
Abstract
Background and Aims:
Cardiovascular (CV) risk equations are routinely used to predict risk in nonbariatric populations, but have not been studied in depth in patients undergoing bariatric surgery and specifically those with impaired glucose regulation. The aim of this pilot study was to investigate changes in the 10-year and lifetime predicted CV risk in subjects with impaired glucose regulation before, 1 month, 6 months, and 5 years after bariatric surgery.
Method and Results:
A nonrandomized prospective study was conducted of 45 participants with impaired glucose regulation undergoing temporal assessments during follow-up. Body weight, body mass index (BMI), blood pressure, lipid profile, and HbA1c were recorded preoperatively, 1 month, 6 months, and 5 years postoperatively. Preoperative and postoperative predicted CV risk was calculated using the QRISK2, QRISK lifetime, and JBS3 calculators. Follow-up rates were 93%, 91%, and 71% at 1 month, 6 months, and 5 years, respectively. The sample had a mean age of 48.8 ± 7.0 years, a mean BMI of 53.9 ± 11.1 kg/m2, and a mean HbA1c of 7.5% ± 1.7%. The predicted 10-year QRISK2 score decreased by 35%, 54%, and 24% at 1 month, 6 months, and 5 years, respectively (P < 0.001). The predicted lifetime risk also decreased with the greatest reduction (24.5% with QRISK lifetime and 26.7% with JBS3 lifetime score) observed at 5 years even though the subjects were 5 years older.
Conclusion:
Bariatric surgery in patients with impaired glucose regulation is associated with a significant reduction in predicted 10-year and lifetime CV risk in a population that was 5 years older compared to baseline.
Introduction
C
Most risk prediction methods provide an absolute 10-year CV risk estimate, and several studies have demonstrated that bariatric surgery is associated with a reduction in CV risk scores. 4 –8 However, risk calculators used in most of these studies do not include body mass index (BMI) or obesity as risk factors. These CV risk calculators include the Framingham risk score (FRS), the Prospective Cardiovascular Munster Heart Study (PROCAM) score, and the United Kingdom Prospective Diabetes Study (UKPDS) Risk engine. 4,6 –9 In addition, many studies have focused on CHD risk rather than CVD risk 8,9 ; the study samples have included the entire spectrum of bariatric patients, with little focus on those impaired glucose regulation 5 –9 ; and the follow-up has also been relatively short. 5 –9 The study by Vogel et al., which consisted of 109 Roux-en-Y gastric bypass (RYGB) patients, reported that the Framingham CHD risk score decreased by 39% in men and 25% in women (P < 0.001) at 17 months following surgery. 8 Torquati et al., also observed a 50% reduction in the Framingham CHD risk score at 1 year following RYGB. 9
CVD risk is a continuum and as such the consequences might not be observed for a significant period of time. Marma et al., showed that ∼67% of adults in the United States with a low 10-year CVD risk had a high lifetime predicted risk. 10 A low 10-year but high lifetime CVD risk is more common in women and in younger age groups because age and gender are two of the main determinants in CVD risk prediction models. 10,11 Morbid obesity and bariatric surgical procedures are more frequent in females and younger age groups (<50 years), with no fewer than 70% of participants in the Swedish Obese Subjects Study being female with a mean age of 47 years. 3,12 To date, no studies have examined the effect of bariatric surgery on the predicted lifetime CVD risk.
The aim of this pilot study was to investigate changes in the temporal 10-year and the lifetime predicted CV risk in subjects with impaired glucose regulation preoperatively and 1 month, 6 months, and 5 years following bariatric surgery using the QRESEARCH Cardiovascular Risk Algorithm (QRISK2), QRISK lifetime, and Joint British Societies 3 (JBS3) score. The QRISK scores and JBS3 score are developed and validated in the United Kingdom and include BMI as a variable in their calculation. 11,13 –15
Materials and Methods
Participants
Approval for the study was obtained from the Local Research Ethics Committee (South West Wales; LREC reference 06/WMW02/7) and ABM University Health Board. Participants were identified and recruited from patients undergoing a planned bariatric surgical procedure in our center. Entry criteria at the outset included the following: both genders, age 20–60 years, BMI >40 kg/m2, and physically fit for surgery. All subjects had previously been diagnosed with type 2 diabetes, or diagnosed during an oral 75 grams glucose tolerance test at the start of the study according to American Diabetes Association (ADA) criteria 16 or impaired glucose tolerance according to ADA criteria. 16 All participants were recruited preoperatively and followed up postoperatively at 1 month, 6 months, and 5 years. This study sample has been previously described. 17 –19
Data collection
Data were collected at baseline (preoperatively), 1 and 6 months, and 5 years postoperatively. Age, sex, ethnicity, address, medications, diabetes, cigarette smoking, family history of CVD, and relevant medical history were self-reported using standardized questionnaire. Height and weight were measured according to local standard protocol, and BMI was calculated as kg/m2. The percentage excess weight loss (%EWL) was calculated using the Ideal body weight at a BMI of 25 kg/m2. 20 A single measurement of systolic and diastolic blood pressure was obtained by the same trained registered nurse. Glucose, hemoglobin A1c (HbA1c), creatinine, estimated glomerular filtration rate, and lipid profile [total cholesterol, high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C), and triglyceride] were analyzed within the local hospital accredited laboratory. Diabetes remission is defined as follows: (1) complete remission with a HbA1c <6% and fasting blood glucose <5.6 mmol/L and off medication and (2) partial remission with a HbA1c 6%–6.4% and fasting blood glucose 5.6–6.9 mmol/L and off medication. 21
CV risk estimation
CV risk, both pre- and postoperatively, was calculated using online calculators as follows: QRISK2-2016 (
Statistical analysis
Statistical analysis was performed using SPSS (version 22; SPSS, Inc., Chicago). Continuous data with a normal distribution are presented as mean and standard deviation, and data which did not have a normal distribution are described as median and interquartile range. A paired samples t-test, one-way repeated measure ANOVA, and independent samples t-test were used for continuous variables with a normal distribution, and the Friedman's test, the Wilcoxon signed rank test, and the Mann–Whitney U test were used for continuous variables, which did not have a normal distribution. The Chi-squared test was used for analysis of categorical variables. In all cases, a P ≤ 0.05 was considered statistically significant.
Results
Participant characteristics
Of the 49 participants, four had pre-existing CVD preoperatively and were excluded from further analysis. Of the remaining 45 subjects, 42 and 41 participants attended the 1- and 6-month follow-up postoperative visits. At the time of article preparation (February 2016), 20 participants had attended a 5-year follow-up visit; 12 participants had attended a follow-up visit with their general practitioners; 8 were lost to follow-up; and 5 were deceased (Fig. 1). At 5 years, data for clinical measures of obesity were available for 27 participants, HbA1c for 31 participants, lipid profile for 30 participants, and medication history for 36 participants. Within the sample, 24 participants had undergone a laparoscopic sleeve gastrectomy, 12 a biliopancreatic diversion, 6 a RYGB, and 3 a laparoscopic adjustable gastric banding.
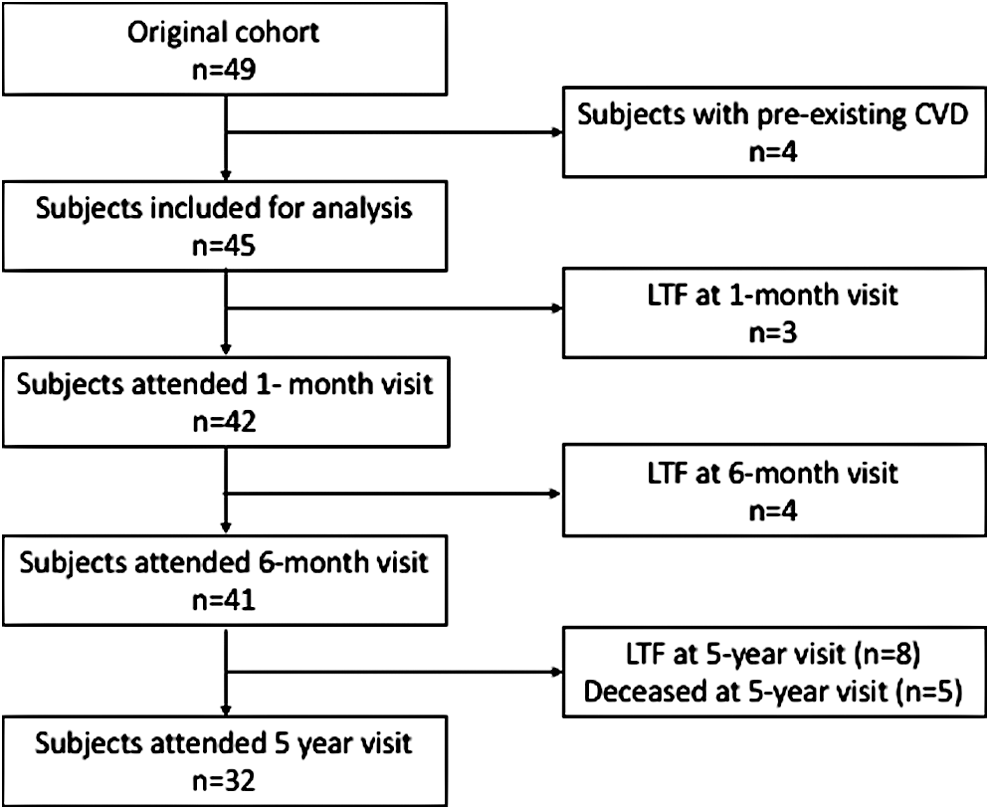
Flow chart showing number of attenders and nonattenders at each visit. LTF, loss to follow-up.
Changes in clinical measures of obesity
Table 1 shows the changes in clinical measures of obesity at 1 month, 6 months, and 5 years following bariatric surgery. The greatest changes were seen at 6 months postoperatively and these were maintained at 5 years. The maximum %EWL (45% ± 18%) was achieved at 6 months following surgery (P < 0.001).
Data are presented as mean ± SD.
P value comparing baseline with 1 month.
P value comparing baseline with 6 months.
P value comparing baseline with 5 years.
Data are presented as median and interquartile range.
BMI, body mass index; %EWL, percentage excess weight loss; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol.
Changes in CV risk factors
Table 1 shows the changes in risk factors for all available subjects at 1 month, 6 months, and 5 years after bariatric surgery. Significant reductions in both systolic and diastolic blood pressures were observed at 1 month. The mean systolic blood pressure decreased by 10.9 ± 4.3 mmHg (P = 0.02) and the mean diastolic blood pressure by 7.3 ± 2.5 mmHg (P = 0.009) at 1 month. No significant changes in blood pressure were recorded at 6-month and 5-year visits.
Total serum cholesterol concentration showed a decrease at 1 month but an increase at 5 years (P = 0.034). HDL-C showed a similar trend to that of total cholesterol (P < 0.001). Significant changes in serum triglyceride level were observed at 6 months, but there was no significant change in LDL-C level.
The greatest change in mean HbA1c was observed at 6 months (P < 0.001). Mean HbA1c decreased by 1.0%, 1.7%, and 1.0% at 1 month, 6 months, and 5 years, respectively (P < 0.001). Of those patients with type 2 diabetes, 71% achieved the National Institute of Health and Care Excellence (NICE) recommended target HbA1c of 7% at 5 years after bariatric surgery. The prevalence of complete remission of type 2 diabetes at 1 month, 6 months, and 5 years postoperatively was 27%, 44.7%, and 35.5%, respectively (P < 0.001). The prevalence of partial remission of T2DM was 18%, 8%, and 18.5% at 1 month, 6 months, and 5 years, respectively (P < 0.001).
Changes in medications
Table 2 shows the changes in medication following bariatric surgery. The requirement for diabetes medication was significantly lower following surgery. A decrease in antihypertensive medication was also observed (68.9% at baseline vs. 39.4% at 5 years), but this was not statistically significant (P = 0.463). The proportion of participants no longer requiring lipid-lowering medication was greatest at 5 years (35.6% at baseline vs. 63.9% at 5 years), but this was not again statistically significant (P = 0.0728).
P values calculated from Chi-squared analysis.
Changes in predicted 10-year CV risk
The preoperative and postoperative QRISK2 scores were calculated using the age at the time of visit. A significant reduction in 10-year predicted QRISK2 scores was observed across the temporal time points (P < 0.001). Table 3 shows the percentage change in absolute risk and relative risk. The QRISK2 calculator also provides relative risk, which is calculated by dividing the subject's predicted risk score by a healthy subject's risk. A healthy person is defined as an individual with same age, sex, and ethnicity; no adverse clinical indicators; a BMI of 25 kg/m2; a systolic blood pressure of 125 mmHg; and a cholesterol ratio of 4. Risk groups were categorized as follows: a score of <10% as low risk; a score of 10%–19% as moderate; and a score of ≥20% as high risk. Chi-squared analysis revealed that there was a significant difference in distribution of low, moderate, and high-risk groups before and after bariatric surgery (P = 0.042) (Fig. 2).

Distribution of risk groups classified by QRISK2 score, before and 1 month, 6 months, and 5 years after bariatric surgery. Chi-squared analysis revealed a significant difference in distribution of risk groups before and after bariatric surgery (P = 0.042). Low risk group: score <10; moderate risk group: score 10–19; and high risk group: score ≥20.
Data are presented as median and interquartile range.
JBS3, Joint British Societies 3.
Table 3 shows changes in the 10-year JBS3 score preoperatively, 1 and 6 months, and 5 years after bariatric surgery. The predicted 10-year JBS3 score was lower at 1 and 6 months, but at 5 years the score was similar to the preoperative level. After adjusting for age, a significant change in 10-year JBS3 score was observed at 5 years (P < 0.001). No significant difference in the distribution of risk groups before and after bariatric surgery was observed.
Changes in predicted lifetime CV risk
We observed that bariatric surgery had a positive impact not only on predicted 10-year CVD risk but also on the lifetime CVD risk. Table 4 shows changes in the QRISK lifetime score and JBS3 lifetime score. The maximum decrease in predicted lifetime CVD risk was observed at 5 years for both risk assessment models. Mean lifetime QRISK score decreased by 10.3%, 15.9%, and 24.5% at 1 month, 6 months, and 5 years, respectively (P < 0.001). Similar observations were seen for the lifetime JBS3 score as follows: 11.8% reduction at 1 month; 15.3% reduction at 6 months; and 26.7% reduction at 5 years (P < 0.001).
Data are presented as mean ± SD.
An one-way repeated measures ANOVA followed by paired t-test revealed significant changes in predicted lifetime cardiovascular disease score over time (P < 0.001).
Baseline predicted CVD risk scores between attenders and nonattenders
Table 5 shows baseline predicted CVD risk scores between two groups defined by their 5-year status. Attenders were those who had attended follow-up visit at 5 years. Nonattenders included those who were lost to follow-up or deceased. There were no differences in baseline risk scores between two groups.
Data are presented as mean ± SD.
Data are presented as median and interquartile range.
Discussion
Our pilot study has demonstrated that bariatric surgery is associated with a reduction in predicted 10-year CVD risk and predicted lifetime CVD risk despite the patients being years older. To our knowledge, no previous studies have examined the effect of bariatric surgery on predicted lifetime CV risk in individuals with impaired glucose regulation. Since the long-term effects of bariatric surgery on CVD events are unclear, there is a need to investigate the effect on predicted lifetime CVD risk following bariatric surgery. The 10-year CVD risk alone might miss a proportion of those with a high lifetime risk. Mackey et al., reported that 76% of bariatric patients with a low 10-year predicted risk had a high lifetime CVD risk. 22 We observed that bariatric surgery was associated with a continuous decrease in the lifetime CVD risk. Of note, age alone is a nonmodifiable risk factor for the development of CVD. In a cohort of 3.6 million individuals aged ≥40 years, the prevalence of any vascular disease increased significantly with each decade of life: 2% in 50 year olds, 3.5% in 60 year olds, 7.1% in 70 year olds, 13% in 80 year olds, and 22.3% in 90 year olds. 23 In our study, the maximum reduction in lifetime CVD risk (up to 26% reduction) was observed at 5 years despite the participants being 5 years older. We also observed a reduction in 10-year CVD risk as follows: 54% reduction in QRISK2 score at 6 months and 24% reduction at 5 years. The relative risk reduction in QRISK2 was more pronounced at 5 years compared to absolute risk reduction (59% vs. 24%). A significant reduction in predicted 10-year JBS3 score was observed at 5 years after adjusting age to baseline. Of interest, several studies have demonstrated that bariatric surgery is associated with a reduction in predicted 10-year CVD risk. The study by Batsis et al., 7 which included 197 RYGB patients and 163 control patients, used the FRS and the PROCAM risk score. The 10-year FRS CVD risk score was lower at 3.3 years in the surgical group (from 7.0% to 3.5%; P < 0.001) compared to the control group (from 7.1% to 6.5%; P < 0.001). The PROCAM score was also lower in the surgical group (4.1%–2.0%; P < 0.001) compared to the control group (4.4%–3.8%; P = 0.08). Aminian et al., demonstrated that RYGB was associated with a relative risk reduction of 27% for 10-year overall risk of CHD, stroke, and peripheral vascular disease; 20% for 10-year risk of CHD; 40% for 10-year risk of myocardial infarction; 42% for 10-year risk of stroke; and 47% for 4-year risk of intermittent claudication in a cohort of 131 diabetic patients at 6 years. 4 Radwan et al. reported that QRISK2 score was significantly lower in a cohort of 250 bariatric surgical patients at 24 months. 5
The QRISK2 algorithm has been developed using routinely collected data from Primary Care practices across England and Wales. The study cohort consisted of 2.3 million patients aged 35–74 years from 531 practices. Validation studies demonstrated that QRISK2 identified high-risk patients more accurately than the modified Framingham score in the U.K. population. 14,24 Recent guidance from NICE recommends QRISK2 as the CVD risk assessment tool. 25 QRISK2-2016 utilizes the following variables: age, gender, ethnicity, Townsend score, smoking status, diabetes mellitus, family history of CVD, chronic kidney disease, atrial fibrillation, rheumatoid arthritis, blood pressure treatment, systolic blood pressure, total cholesterol, HDL-C, and BMI. 26 End points assessed in QRISK2 are fatal and nonfatal myocardial infarct, angina, coronary revascularization, fatal and nonfatal stroke, transient ischemic attack, and intermittent claudication. The QRISK lifetime 14 uses the same variables as QRISK2 and calculates CV risk up to 95 years of age. The JBS3 risk calculator was also developed in the United Kingdom and released in 2014. Variables used and end points assessed in JBS3 are similar to those in QRISK2. 11
Bariatric surgery aims to provide improvement in CVD risk factors and long-term weight loss. In our current study, we observed a reduction of 44% in %EWL, 22.7% in body weight, 35.5% in prevalence of diabetes remission, a reduced proportion of glucose lowering medication, improvement in CV biomarkers with an increase in HDL-C, and a decrease in total cholesterol to HDL-C ratio at 5 years. The increase in total cholesterol may be explained by the increase in HDL-C and the decrease in total to HDL-C ratio. A reduction in both systolic and diastolic blood pressure, lower antihypertensive medication, and lipid lowering medication were observed, but the differences were not statistically significant.
One of the limitations of our study is that these risk assessment tools have not previously been validated specifically in those with impaired glucose regulation and morbid obesity. Another limitation is the drop-out rate at 5 years. However, we observed no differences in baseline risk scores between participants with follow-up and those lost to follow-up or were deceased. In addition, significant reductions in risk scores were observed in the baseline-observation-carried-forward analysis (data not shown). A further limitation is the small number of patients included. Nevertheless, this study is the first study to examine the predicted lifetime CVD risk in bariatric surgical patients with impaired glucose regulation. We also have temporal measures from preoperative to 1 month, 6 months, and 5 years postoperative period.
Conclusion
In conclusion, the results of this pilot study indicate that bariatric surgery in patients with impaired glucose regulation is associated with a significant reduction in predicted 10-year and lifetime CVD risk in a population that was on average 5 years older compared to baseline. Furthermore, we observed long-term weight loss, excellent control of diabetes, and less of a requirement for hypoglycemic agents. This is a pilot study with a small sample size, and hence, further studies with larger numbers are warranted.
Footnotes
Acknowledgments
The authors thank Dr. Rachel Still and the staff of the Department of Clinical Chemistry at Morriston Hospital; ABM University Health Board for their assistance and collaboration in measuring glucose, insulin, and C-peptide; Jane Griffiths, Kathie Wareham, Nia Jenkins, Caroline Parsley, and James Morgan for subject recruitment and data collection; Claire MacIver for data collection; and Gareth Dunseath for laboratory analysis. This study was supported by a project research grant from the BUPA Foundation (33NOV06).
Author Disclosure Statement
No conflicting financial interests exist.