in older age groups (except age group >75 years and sometimes age group 65–75 years) in each phase. The prevalence of MetS, low HDL-C, and abdominal obesity was higher in females than males in all three phases, however, no specific patterns were observed in other components of MetS.
The age-standardized prevalence of MetS and its components showed an increasing trend in the prevalence of MetS (6.9% increase), elevated blood pressure (5.5% increase), low HDL-C (12.0% increase), abdominal obesity (2.3% increase), and diabetes/IGT (18.7% increase), but not in hypertriglyceridemia (15.6% decrease) (Fig. 1). These trends were observed, to some extent, in each age category (Fig. 2). The prevalence of MetS, low HDL-C, and abdominal obesity was higher in females than in males in all three phases. When the population was divided based on their residential area, an upward trend was also observed in MetS, elevated blood pressure, low HDL-C, abdominal obesity, and diabetes/IGT for both rural and urban populations. Dietary changes to unhealthy diet were also observed in both populations. However, the increases in the prevalence of these metabolic abnormalities were higher in the rural population compared with the urban population. Moreover, the prevalence of MetS and its components was higher in urban areas in 2001 and lower in 2013 compared with rural areas (Table 2). Overall, of all the components, the prevalence of diabetes/IGT increased the most, followed by low HDL-C.

Age-standardized prevalence of MetS from 2001 to 2013 in female.
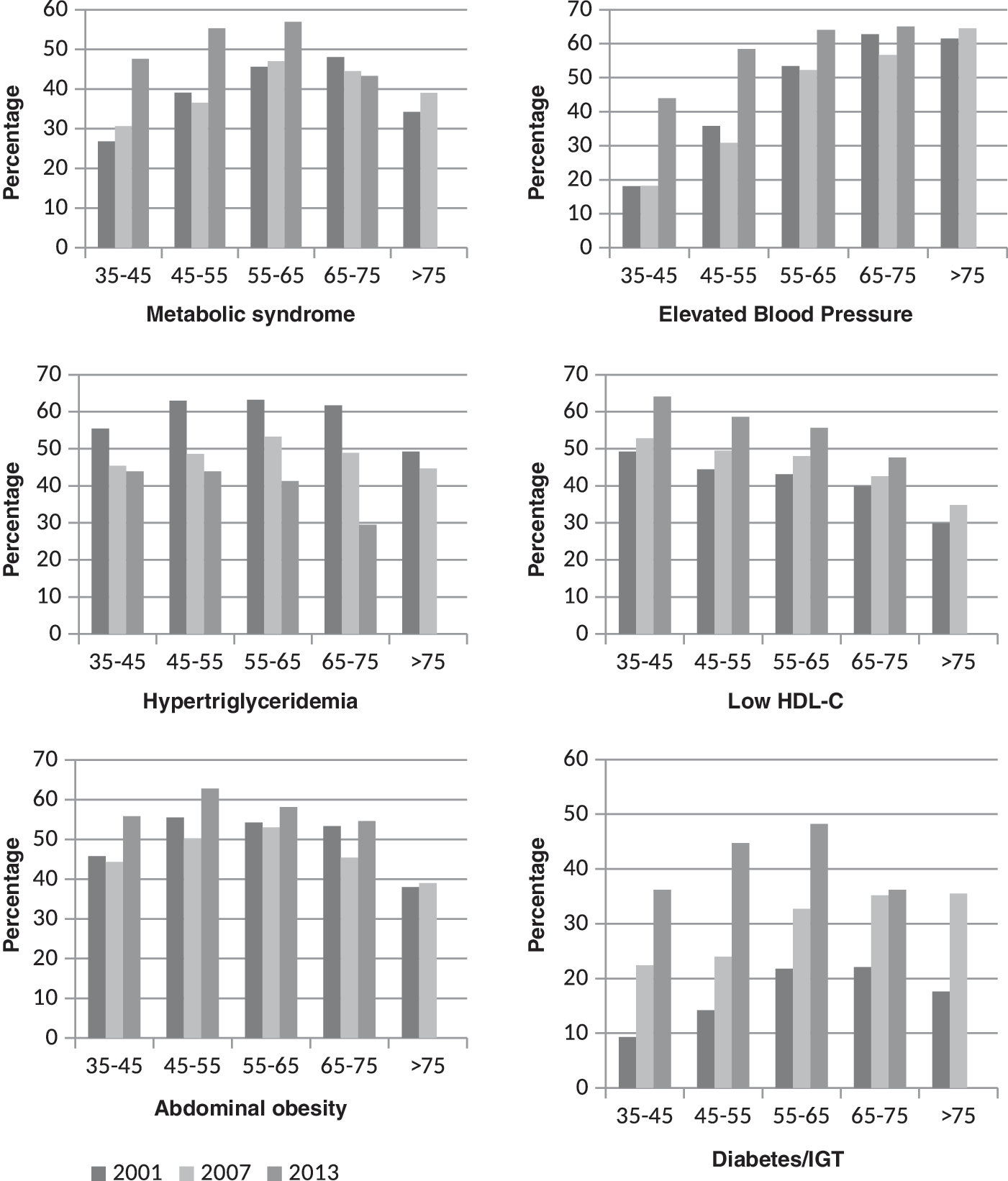
Prevalence of MetS and its components from 2001 to 2013 by age group.
Prevalence is reported in percentage.
A significant change (P < 0.05) in 2001, 2007, and 2013.
Impaired glucose: FBS ≥5.6 mmol/L (100 mg/dL), abdominal obesity: men: WC >102 cm and women: WC >88 cm, elevated blood pressure: SBP/DBP ≥130/85 mmHg, hypertriglyceridemia: Tg ≥1.7 mmol/L (150 mg/dL), low HDL-C: men: <1.03 mmol/L (40 mg/dL) women: <1.29 mmol/L (50 mg/dL).
Age-adjusted odds of MetS and its components in 2001, 2007, and 2013 were presented in Table 3. Results indicated that the risk of MetS, elevated blood pressure, low HDL-C (except for females in 2007), and impaired glucose were significantly higher in 2007 and 2013 compared with 2001 independent of age and gender. On the contrary, the risk of hypertriglyceridemia has been significantly decreased in 2007 and 2013. Moreover, the age-adjusted odds ratio for abdominal obesity decreased in 2007 and increased in 2013 compared with 2001.
CI, confidence interval; OR, odds ratio.
Discussion
This study investigated the prevalence and trends of MetS and its components among Iranian adults in a cohort study from 2001 to 2013. The current study revealed that the prevalence of MetS and most of its components were increased over the 12-year period. This study also showed an increase in the prevalence of MetS with an increase in age up to the age of 75 years followed by a decrease in its prevalence. Several factors might be responsible for this reduction, the most possible is the decrease in appetite and abdominal obesity in elderly. 20 Frequent medical check-up and treatment in people older than 75 years might be another cause for this result. Moreover, older people may not be interested in modern lifestyles such as the changes in dietary behavior were not significant among individuals older than 65 years (data not shown). Finally, individuals with MetS may develop other diseases that lead to premature death. 21 Furthermore, a small sample size in this age group compared with other age groups might have also affected the proportion of individuals with metabolic abnormalities. In the present study, a similar pattern was also observed in the components of MetS and thus confirmed the findings of previous studies, 22,23 which reported that the prevalence of MetS increases strongly with age. The Third National Health and Nutrition Survey (NHNS), on American adults, revealed that the MetS prevalence increased with age from 20–29 to 60–69 years. 23 Another study showed that the prevalence of MetS and its components increased, and the highest prevalence was reported at the ages of 60–69 years. 24 Although more risk factors emerge as age increase, this result may indicate that aging affects the MetS prevalence independent of other related factors such as genetics and environment. It has also been proposed that a lifetime accumulation of unhealthy behaviors, such as low physical activity; an unhealthy dietary intake; obesity; untreated dyslipidemia and hypertension; changes in insulin and other hormone secretion; and other physiological and environmental factors may lead to a higher prevalence of MetS in older ages. 17,25
To eliminate the effect of aging, which is an intrinsic part of cohort studies, we calculated the age-adjusted prevalence of MetS and its components from 2001 to 2013, which showed an increase in the prevalence of MetS by 6.9% from 2001 to 2013. The contributors to this increase were elevated blood pressure, low HDL-C, abdominal obesity, and diabetes/IGT (5.5%, 12.0%, 2.3%, and 18.7% respectively). Interestingly, the increases in the prevalence of MetS, elevated blood pressure, low HDL-C, abdominal obesity, and diabetes/IGT over a period of 12 years, were higher in men. Although the reason for this result is not evident, less concern for diet, health, and appearance by men compared with women may result in a metabolic worsening in men. 26
When calculating changes in the prevalence of MetS components from 2001 to 2013, an increase in the prevalence of diabetes/IGT was higher than other components and also indicated that the risk of diabetes increased in the recent years. Glucose intolerance is one of the most important characteristics of MetS. 27 Glucose intolerance increases free fatty acids 28 while insulin resistance can result in sodium retention and vasoconstriction, which eventually initiate hypertension. 29 The prevalence of diabetes is increasing as a result of aging, population growth, lifestyle changes, such as urbanization, physical inactivity, and the increasing prevalence of obesity. 30 The prevalence of diabetes is expected to be double in 2030 compared with 2010. 31 In developing countries, the number of people with diabetes has been increasing over recent decades, mostly due to rapid socioeconomic growth. 32 In addition, abdominal obesity is significantly associated with glucose intolerance/insulin resistance, 33 hypertension, 34 and hyperlipidemia. 35 As a result, abdominal obesity is a critical factor in the pathogenesis of MetS. Our results also reflect an increasing trend in abdominal obesity and decreasing trend in physical activity after 12 years. 36 During past decades a dramatic change has occurred regarding the way that people move, eat, and drink. These transformations have conflicted with personal biology, and consequently, body composition has been affected as illustrated by rising obesity in both developed and developing countries. 37,38 It has been estimated that the prevalence of obesity will increase by 33% over the next two decades, and 51% of the population will be obese by 2030. 39
On the contrary, the association of sedentary lifestyle with central adiposity, insulin resistance, 40 and hypertension 41 has been reported by previous studies. After all, an inverse association between the amount of physical activity and MetS has been documented. 42 Urbanization and rapid economic changes have been found to be associated with decreased physical activity generally and occupational, domestic, and transport-related physical activities. 43 It has also been revealed that information and communication technology and transportation changes are the most important reasons for decreasing physical activity. 44
A decreasing trend, over the 12-year period, in the prevalence of hypertriglyceridemia is another important result of this study. Previous studies also reported a decreasing trend in the level of serum lipids after 6–20 years. 45 –47 Although there is no clear reason for the decreasing prevalence of hypertriglyceridemia in our study population, there could be several possible explanations for this decreasing trend. The favorable trends in serum lipids may be due, in part, to an increase in clinical screening and recognition of dyslipidemia and also an increase in the percentage of the population who receive lipid-lowering treatment. 47 Moreover, healthy lifestyle changes, such as a decrease in the consumption of carbohydrates and trans-fatty acids has been suggested as a possible reason for this trend. 48 There is also some evidence that the decreasing trend in triglyceride levels is attributable to a reduction in cigarette smoking and carbohydrate intake. 47 Iranians traditionally used to have a high carbohydrate and saturated fat diet that could increase triglyceride levels. However, their diet has been gradually changed and the portion of carbohydrates and saturated fat consumed has decreased in recent years. 49 Moreover, it is possible that the existing public educational programs 50 may have contributed to this change. In ICS, smoking from 16.7% in 2001 decreased to 6.7% in 2007 and 2.8% in 2013. Moreover, mean consumption of bread and rice decreased in this period (data are not shown).
Another interesting result of our study is the changes in the pattern of MetS and its components between rural and urban areas. Although in 2001, as expected, the metabolic abnormalities were worse in urban areas, the inverse situation was observed in 2013. Rural areas in Iran also embraced lifestyle changes by changing their diet and decreased physical activity as a result of modern technology. It is possible that this transformation could have an important effect on abdominal obesity and, consequently, on other components of MetS. It has been reported that by increasing income, a higher prevalence of obesity was regularly reported in rural areas and among poor families due to increased intakes of refined carbohydrates, added sugars, and fats. Moreover, the increase in the prevalence of obesity was higher in rural (3.9%) than urban (2.5%) residence. 37
The strengths of this study include the assessment of MetS and its components, three times over a period of 12 years, based on a cohort data to remove the effect of diversity in the studied population. Previous studies dealt with the prevalence of MetS and its components over time using cross-sectional studies, at different points in time. Besides, in the current study the revised version of ATP III criteria, which was the best predictor of CVD in the studied population based on our previous study, 8 was used to diagnose MetS. The primary limitation of the present study was the loss to follow-up individuals over the 12-year period, which is inevitable in cohort studies. Moreover, the use of medications was based on self-reported data that may be inaccurate.
In conclusion, this study reveals a significant increasing trend in the age-standardized prevalence of MetS from 2001 to 2013 among the Iranian population. Interestingly, the increased prevalence of MetS is observed in both rural and urban areas. Aging, low physical activity, abdominal obesity, and glucose intolerance were the main determinants for increasing the prevalence of MetS. Thus, to prevent an increase in the cardiovascular risk factors and the risk of other diseases related to MetS, there is an urgent need for developing an appropriate intervention programs to control MetS and its components.
Footnotes
Acknowledgments
The authors state their appreciation to the Isfahan Cardiovascular Research Institute personnel, particularly those involved in the Isfahan Cohort Study for their serious support. Moreover, we especially thank Mrs. Mansoureh Boshtam and Mrs. Minoo Dianatkhah for their constant cooperation in ICS.
Authors' Contribution
H.K.-B. contributed to the design of the study, analyzed the data, and wrote the manuscript; M.S., H.R., M.T., and A.P. collected the data; S.-K.N. and H.P. provided guidance in performing statistical analysis and critical revision of the manuscript; N.S. contributed to the design of the study and critical revision of the manuscript; F.A. provided guidance on the overall design of the study, and critical revision of the manuscript. All authors have read and approved the final manuscript.
Author Disclosure Statement
No competing financial interests exist.