
Abstract
Background:
The current study aimed to determine the relationship between self-reported sleep duration and morbid obesity in an employee population.
Methods:
Baptist Health South Florida conducts an annual Health Risk Assessment (HRA) for its employees. Data for this cross-sectional study was collected via this HRA in 2014, and included information on self-reported sleep duration, height and weight for body mass index (BMI), and other biometric measures. Average sleep duration was categorized as short sleep (<6 hr), optimal sleep (6–7.9 hr), and long sleep duration (≥8 hr), while obesity status was categorized as nonobese (BMI <30 kg/m2), obese (30–34.9 kg/m2), and morbid obese (≥35 kg/m2).
Results:
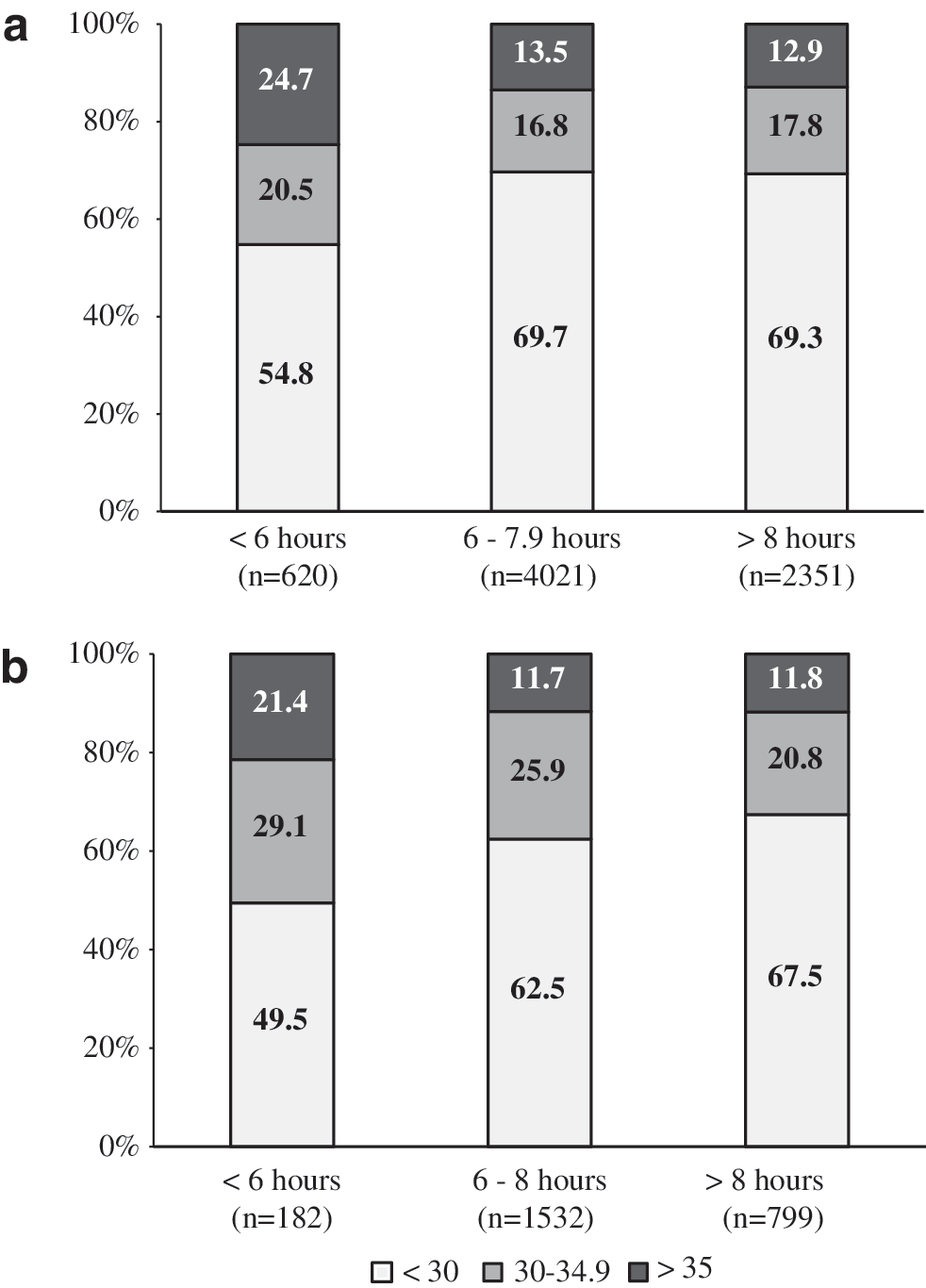
A total of 9505 participants (mean age 42.8 ± 12.1 years, 75% females, and 55% Hispanic) were included in this study. Prevalence of morbid obesity was about 24% among employees who were sleeping for less than 6 hr compared to 13% and 14% among those sleeping for 6–7.9 hours, and 8 or more hours respectively. In regression analyses, persons who slept less than 6 hr had almost twice the odds of morbid obesity compared to those who slept 6–7.9 hr (odds ratio = 1.8; 1.5–2.2).
Conclusion:
Our finding that short sleep duration (<6 hr) is significantly associated with a higher risk of morbid obesity should facilitate the development of workplace-based programs that focus on improving sleep among at-risk employees, especially those who work in shift duties to reduce the risk of morbid obesity and other comorbid conditions. Future studies are needed to further explore the relationship of sleep duration and morbid obesity in employee populations.
Introduction
O
Methods
Design and participant population
This cross-sectional study was conducted among employees of Baptist Health South Florida, a large nonprofit healthcare organization based in Miami, Florida, who participated voluntarily in an annual Health Risk Assessment (HRA) in 2014. The HRA comprised an extensive web-based health and lifestyle questionnaire and an in-person measurement of biometric data. Further details of the study procedures have previously been described. 5,6 Participants were excluded from this present study if they were pregnant at the time of the HRA. Informed consent was given by all participating employees. The study was approved by the BHSF Institutional Review Board.
Study variables
The data collected from the online health questionnaire included demographic characteristics such as age, gender, ethnic/racial origin, and educational attainment; self-reported lifestyle characteristics such as diet, smoking status, and physical activity, as well as average sleep duration and sleep quality. Biometric measures collected included height, weight, blood pressure (BP), blood glucose, and total cholesterol.
Weight and height measurements were collected using a portable stadiometer, from which body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters (kg/m2). Blood samples were collected from participants and analyzed for blood glucose and cholesterol measurements using a CardioChek® PA analyzer (PTS Diagnostics, Indianapolis, IN). BP was measured with participants seated after 5 min of rest. This procedure was repeated thrice in persons who had an elevated BP measurement. Participants' average duration of sleep at night was reported using the online questionnaire and categorized as <6 hr (short sleep duration), 6–7.9 hr (optimal sleep duration), and ≥8 hr (long sleep duration). Obesity status was categorized based on the BMI as nonobese (BMI <30 kg/m2), obese (30–34.9 kg/m2), and morbid obese (≥35kg/m2). Data for physical activity (as minutes per week of exercise) and diet (scored out of 10 points) are described elsewhere. 5,6 Smoking status was also self-reported and confirmed with CO breath test.
Statistical analysis
All data were analyzed using Stata 13 (StataCorp LP, College Station, TX). Continuous variables are described as mean and standard deviation for normally distributed variables and median/interquartile range for nonparametric variables. Categorical variables are described as frequencies. The one-way analysis of variance test (for parametric continuous variables), Kruskal–Wallis test (for nonparametric variables), and chi-square test (for proportions) were used to compare the differences between groups. All demographic variables and cardiovascular risk factors are presented in relation to categories of average sleep duration.
Unadjusted and adjusted logistic regression models were used to determine odds ratios (OR) for the association of sleep duration with obesity. Covariates included in the regression analysis for the first adjusted model were age and sex. Covariates in the first adjusted model with educational attainment and ethnicity were used in the second regression model, while the third adjusted model included the above covariates, as well as diet, physical activity, and smoking. Statistical significance for all analyses was set at P < 0.05.
Results
A total of 9505 participants (mean age 42.8 ± 12.1 years, 75% females, and 55% Hispanic) had complete information on the variables of interest. Table 1 shows the distribution of demographic and cardiovascular risk factors of the population according to categories of sleep duration. Proportionally more Non-Hispanic Blacks than Hispanics or non-Hispanic whites had a short sleep duration. Mean BMI and systolic and diastolic BPs were significantly higher, and median diet scores were significantly lower, among participants who slept for <6 hr. Figure 1a and b shows sex stratified distribution of sleep duration across BMI categories. Among both males and females, significantly more obese persons slept for <6 hr. In comparison to those who reported 6–7.9 hr of sleep, the odds for obesity among participants who sleep <6 hr were 1.8 (95% confidence interval [CI]: 1.6–2.1) (Table 2). After adjusting for age and sex, the odds for obesity among those with short sleep was 1.9 (95% CI: 1.6–2.2). In further multivariate regression models, this relationship persisted. Similarly, persons who slept <6 hr were twice as likely to be morbidly obese as those who slept between 6 and 7.9 hr (OR: 2.1; CI: 1.8–2.5). For participants who slept ≥8 hr, no significant risk for obesity or morbid obesity was observed, compared to those who slept 6–7.9 hr. Inclusion of potential confounders in regression models did not change this pattern.
DBP, diastolic blood pressure; IQR, interquartile range; SBP, systolic blood pressure.
Discussion
In this study of a large employee population, we found that compared to optimal sleep duration, an average sleep duration of less than 6 hr (short sleep duration) was significantly associated with an increased risk of both obesity and morbid obesity. This association persisted even after controlling for various demographic and lifestyle factors. However, no significant association was observed between obesity and longer sleep duration (≥8 hr).
Our findings are consistent with previous studies that have shown a relationship between a short duration of sleep and obesity. A recent meta-analysis of 11 studies conducted in 2014 found that a shorter duration of sleep (irrespective of definitions used in the individual studies) was associated with a significantly increased odds of obesity (OR = 1.45; 95% CI, 1.25–1.67). 7 In another study, Patel et al. showed that compared to persons who sleep 7–8 hr, a shorter sleep duration (<5 hr) was associated with an increased odds of obesity (BMI ≥30 kg/m2) in both men (OR 3.7, 95% CI: 2.7–5.0) and women (OR 2.3, 95% CI: 1.6–3.1). 8 Similar results were also observed in a population based study conducted by Anic et al. In that study of over 5500 women, short sleep was associated with greater odds of obesity (OR:1.89; CI: 1.45–2.47) and extreme obesity (OR 3.12; CI: 1.7–5.95). 9 Also in keeping with our findings, studies which have investigated the relationship between a longer sleep duration (>8 hr of sleep) with obesity in adults have not revealed any significant associations. 7,10
The evidence for the association of reduced sleep with obesity is overwhelming, and theories that explain how poor sleep leads to obesity have also been described. 11 –13 However, to the best of our knowledge, this is one of the first studies to examine the association between sleep and obesity among employees in a healthcare organization, which has important implications. An important characteristic of employee populations, especially in the healthcare industry, that can result in poor sleep is demanding shift work. Studies have suggested that shift work is associated with reduced sleep 14 and this may explain the risk of obesity associated with short/reduced sleep duration, the increased risk of hypertension and metabolic syndrome, and may also negatively impact employee performance and productivity. 15 –17 The foregoing highlights the need for employers to adopt policies and interventions that encourage adequate sleep. Such interventions may include modification of work scheduling and shift rotation policies, as well as incorporation of mobile technologies to facilitate education on good sleep habits and hygiene. 18
In this study, some limitations should be noted. First, self-reporting of sleep duration is potentially a source of bias. Second, our study also lacked sufficient information on, and therefore did not take into account in our analyses, job-related circumstances such as shift work, job-related stress, work schedules, and certain medical conditions among employees like depression, which may impact sleep duration adversely. Finally, the cross-sectional design of this study prevents the establishment of a temporal association between sleep duration and obesity. Despite these limitations, this study has a large sample size, conducted in a healthcare employee population. In addition, standardized methods for data collection were used in this study.
In conclusion, in this large diverse employee healthcare population, reduced sleep was associated with obesity, as well as morbid obesity. Although our findings do not suggest causality, they highlight a potentially modifiable risk factor that can result in substantial gains to employees and employers alike in terms of improved health and productivity, as well as reduced healthcare expenditure. Future studies are needed to examine the impact of wellness strategies to improve sleep, as well as employer policy changes regarding shift work to address these challenges.
Footnotes
Acknowledgment
We are highly thankful to Dr. Yugandhar Kandimalla, Department of Internal Medicine, Ocala Regional Medical Center, Florida, for contribution in revision of the current manuscript and providing candid and critical comments which has helped us in final processing of this manuscript.
Author Disclosure Statement
No competing financial interests exist.