
Abstract
Background:
The increasing prevalence of metabolic syndrome (MetS) in childhood makes lifestyle interventions imperative during adolescence. This study aimed to assess the effects of a community-based lifestyle intervention on MetS and its components in adolescents.
Methods:
Adolescents, based on their residential area were categorized into three groups: complete intervention (residing in the intervention area at baseline and during all follow-ups), incomplete intervention (residing in either the intervention or control areas and were in transition between these two areas), and control group (residing in the control area at baseline and throughout all follow-ups). All measurements were repeated every 3 years for up to 9 years. Lifestyle intervention aimed at achieving healthy dietary patterns and increasing physical activity. Generalized estimating equation models were used to analyze data.
Results:
In boys with incomplete intervention versus controls, the prevalence of MetS was significantly lower in the short term (14.0 vs. 22.9), but not in long term. In boys with complete intervention, the prevalence was significantly lower versus controls (9.0 vs. 23.4) in the long term. In girls, the short-term prevalence of MetS was significantly lower in the complete intervention group compared with controls (2.5 vs. 9.1) and then remained constantly low in all study groups after that. Among MetS components, in boys, triglycerides and fasting plasma glucose in the short term and high-density lipoprotein mid term, and in girls HDL in mid and long term were both significantly improved. The odds of MetS decreased significantly in the complete [odds ratio (OR): 0.516, confidence interval (95% CI): 0.273–0.973] and incomplete (OR: 0.591, 95% CI: 0.358–0.976) intervention groups only in boys. The short- and long-term interventions resulted improvement in some of the MetS components in both genders.
Conclusions:
The healthy lifestyle intervention reduced the risk of MetS in both genders in short and long term, but with different patterns and improved some of the MetS components.
Introduction
M
Healthy lifestyle is the main key to weight control; therefore, interventions tackling unhealthy lifestyle behaviors are recommended for weight management and preventing MetS in the earlier years of life. 6 Unhealthy lifestyle behaviors, such as sedentary activities and high caloric foods, which mostly originate in childhood and adolescence, can continue into adulthood, 7 making the transitional period of adolescence a critical stage for implementing lifestyle interventions to improve eating habits and exercise patterns for a lifetime. 7 Considering the definitive role of obesity in the development of MetS in children and adolescents, 8 several lifestyle interventions in different countries have been designed to prevent or treat obesity. 9 Not many studies have been documented directly addressing MetS 6,7,10 –12 ; most of these had small sample sizes and were mostly limited to obese children as the secondary line of prevention. As multidisciplinary programs are increasingly being recommended to prevent childhood obesity and reduce cardiovascular risk factors, interventional studies, aimed at improving diet, physical activity or both, are conducted in home, school, the community, or combination of these settings. 13 Therefore, generalizability of the findings of most studies to other populations with different ethnicities, cultures, and lifestyles is debateable. 14 Similarly, in Iran, few studies have investigated the influence of physical activity and diet interventions aimed at curtailing metabolic risk factors in adolescents in the short and long term. 15 –17 We, therefore, aimed to investigate the effects of a 9-year community-based lifestyle intervention through both school and public programs on MetS and its components in Tehranian adolescents, aged 12–15 years.
Methods
Study design
This study, conducted within the framework of the TLGS, is mainly aimed at: (1) Determining the prevalence of noncommunicable diseases (NCDs) and their associated risk factors through a cross-sectional phase (1999–2001) followed by examinations at 3-year intervals; (2) Investigating the effects of healthy lifestyle education on NCD risk factors and outcomes. Briefly, as a controlled field trial, the TLGS is being conducted in one of the districts of Tehran with a homogenous population and approximately the same sociodemographic status. Using a multistage cluster randomized sampling, TLGS participants (15,005 individuals, 3 years of age and over) were recruited from three randomly selected healthcare centers, located in the study area; from among them a total of 5630 subjects under coverage of one of the three health centers, which was far from two other centers were considered for lifestyle modification to minimize the interference of intervention and control groups. The minimum and maximum distances between intervention and control groups were 1.5 and 5 km, respectively. Considering the distance among study areas, there was no difference in socioenvironmental conditions such as public transportation, which could affect the results of the intervention among control and intervention groups. More details on the rationale and design of the TLGS and also the healthy lifestyle intervention have been published elsewhere. 8,18
Study participants
Using the TLGS database (1999–2010) a total of 1403 adolescents, 12–15 years of age were recruited for the current analysis (in 2015). The following subjects were excluded: 173 (12.3%) for lack of precise residential address, 174 (12.4%) for lack of attendance in all three examinations carried out in the third, sixth, and ninth year after the baseline assessments, which have been defined as the short term, mid term, and long term in the current article. Eventually, 1056 individuals remained for study analysis and were assigned to the three following groups, based on their area of residence; 174 (16.4%) and 539 (51%) adolescents, residing in the intervention and control areas in all three examinations of study, were assigned to the complete intervention and control groups, respectively, and 343 (32.4%) adolescents, who did not always reside in either the intervention or control areas and were in transition between these two areas, were assigned to the incomplete intervention group (Fig. 1).
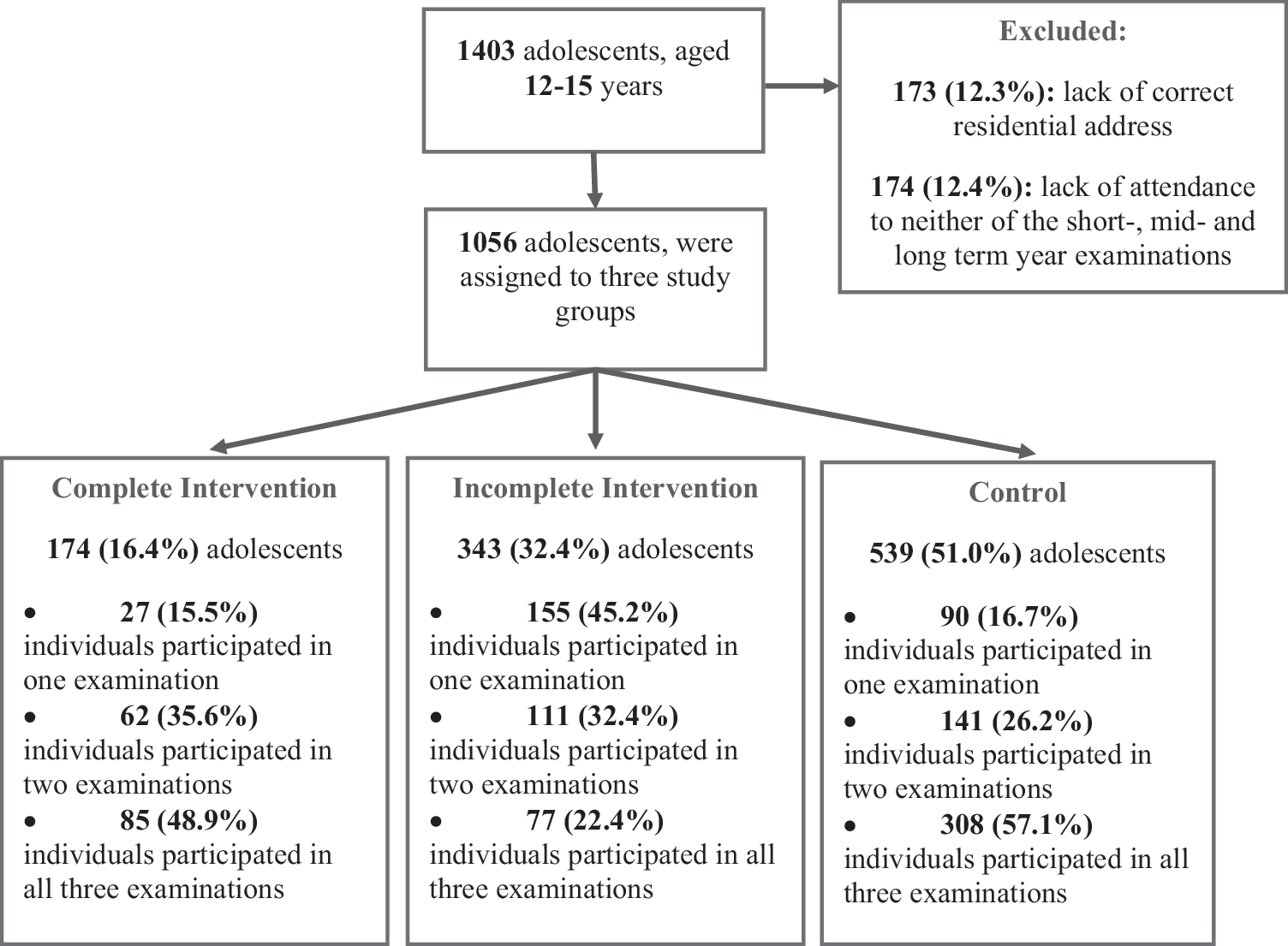
Trial flowchart. Short-term examination: 3 years after baseline; mid-term examination: 6 years after baseline; long-term examination: 9 years after baseline. Complete intervention and control: adolescents who lived in the intervention and control areas, respectively, during the short-, mid-, and long-term examinations; incomplete intervention: adolescents who did not completely reside in either of the areas (intervention or control) and were in transition between these two areas.
Measurements and definition
The design of TLGS has previously been published in detail. 8,18 Briefly, trained interviewers collected information, using a pretested questionnaire which included demographic data. Anthropometric indices, including weight, height, and waist circumference (WC), were measured using standard protocols. A qualified physician measured blood pressure twice with the individuals in a seated position after one initial measurement for determining peak inflation level using a standard mercury sphygmomanometer; the mean of the two measurements was considered to be the participant's blood pressure. Blood samples for the measurement of glucose and lipid concentrations were drawn after the individuals had fasted overnight; fasting blood glucose (FBG) was measured on the day of blood collection by the enzymatic colorimetric method using glucose oxidase; TG concentration was measured by commercially available enzymatic reagents (Pars Azmoon, Tehran, Iran) adapted to a Selectra autoanalyzer, and HDL-C was measured after precipitation of the apolipoprotein B-containing lipoproteins with phosphotungstic acid.
In adolescents, MetS was defined based on the Cook et al. criteria 19 as the presence of three or more of the following factors: (1) TG ≥110 mg/dL; (2) HDL-C <40 mg/dL; (3) WC ≥90th percentile for age and sex, according to national reference curves 20 ; (4) systolic blood pressure (SBP) and/or diastolic blood pressure (DBP) ≥90th percentile for sex, age, and height, from national reference cutoff points, 21 and (5) FBG ≥100 mg/dL. For individuals >18 years of age during follow-up, we used the criteria for MetS in adults, specified by the Joint Interim Statement (JIS) as the presence of any three of the following five risk factors: (1) abdominal obesity with a WC ≥90 cm for both genders, according to Iranian cutoff values 22 ; (2) reduced HDL-C <50 mg/dL in women and <40 in men or on drug treatment to reduce HDL-C; (3) elevated TG level ≥150 mg/dL or on drug treatment for elevated TG; (4) elevated blood pressure (≥130 mmHg SBP or ≥85 mmHg DBP) or on antihypertensive drug treatment, and (5) elevated FBG ≥100 mg/dL or on drug treatment for elevated glucose. 23
Lifestyle interventions
Design of the healthy lifestyle interventions in the TLGS has been published previously. 8 Generally, it aimed at primary prevention for NCDs and could be summarized in two categories: (1) school-based healthy lifestyle program and (2) public healthy lifestyle education. Detailed information of the intervention is available in the Appendix Table A1 of the current article and key aspects include promotion of healthy food choices and eating patterns, increasing physical activity and reducing sedentary behaviors, and tobacco use prohibition.
The sequence of the current intervention, which directly addressed adolescents, was conducted within the framework of school-based program and encompassed educational sessions for three groups: students, parents, and teachers. A total of 12 healthy lifestyle sessions (45 min each) have been held for the 1st grade students, which were followed with three reminding sessions for students of grades 2 and 3, in each educational year. For parents, three face-to-face educational sessions (60 min for each) were conducted for each grade. For teachers, 2-day seminars focusing on the knowledge and skills regarding healthy behaviors along with a 45-min class were held annually. To monitor school-based interventions (students, parents, and teachers) the number and duration of educational sessions as well as the number of participants were registered based on the study protocol. Public healthy lifestyle education, provided each family with face-to-face healthy lifestyle education and consultation in the healthcare center. All details of the number of participants and educational sessions and consultation were recorded by trained staff. Written materials, including health newsletters (paik-e tandorosti), pamphlets, brochures, and booklets were distributed two to four times a year to all families. The health officials were responsible to confirm whether written materials had been received by all families.
This study was funded by the Research Institute for Endocrine Sciences (RIES), Shahid Beheshti University of Medical Sciences and has been reviewed and approved by the Iranian registry of clinical trials (ISRCTN52588395), also by the Research Ethics Committee of the RIES, Shahid Beheshti University of Medical Sciences (No. EC 121). All participants gave written informed consent before beginning the study.
Statistical analyses
All analyses were split by sex in adolescents. Metabolic risk factors of adolescents at baseline were expressed as mean (SD) and compared among the three study groups, using one-way ANOVA. Adjusted prevalence of MetS in the short-term, mid-term, and long-term examinations was calculated using logistic regression analysis. To consider the potential intraindividual dependence of observations in this longitudinal study, generalized estimating equations (GEEs) with an exchangeable working correlation structure were performed. The GEE method focuses on changes in odds of MetS in the short-, mid- and long-term examinations and the impact of intervention. The most common research question is whether the treatment groups follow the same changes in the cardiometabolic risk factors over time. For illustrative purposes, follow-up time, treatment groups, and the interaction between follow-up time and treatment groups were included in the models. We have shown the results of this analysis, from the short- to the long-term examinations, as a graph of risk factor versus time. All GEE models were adjusted for age at each follow-up and baseline status of each metabolic parameter. Statistical analyses were performed using SPSS (version 16; SPSS, Inc., Chicago, IL) and software package STATA (version 12; STATA, Inc., College Station, TX), considering significance level at P < 0.05, and confidence interval (CI) as 95%.
Results
At baseline, in both genders, there was no significant difference in mean values for MetS components and the prevalence of MetS between controls and each intervention group, even after adjusting for age at the time of recruitment (Table 1).
Data are presented as mean ± SD or percent.
P value calculated using one-way ANOVA.
Short-term examination: 3 years after baseline; mid-term examination: 6 years after baseline; long-term examination: 9 years after baseline.
Complete intervention and control: adolescents who lived in the intervention and control areas, respectively, during the short-, mid-, and long-term examinations, incomplete intervention: adolescents who did not completely reside in either of the areas (intervention or control) and were in transition between these two areas.
DBP, diastolic blood pressure; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; Ln TG, natural logarithm transform of triglycerides; MetS, metabolic syndrome; SBP, systolic blood pressure; TG, triglycerides; WC, waist circumference.
After adjusting for age and baseline values, comparison of the prevalence of MetS between each of the intervention groups and the controls, showed significant decrease in boys who were placed in the incomplete (14.0 vs. 22.9, P = 0.034) and the complete groups (9.0 vs. 23.4, P = 0.031) in short and long term, respectively. In girls, compared with controls, the prevalence of MetS was significantly decreased in short term only in the complete intervention group (2.5 vs. 9.1, P = 0.06) (Fig. 2). Although the prevalence of MetS remained constant in girls through mid and long term, there were no significant differences among the three study groups.

MetS prevalence among study groups through the short-, mid- and long-term examinations. Short-term examination: 3 years after baseline; mid-term examination: 6 years after baseline; long-term examination: 9 years after baseline. Complete intervention and control: adolescents who dwelled in the intervention and control areas, respectively, during the short-, mid-, and long-term examinations; incomplete intervention: adolescents who did not completely reside in either of the areas (intervention or control) and were in transition between these two areas. MetS, metabolic syndrome.
Table 2 reports the estimated odds ratios (ORs) and 95% CIs from GEE logistic regression models for MetS, which were significantly decreased only in adolescent boys in the complete (OR: 0.516, 95% CI: 0.273–0.973, P = 0.04) and incomplete (OR: 0.591, 95% CI: 0.358–0.976, P = 0.04) intervention groups compared with controls. However, in girls, ORs were not significant for MetS among the groups studied.
Short-term examination: 3 years after baseline; mid-term examination: 6 years after baseline; long-term examination: 9 years after baseline.
Complete intervention and control: adolescents who lived in the intervention and control areas, respectively, during the short-, mid-, and long-term examinations; incomplete intervention: adolescents who did not completely reside in either of the areas (intervention or control) and were in transition between these two areas.
CI, confidence interval; OR, odds ratio.
The results of GEE analysis for MetS components are shown in Fig. 3. In the short term, the mean value of fasting plasma glucose (FPG) decreased in boys and girls in the complete intervention group (P = 0.014 and P = 0.081, respectively); however decrease in mean TG level was significant only in boys of the complete intervention group (P = 0.045). Furthermore, in girls of both intervention groups, a decreasing pattern was seen in mean SBP in the short term (P = 0.052, P = 0.057). In girls, while the mean HDL-C level declined in the complete and incomplete intervention groups in short term (P = 0.080 and P = 0.048, respectively), in the complete intervention group, it increased in the mid- and long-term assessments (P = 0.02, P = 0.029). A similar pattern was seen in mean HDL-C in boys, which was only significant in the incomplete intervention group in the mid-term assessment (P = 0.016).
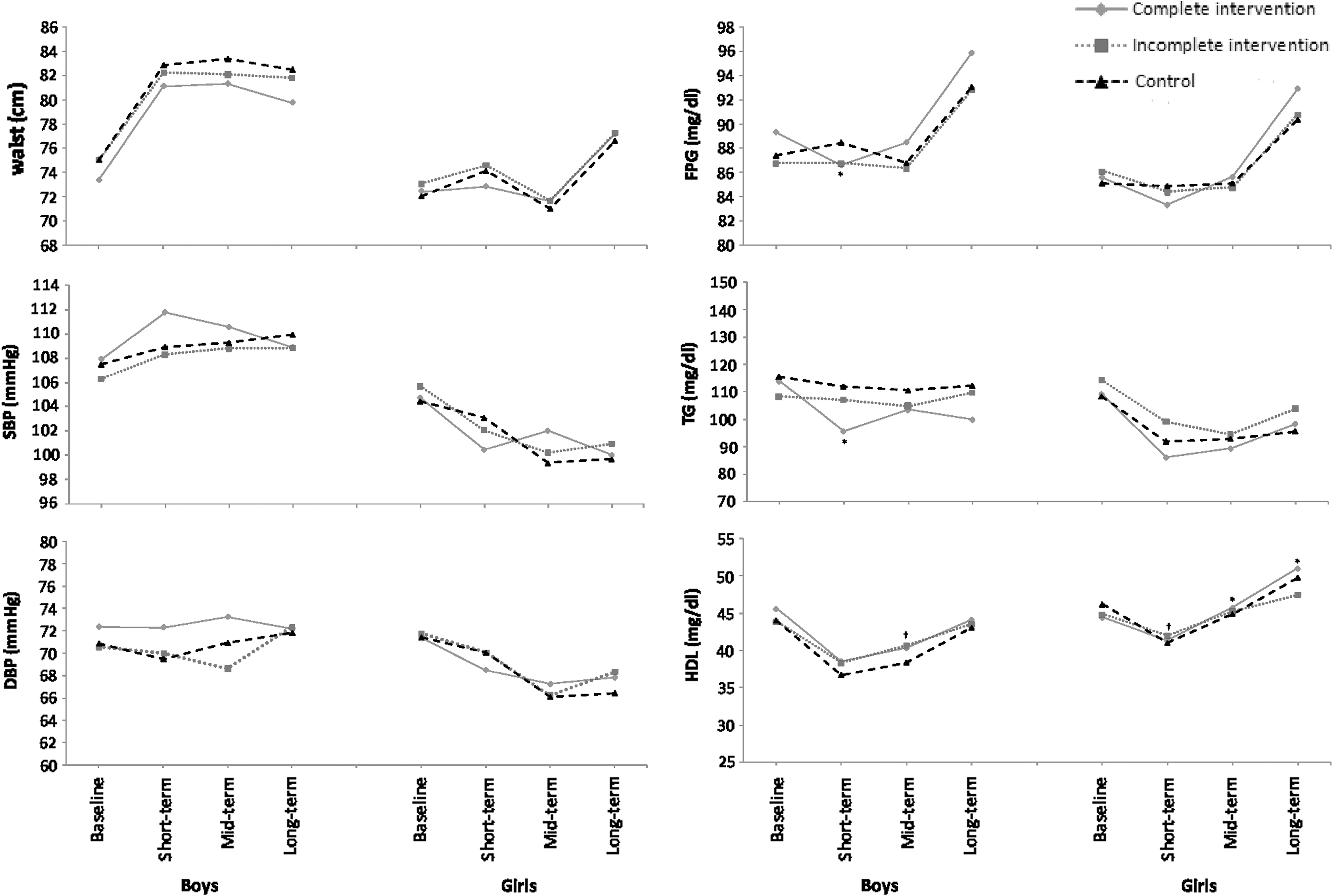
Changes of MetS components: marginal means among study groups through the short-, mid-, and long-term examinations: results of GEE analysis. Short-term examination: 3 years after baseline; mid-term examination: 6 years after baseline; long-term examination: 9 years after baseline. Complete intervention and control: adolescents who dwelled in the intervention and control areas, respectively, during the short-, mid-, and long-term examinations; incomplete intervention: adolescents who did not completely reside in either of the areas (intervention or control) and were in transition between these two areas. *P < 0.05, complete intervention compared to control group. † P < 0.05, incomplete intervention compared to control group. DBP, diastolic blood pressure; FPG, fasting plasma glucose; GEE, generalized estimating equation; HDL-C, high-density lipoprotein cholesterol; SBP, systolic blood pressure; TG, triglycerides; WC, waist circumference.
Discussion
Our findings show that short-term healthy lifestyle intervention resulted in a lower prevalence of MetS in girls and boys who participated in the program completely or incompletely. Over time, the intervention reduced the prevalence of MetS in boys, which resulted in a significant difference between controls and those who received complete long-term intervention. However, in girls the prevalence of MetS remained low and approximately similar in both the intervention and control groups, through both mid and long term. While boys in both intervention groups were less likely to have MetS through the study, no significant difference was observed between girls in intervention groups and controls in this regard.
Findings of the current study revealed that the lifestyle intervention decreased the prevalence of MetS in the short term in both genders, findings in line with those of previous lifestyle interventions, such as Obeldicks, 10 Bright Bodies, 12 and a number of other short-term intervention studies, which documented a positive change in the prevalence of MetS, although some deferred in terms of duration (2 months to 2 years). 6,7,11 The comparison of the prevalence of MetS between intervention and control groups showed that in girls, the intervention initiated its desired effects sooner and more intensely, resulting in a significantly lower prevalence of MetS in the intervention group after short term. Previous studies show that different body ideals for boys (muscular) and girls (thin), and different ages at which their body ideals change, could explain gender differences in the response to the related intervention. 24 Furthermore, studies have shown that girls in early adolescence are more influenced by the intervention and are also more knowledgeable about the topic of intervention than boys. 25
In the mid and long term, although boys had higher prevalence of MetS than girls in all three groups of the study, they had a lower risk of having MetS after receiving the complete or even incomplete intervention. On the other hand, the intervention succeeded in maintaining a constantly low prevalence for MetS in girls through mid term and long term in all study groups; a plausible explanation for this is the concurrent decrease in the prevalence of MetS in the control group during mid and long term, which could be attributed to factors other than education, such as being concerned about puberty changes, moving away from the thin ideal body, 24 and actively participating in physical exercises, 25 with a strong internal motivation to remain thin. There are limited studies investigating the impact of lifestyle interventions in the long term, and these mostly focus on the obesity prevention and metabolic outcome, not just MetS per se. 26 –28 Although short-term interventions may be more intensive and have a higher frequency and better adherence of participants, long-time follow-up is critical for evaluating the sustainability of each lifestyle intervention program. 29 While one meta-analysis pointed out that interventions of >1 year duration are more effective, 30 another revealed no significant difference in the effectiveness of studies of varying durations. 31
In the current study, improvements in the MetS components were mostly significant in the short term in the complete intervention group. Short-term evaluation of lipid profiles showed positive effects on TG in both genders, only significant in boys, and although constantly evident, not significant in the mid- and long-term assessments. Similarly, the “Crete” school-based healthy intervention 3,32,33 had a positive impact on TG in the short term and significantly improved total cholesterol and LDL after 3 years, improvements which remained after 6 and 10 years. In contrast, the “CATCH” program, 34,35 although successful in improving healthy habits in school-age children, could not influence lipid profiles after 2 years of school–home-based interventions and a 5 year follow-up. Furthermore, in the current study, positive short-term changes in mean SBP level occurred in girls, but were no longer evident in the mid and long term. Similarly, the “Know Your Body” program 36 conducted on 1st to 6th grade students, yielded an improvement in SBP and DBP levels after a 3-year follow-up, although not consistent after 5 years. Other studies reported some positive short-term effects on SBP and DBP, the “CHILDREN” study, 37 a 1-year healthy intervention in primary schools, and the “ENERGIZE” study, 38 a 2-year school-based obesity control program (with stronger effects on boys). Moreover, in the current study, a short-term decrease in the FPG mean level was seen in both genders, which was not seen in the mid- and long-term assessments. A plausible reason for the increasing trend in FPG in the mid- and long-term assessment is the decrease in insulin sensitivity during puberty and postpuberty related to gender and increasing body fat. 39
This is one of the first efforts to investigate the effects of a community-based multidisciplinary lifestyle intervention on MetS in Tehranian adolescents. The study has a comprehensive approach, which simultaneously targets schoolchildren, families, and school staff and focuses on all aspects of lifestyle behaviors (nutrition, physical activity, and smoking) concurrently. In the current study, the incomplete intervention group defined to compensate for the biased data of relocating families between the control and intervention regions. Other strengths include the considerable sample size, long-term intervention and follow-up and using the GEE method as a more efficient and unbiased analysis of longitudinal data, and repeated measures and time-varying variables. The present study, however, does have some limitations. Due to the large sample size, limited availability of validated tools and the long duration of interventions, it was not possible to assess the effect of lifestyle components (nutrition, physical activity, and smoking) separately and to distinguish the impact of each on the prevalence of MetS and its components. While we targeted diet and physical activity as the main lifestyle components, we failed to address other weight-related behaviors and barriers (such as body image, self-esteem, and motivation), which underlie food choice, exercise attendance, and long-time health outcomes. Future behavioral assessments are needed to evaluate the effects of each component of lifestyle intervention separately, in adolescents.
In conclusion, by implementing a community-based multidisciplinary healthy lifestyle intervention, the current study was successful in significantly reducing MetS prevalence in both genders in the short and long term, but with different patterns and to curtail a number of MetS components in female and male adolescents. Findings of the current study can enhance the development of more adjusted intervention programs and facilitate future health policy making.
Footnotes
Acknowledgments
The authors would like to thank the participants and the TLGS personnel for their collaboration. This study was financially supported by the Research Institute of Endocrine Sciences, Shahid Beheshti University Medical Sciences, and I.R. Iran. They would like to thank Ms. N. Shiva for critical editing of English grammar and syntax of the article.
Ethical Approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the Institutional and/or National Research Committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards and were approved by the Research Ethics Committee of the Research Institute for Endocrine Sciences (RIES), Shahid Beheshti University of Medical Sciences (No. EC 121).
Author Disclosure Statement
No conflicting financial interests exist.
| Intervention description | Intervention goals | |
|---|---|---|
| School-based lifestyle programs | ||
| Students | ||
| Classroom curriculum and practice | • Healthy lifestyle behavior classes per semester focusing on food values based on food pyramid, replacement of unhealthy food choices with healthy options, and the importance of daily physical activity. • “Tobacco-free lifestyle” classes during the first year of intervention covering topics such as prevalence of smoking, and short-term and long-term consequences of tobacco use. |
• Improving adolescents' knowledge, attitude, and behaviors regarding healthy dietary habits, appropriate physical activity, and avoiding smoking. • Motivating adolescents to modify their unhealthy behaviors. • Creating a supportive environment to encourage healthy behaviors among adolescents. • Reducing rate of NCDs in adolescents. |
| Peer teaching | • Involving students in program management by forming supervised student health teams. | |
| Policy modification | • Using red and green labels for selling unhealthy and healthy snacks, respectively. |
|
| Parents | ||
| Face-to-face education | • Face-to-face education per academic year focusing on healthy nutrition principles, appropriate physical activity, and avoiding smoking in adolescence. | |
| Written educational materials | • Pamphlets, bulletins, and posters for covering lifestyle modification issues, which were taught during face-to-face education program. | |
| Group discussions | Group discussion sessions per academic year focusing on: |
|
| Teachers | ||
| Face-to-face education | • Two-day seminar held by physicians and dietitians focusing on the knowledge and skills needed for volunteer teachers to modify unhealthy behaviors (nutrition, physical activity, and smoking) in adolescents; followed by a 45-min class per academic year to respond to teachers' questions about healthy behaviors, especially healthy dietary habits and appropriate physical activity in adolescents. | |
| Public healthy lifestyle programs | ||
| Face-to-face education | • Nutrition education classes in medical health centers held 4 days of week for an average of 12 adult participants, including face-to-face consultation; one-on-one interviews, education, and training; videos and slides. |
• Improving public knowledge, attitude, and behavior regarding healthy dietary habits, appropriate physical activity, and avoiding smoking. |
| Written education materials | • Health newsletter named “paik-e tandorosti” published every 3 months, containing healthy nutrition principles, appropriate physical activity, and avoiding smoking in adolescence. |
|
| Education by volunteer health workers | • Trained health workers called “the health liaisons” to appoint individuals and distribute written educational materials to families, schools, and mosques. | |
NCD, noncommunicable disease.