
Abstract
Background:
Metabolic syndrome (MetS) is an important cardiovascular risk factor for insulin resistance and has been linked to colorectal adenoma via inflammation. The neutrophil-to-lymphocyte ratio (NLR) has been suggested as an important inflammatory marker. We initiated this investigation to determine the relationship between colorectal adenoma and NLR in patients with MetS.
Methods:
We examined participants who visited the Health Promotion Center at Kosin University Gospel Hospital, Busan, Korea. Subjects who underwent both colonoscopy and liver ultrasonography were included. Colorectal adenoma was defined as the presence of a colon polyp with a histologically adenomatous component. MetS was defined according to the modified National Cholesterol Education Program Adult Treatment Panel III definition for South Asians. Anthropometric measurements and biochemical tests of liver and metabolic function were assessed.
Results:
A total of 1007 subjects were included in the study sample. Their mean age was 48.3 ± 9.7 years and 262 (26.0%) subjects had MetS, while 439 (43.6%) subjects had pathologically proven colorectal adenoma. Subjects with MetS were older, more likely to be male, and had significantly higher prevalences of colorectal adenoma (49.2% vs. 41.6%, P = 0.032), nonalcoholic fatty liver disease (62.8% vs. 19.5%, P < 0.001), and higher NLR (2.0 ± 0.9 vs. 1.7 ± 0.7, P < 0.001) compared to those without MetS. High NLR (≥2.0) was an independent factor affecting the prevalence of colorectal adenoma [odds ratio (OR) 1.38, confidence interval (95% CI) 1.02–1.88, P = 0.040], especially in subjects with MetS (OR 1.91, 95% CI 1.12–3.28, P = 0.018).
Conclusion:
High NLR was associated with increased colorectal adenomatous polyps, particularly in subjects with MetS. Screening colonoscopies for the prevention of colorectal adenoma may be warranted for patients with high NLR and MetS.
Introduction
C
Metabolic syndrome (MetS) is an important cardiovascular risk factor related to insulin resistance that has also been linked to colorectal adenoma via inflammation. 9 –11 Among the components of MetS, central obesity, hyperglycemia, and dyslipidemia are associated with increased risk of CRC. 12 –14 Recent studies have shown that MetS is an important risk factor for the occurrence of colorectal adenoma. 15 –17 According to revised National Cholesterol Education Program (NCEP) criteria, the prevalences of MetS in Korean men and women in 2007 were reported to be 29.0% and 32.9%, respectively. 18 Nonalcoholic fatty liver disease (NAFLD) is regarded as a manifestation of MetS in the liver and is associated with inflammation and increased oxidative stress. 19 In a meta-analysis, NAFLD was a significant predictor of colorectal adenoma in asymptomatic patients. 20
Buyukkaya et al. found that the neutrophil-to-lymphocyte ratio (NLR) was associated with the presence and severity of MetS. 21 NLR has been suggested as a potential predictor of long-term outcomes in patients with CRC and can be easily calculated as the neutrophil count divided by the lymphocyte count and, therefore, can be routinely used in clinical practice. Some researchers have proposed that relative neutrophilia and lymphocytopenia may constitute part of the cancer-induced systemic response to inflammation. 22 NLR has been suggested as a possible biomarker of neoplastic colon polyps and could therefore potentially distinguish neoplastic polyps from non-neoplastic polyps. 23 In addition, NLR might gradually increase in the pathway from adenoma to cancer. 24
Based on previous studies, we hypothesized that NLR, NAFLD, and MetS might be associated with colorectal adenoma and evaluated the impacts of NLR, NAFLD, and MetS on the prevalence of colorectal adenoma.
Materials and Methods
Study sample
We examined subjects who visited the Health Promotion Center at Kosin University Gospel Hospital, Busan, Korea, from January 2010 to January 2011, for routine health examinations. Subjects who underwent both colonoscopy and liver ultrasonography were included. Subjects who were diagnosed with CRC by colonoscopy or for whom liver masses were detected during liver ultrasonography (USG) were excluded. Detailed clinical data for all participants, including patient age, gender, history of smoking, alcohol consumption, and exercise, family history of cancer, and history of medication use, were collected through a self-administered questionnaire. Cigarette smoking was divided into three categories based on current use estimates: nonsmoker, ex-smoker, and current smoker. Alcohol consumption was classified into three categories: abstinence (no alcoholic drinks consumed within the last year), moderate drinking (less than 14 standard drinks consumed per week for men or 7 for women), and heavy drinking (more than 14 standard drinks consumed per week for men or 7 for women). 25 Physical activity was classified as low or moderate/high. Low physical activity was defined as 150 min or less of moderate-intensity or 75 min or less of vigorous-intensity exercise per week. 26
Height and weight were measured while patients were wearing light clothing without shoes. Blood pressure was measured in the right arm using an appropriately sized cuff and a standard mercury sphygmomanometer in a sitting position and was recorded as the average of three measurements. Body mass index (BMI) was calculated by dividing weight (kg) by height squared (m2), and waist circumference was measured at the end of normal expiration. Blood sample was collected from the antecubital vein after at least an 8-hr fast and was sent for analysis within 4 hr of collection. Fasting blood glucose levels were measured using the hexokinase method. Complete blood count parameters (neutrophil, lymphocyte, platelet, and hemoglobin) were measured by an ADVIA 2120 analyzer (Siemens Healthcare Diagnostics, Surrey, United Kingdom). Fasting serum total cholesterol, low-density lipoprotein, high-density lipoprotein (HDL), triglycerides, alanine transaminase (ALT), and aspartate transaminase (AST) were measured by enzymatic methods with a chemistry analyzer (TBA 200-FR, Toshiba, Japan). This study was approved by the Institutional Review Board of Kosin University Gospel Hospital.
Definitions of Mets and NAFLD
MetS was defined according to the modified NCEP Adult Treatment Panel III (NCEP-ATP III) definition for South Asians. 11 Subjects with three or more of the following criteria were diagnosed with MetS: central obesity (waist circumference ≥90 cm for men and ≥85 cm for women), 27 fasting plasma glucose ≥100 mg/dL or current treatment for diabetes mellitus, systolic blood pressure ≥130 mmHg or diastolic blood pressure ≥85 mmHg or current treatment for hypertension, serum triglyceride ≥150 mg/dL, and HDL <40 mg/dL in males or <50 mg/dL in females.
NAFLD was defined according to the presence of hepatic steatosis without causes such as significant alcohol use by liver USG. The diagnosis of hepatic steatosis was made according to criteria, including liver brightness, hepatorenal echogenic contrast, deep attenuation, and vascular blurring. 28 NAFLD fibrosis score was calculated by the following formula: −1.675 + 0.037 × age (years) + 0.094 × BMI (kg/m2) + 1.13 × impaired fasting glucose/diabetes (yes = 1, no = 0) + 0.99 × AST/ALT ratio − 0.013 × platelet (109/L) − 0.66 × albumin (g/dL). 29
Assessment of NLR
The neutrophil and lymphocyte counts were used to calculate NLR in blood samples from participants. NLR was calculated by dividing the absolute neutrophil count by the absolute lymphocyte count. Cutoff values, sensitivity, and specificity of the NLR were evaluated using receiver operating characteristic (ROC) curves.
Diagnosis of colon polyps
All colonoscopies were performed by one experienced endoscopist at the Health Promotion Center of our hospital with an EVIS LUCERA CV-260 colonoscope (Olympus, Tokyo, Japan). The sizes and locations of all detected polypoid lesions were recorded, and the lesions were subsequently biopsied or removed. All specimens were histologically evaluated by experienced pathologists. Colorectal adenoma was defined as the presence of a colon polyp with histologically adenomatous component, and advanced adenoma was defined as adenoma 1 cm or greater in size, or with high grade dysplasia (HGD), or with a villous component (tubulovillous or villous).
Statistical analyses
Continuous data with normal distributions are expressed as mean ± standard deviation, and categorical data are presented as the number of patients (%). Student's t-test and the chi-square test were performed for continuous and categorical variables, as appropriate. ROC curves were used to assess the ability of the NLR to predict the prevalence of colorectal adenoma. Cutoff values, sensitivity, and specificity were derived for each parameter. The efficacy of NLR for predicting the prevalence of colorectal adenoma was analyzed by univariate and multivariate logistic regression analyses adjusted for the variables with a significance level of P < 0.10 in univariate analysis. Each odds ratio (OR) is presented with a 95% confidence interval (CI). P-values less than 0.05 were considered statistically significant. Statistical analyses were performed using IBM SPSS version 23.0 (IBM Co., Armonk, NY).
Results
Baseline characteristics of the study sample
A total of 1007 participants were included in the analysis. The mean age of participants was 48.3 ± 9.7 years and 659 (65.4%) subjects were male. Among the subjects, 262 (26.0%) had MetS, 309 (30.7%) had NAFLD, and 164 (16.3%) had both MetS and NAFLD. Baseline characteristics are summarized in Table 1. Subjects with MetS were significantly older and more likely to be male. They had higher BMI, larger waist circumference, more severe smoking and alcohol histories, and higher prevalence of NAFLD compared with subjects without MetS (Table 2). The mean NAFLD fibrosis score of subjects with MetS was −1.72 ± 1.29, and that of subjects without MetS was −2.36 ± 1.21. The mean NLR of subjects with MetS was 2.0 ± 0.9 and that of subjects without MetS was 1.7 ± 0.7. In ROC analysis, the NLR was found to have the largest area under the curve (AUC = 0.571, 95% CI 0.501–0.641, P = 0.047) with an optimal NLR cutoff value of 2.0 (sensitivity 42%, specificity 72%) for predicting colorectal adenoma.
Data are presented as mean ± SD or number (percentage).
Exercise was defined as aerobic exercise performed for 30 min or more per day.
Metabolic syndrome was defined according to the modified National Cholesterol Education Program Adult Treatment Panel III definition for South Asians.
NAFLD was diagnosed based on ultrasonographic findings.
BMI, body mass index; BP, blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein; MetS, metabolic syndrome; NAFLD, nonalcoholic fatty liver disease.
Data are presented as mean ± SD or number (percentage).
NLR, neutrophil-to-lymphocyte ratio.
Characteristics of colon polyps
Table 3 shows the characteristics of colon polyps according to the presence of MetS. Colon polyps were more often detected in subjects with MetS compared to those without MetS (71.8% vs. 61.5%, P = 0.003). The mean number of detected colon polyps in subjects with MetS was higher than that in subjects without MetS (2.5 ± 2.8 vs. 1.9 ± 2.9, P = 0.004). However, the location of colon polyps and the proportion of large polyps (≥1 cm) were not significantly different between the groups. In assessments of histopathology, adenoma was more often detected in subjects with MetS than in those without MetS (49.2% vs. 41.6%, P = 0.032). However, the detection of advanced adenoma was not significantly different between groups (13.4% vs. 9.5%, P = 0.082).
Data are presented as mean ± SD or number (percentage).
Colon adenoma was defined as a colon polyp with histologically adenomatous components.
Advanced adenoma was defined as adenoma that was 1 cm or greater, or with HGD, or with villous component (tubulovillous or villous).
HGD, high grade dysplasia.
Prevalence of colorectal adenoma according to NLR
Figure 1 shows the prevalence of colorectal adenoma according to NLR. In subjects with high NLR (≥2.0) (n = 262), colorectal adenoma was more likely to be detected than in those with low NLR (<2.0) (n = 745). The difference between groups was significant (51.1% vs. 40.9%, P = 0.004). In addition, we assessed the prevalence of colorectal adenoma in subjects with NAFLD or MetS according to NLR. Among subjects with NAFLD (n = 309), the prevalence of colorectal adenoma was 51.2% (n = 110) and 48.9% (n = 46) in subjects with low NLR (n = 215) and high NLR (n = 94), respectively, and the difference was not significant (P = 0.719). However, among subjects with MetS (n = 262), the prevalence of colorectal adenoma was 44.4% (n = 75) and 58.1% (n = 54) in subjects with low NLR (n = 168) and high NLR (n = 93), respectively, and the difference was significant (P = 0.034) (Fig. 2).

Prevalence of colon adenoma according to NLR. NLR, neutrophil-to-lymphocyte ratio.
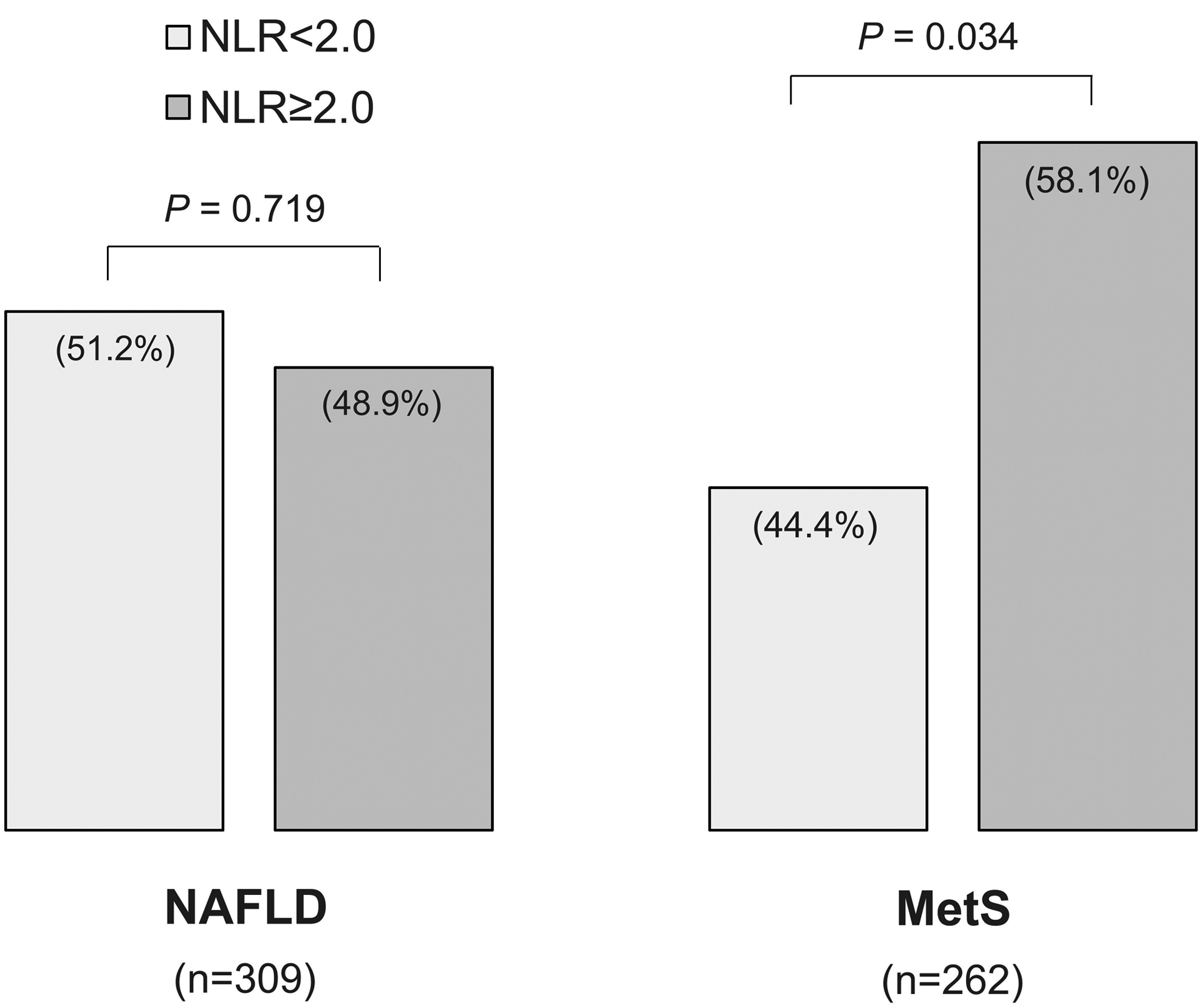
Prevalence of colon adenoma in patients with NAFLD and MetS according to neutrophil-to-lymphocyte ratio. MetS, metabolic syndrome; NAFLD, nonalcoholic fatty liver disease.
Factors affecting the prevalence of adenomatous polyps
In univariate logistic regression analysis, NAFLD, NAFLD fibrosis score, MetS, and high NLR (≥2.0) were found to be predictors of the prevalence of colorectal adenoma. However, NAFLD, NAFLD fibrosis score, and MetS were not found to be significant predictive factors after adjusting for covariates, including age, gender, BMI, and smoking, which are factors that affect the prevalence of colorectal adenoma. High NLR was an independent factor affecting the prevalence of colorectal adenoma after adjusting for age, gender, BMI, smoking, alcohol, and exercise (OR 1.38, 95% CI 1.01–1.87, P = 0.043), especially in subjects with MetS (OR 1.94, 95% CI 1.13–3.32, P = 0.016) (Table 4).
Model 1, unadjusted; Model 2, adjusted for age and gender; Model 3, adjusted for age, gender, BMI, smoking, alcohol, and exercise.
Adjusted for age, gender, BMI, smoking, alcohol, and exercise.
OR, odds ratio; CI, confidence interval.
Discussion
The results of the present study indicate that high NLR (≥2.0) is associated with increased risk of colorectal adenoma, especially in subjects with MetS. According to our results, screening colonoscopies may be helpful for the prevention of colorectal adenoma when routine health examinations detect elevated NLR and MetS. To our knowledge, this is the first study demonstrating the usefulness of NLR for predicting the occurrence of colorectal adenoma in patients with MetS.
MetS is not only known to be a main cause of cardiovascular disease but is also a risk factor for various cancers. 30,31 MetS is reported to have a close relationship with colorectal neoplasm. 17,32,33 Possible mechanisms for the close relationship between MetS and colorectal neoplasm include obesity-induced insulin resistance and inflammation. Epidemiologic studies have shown that obesity is an independent risk factor for the development of colorectal adenoma. 34,35 Some studies have suggested that dyslipidemia also has a positive relationship with increased risk of colorectal adenoma. 36 –38
Inflammatory response may increase the risk of developing many types of cancers. 39,40 NF-κB, STAT3 (signal transducer and activator of transcription 3), and inflammatory cytokines, including IL-1β, IL-6, and TNF-α produced in chronic inflammatory states, are associated with cellular survival and proliferation. 39,41 Most CRCs arise from adenoma, and genetic alterations are involved in each step from adenoma to carcinoma. 42 Microenvironments, including inflammatory cells, have been considered as factors underlying genetic alterations. 43 However, few studies have addressed the relationship between inflammatory response and the development of colorectal adenoma. Nonsteroidal anti-inflammatory drugs (NSAIDs) have been shown to reduce the risk of colorectal adenoma by inhibiting cyclooxygenase (COX) enzymes. 44,45 In experimental studies, NSAIDs suppressed the growth of CRC by COX2 mechanisms, including activation of apoptotic and anti-inflammatory signals. 46,47 In other words, the inhibition of inflammatory responses may reduce the risk of development of colorectal adenoma, and some inflammatory markers may be helpful to screen for risk of colorectal adenoma. Karaman et al. showed that patients with neoplastic polyps (tubular adenoma, villous adenoma, or tubulovillous adenoma) had higher NLR than those with non-neoplastic polyps (hyperplastic polyp or inflammatory pseudopolyp). 23 Ucmak and Tuncel reported that NLR levels were significantly higher in patients with large polyps (≥1 cm) than in patients with small polyps (<1 cm). 24 In this study, we focused on the possibility that NLR had a positive relationship with risk of colorectal adenoma, and found that high NLR (≥2.0) was associated with increased risk of colorectal adenoma. In addition, we found that high NLR was an independent factor affecting the prevalence of colorectal adenoma in subjects with MetS, and that high NLR was associated with risk of colorectal adenoma that was about two times greater than that of patients with low NLR (Table 4).
NAFLD is a common hepatic manifestation of MetS, and cardiovascular disease a major cause of mortality in patients with NAFLD. 19 Previous studies reported that NAFLD is associated with a high prevalence of colorectal adenoma. 48 –50 However, the prevalence of colorectal adenoma in subjects with NAFLD was not significantly different according to NLR (Fig. 2). Our results suggest that NAFLD is not an independent factor affecting the prevalence of colorectal adenoma after adjusting for covariates (Table 4).
This study has some limitations. First, this study was retrospectively performed in a single center. Therefore, we could not avoid selection bias when collecting information on subjects. However, we attempted to minimize bias by repeatedly reviewing medical records. Second, the NLR was assessed using single measurements at the time of first visit. If participants had infectious diseases that could increase NLR values at the time of their visits, NLR measurements may be incorrect. It would be better to average the NLR of participants for several years.
In conclusion, we found that high NLR is a useful predictor of colorectal adenoma, especially in subjects with MetS. Based on our results, assessing NLR during routine health examinations might be helpful in recommending screening colonoscopies to prevent colorectal adenoma, especially in subjects with MetS. Further prospective, longitudinal studies will be needed to clarify the usefulness of NLR during routine health examinations for predicting the prevalence of colorectal adenoma.
Footnotes
Acknowledgment
This study was supported by a grant from Kosin University College of Medicine (2016).
Author Disclosure Statement
No competing financial interests exist.