
Abstract
Background:
There are inconsistent results for the effectiveness of using smartphone applications (apps) or websites on weight loss. We investigated the efficacy of a smartphone intervention using a designated app that utilizes a lifestyle intervention-focused approach, including a human coaching element, toward weight loss in overweight or obese Korean adults.
Methods:
One hundred four adults aged 20–60 years with a body mass index ≥23 kg/m2, who signed up for a smartphone program for weight loss (using the Noom app), were recruited. Participants received an in-person orientation about the study and app use, and a baseline blood sample was obtained. The in-app intervention with daily behavior and nutrition education content and coaching lasted 15 weeks. The primary endpoint of the study was a change in weight. The secondary endpoints were changes in metabolic risk factors such as blood pressure, waist circumference, and glucose and lipid profiles. Body composition changes were also assessed, and body weight at 52 weeks was measured to ascertain long-term effects.
Results:
Participants showed a clinically significant weight loss effect of −7.5% at the end of the 15-week program (P < 0.001), and at a 52-week follow-up, a weight loss effect of −5.2% was maintained. At 15 weeks, percent body fat and visceral fat decreased by −6.0 ± 5.4% and −3.4 ± 2.7 kg, respectively (both P < 0.001). Fasting glucose level also decreased significantly by −5.7 ± 14.6 mg/dL at 15 weeks. Lipid parameters showed significant improvements, except for high-density lipoprotein cholesterol. The frequency of logging meals and exercise was associated with body fat loss.
Conclusions:
This advanced smartphone app was a useful tool to maintain weight loss in overweight or obese people.
Introduction
O
Since the 1990s, several drugs have been introduced for the management of obesity, but most have since been stopped in clinical practice because of a lack of efficacy and adverse side effects. 9 –11 Only a few drugs, such as orlistat, were available until 2015. More recently, four new antiobesity drugs have been approved by the U.S. Food and Drug Administration (FDA): lorcaserin, phentermine/topiramate, naltrexone/bupropion, and high-dose liraglutide. 12 However, the long-term efficacy and safety of these drugs have yet to be confirmed. To date, the gold standard of obesity treatment is intensive lifestyle modification. 13 Healthy lifestyle recommendations consist of decreasing caloric intake and increasing physical activity. One study demonstrated that a 1-year intensive lifestyle intervention decreased body weight by between 7% and 10% of participants' baseline weight. 14 Another study utilized a 12-week intervention with coaching over the phone, a formula/low-carbohydrate diet, and glucose self-monitoring for patients with type 2 diabetes. 15 The intervention achieved significantly improved glycemic control, and weight and blood pressure compared with controls at 26 and 52 weeks. 15 A previous meta-analysis revealed that a lifestyle intervention yielded significant initial weight loss, but weight was regained after 1 year. 16 Thus, while an initial weight loss can be successful in obese subjects, it can be very difficult to maintain this loss in the long term. Therefore, adherence to treatment is more important than any initial weight loss. 17
In this context, self-monitoring of dietary intake and exercise are effective for reducing body weight and improving adherence to advised lifestyle changes. 18 There are various self-monitoring systems, including simple self-assessment, Internet, or smartphone applications (apps), for this purpose. Among them, a smartphone app conjoined with a designated website is considered the most effective method because of its convenience and accessibility. 19 Several recent studies showed that smartphone apps were effective for weight loss. 18,20 One study demonstrated that an interactive intervention, including logging on to a designated website and receiving an individualized calorie-restricted diet, is effective for lifestyle improvement. 21 However, some studies did not prove the benefits of using a smartphone app compared with conventional approaches. 22,23 The inconsistent results from these prior studies might result from differences between the apps used or the study subjects that were enrolled.
Among the currently available smartphone apps, Noom® (Noom, Inc., Seoul, Korea) is one of the most popular, with over 45 million users worldwide (accessed June 2017). In a previous study, the Noom app received the highest scores in quality assessment compared with other smartphone apps. 24 The quality assessment included accountability, scientific coverage and content accuracy, technology-enhanced features, usability, and incorporation of behavior change techniques. In this study, we investigated the preliminary efficacy of a smartphone intervention for weight loss using the Noom smartphone app in overweight or obese Korean adults.
Subjects and Methods
Weight loss program participants
One hundred twenty adults from 11 corporations, aged 20–60 years, who underwent a medical checkup by Seoul Metropolitan City Government and Life Insurance Foundation (LIF) (Seoul, South Korea), were recruited. Each person provided written consent to participate in the study and signed up for Noom's weight loss program. Among them, participants with a BMI ≥23 kg/m2 (n = 104) were included. The 15-week intervention took place from March 2015 to July 2015. The study protocol was approved by the ethics committee of Seoul National University Bundang Hospital (SNUBH IRB#B-1608/359-106).
Matched controls
The weight loss program group was compared at 15 and 52 weeks from baseline with a noncoached control group that did not receive the weight loss curriculum. This gender-, age-, weight-, and height-matched group of Korean adults comprised 55 men and women (Table 1). Control data were obtained from Korean Noom app users of a standard free program that does not include coaching or a structured curriculum and is demographically similar to the experimental group. All participants consented to participation in the study by accepting the IRB-approved Research Policy and Terms and Conditions of the app. Therefore, data were available for an equal number of weeks as the experimental group.
Data are expressed as the mean ± SD. P values were calculated by Student's t-test for continuous data and chi-squared test for categorical data.
BMI, body mass index; C, cholesterol; DBP, diastolic blood pressure; FPG, fasting plasma glucose; HDL, high-density lipoprotein; LDL, low-density lipoprotein; NS, not significant; SBP, systolic blood pressure; SD, standard deviation; WC, waist circumference.
Measurement of anthropometric and biochemical parameters
Height (in centimeters) and weight (in kilograms) were measured by standard protocols at baseline and at weeks 6, 10, 15, and 52. The BMI was calculated by dividing body weight (in kg) by the square of the height (m2). Waist circumference was measured at the midpoint between the lateral iliac crest and the lowest rib. Blood pressure was measured with an automatic blood pressure measurement device. Body composition, including whole body fat mass, fat percentage, and visceral fat mass, was estimated using a portable bioelectrical impedance analysis device (InBody H20B; InBody, Seoul, South Korea). After a 12-hr overnight fast, blood samples were obtained in the morning. Fasting plasma concentrations of glucose, total cholesterol, triglycerides, high-density lipoprotein (HDL) cholesterol, and low-density lipoprotein cholesterol were measured on an automatic chemistry analyzer. These anthropometric and laboratory parameters were measured at baseline and after intervention at 15 weeks.
Offline intervention
Before study initiation, participants were involved in a 1-hr offline orientation session about how to use the Noom app and the curriculum throughout 15 weeks. Seoul Metropolitan City Government, LIF, and Noom, Inc. organized kick-off and wrap-up events during which a blood sample of each participant was collected. During the study, participants were provided with two offline education sessions about nutrition and physical activity.
Smartphone intervention
Participants were instructed to use Noom's food and exercise logging, and group and private message functions during the 15 weeks at no cost. The Noom Health app provided automated feedback based on calorie density when the participants logged their meals. A human coach provided by Noom was involved to empower participants to use the app easily and to engage each group. The coach provided weekly missions to the group designed to keep participants motivated and increase their activities such as food logging, cooking healthy recipes, and increasing physical activity.
Rewards
Rewards were provided to the participants based on their activity and outcomes. Coffee coupons worth $3 to $5 were provided to the participants who successfully completed weekly missions. Financial rewards after week 15 were given based on personal and group outcomes.
Study endpoints
The primary endpoint of the study was any change in weight after 15 weeks. The secondary endpoints were changes in metabolic syndrome risk factors such as blood pressure, waist circumference, and glucose and lipid parameters. Body composition changes from baseline to 15 weeks were also assessed. Change in weight at 52 weeks was assessed as the secondary endpoint to ascertain the long-term effect of the intervention.
Statistical analysis
Descriptive statistics [means ± standard deviations (SDs)] were calculated for subject baseline characteristics. Adjusted mean changes in weight up to 52 weeks, body composition, and biometric variables up to 15 weeks were obtained through linear mixed-effects models (LMMs) accounting for repeated measures and missing data. Models were fit accounting for sex and time point from baseline to 15 weeks for biometric variables, baseline and 6, 10, 15, and 52 weeks for weight change, and baseline and 6, 10, and 15 weeks for body composition change variables. LMMs were also used to evaluate the mean weight loss between the intervention group and controls. Multiple linear regression analyses were used to examine whether engagement variables predicted body composition change at 6 and 15 weeks, weight change up to 52 weeks, and all body composition variables (body fat, visceral fat, and fat-free mass) at 6 and 15 weeks, controlling for age and sex. Significance tests were two-sided with significance assumed at P < 0.05; Bonferroni corrections for multiple testing significance at P < 0.0036 or P < 0.008 are indicated in the Tables. Statistical analyses were performed using Minitab (version 17.0;
Results
Baseline characteristics of the study subjects
The demographic and clinical characteristics of the study population and matched controls are presented in Table 1. The mean ± SD age and BMI of the subjects in the intervention group were 38.7 ± 8.4 years and 28.7 ± 3.3 kg/m2, respectively. Fasting plasma glucose levels were 104.4 ± 21.2 mg/dL, and body fat percent estimated using bioelectrical impedance method was 32.9 ± 5.8%. In terms of app activities, the mean number of logs recording meals and exercise over 15 weeks was 232.4 ± 89.5 and 38.6 ± 40.8, respectively. No differences in baseline characteristics were observed between the intervention participants and matched controls.
Change in body weight during study period
Mean body weight decreased significantly by 4.7 kg between baseline and 6 weeks and by 6.5 kg between baseline and 15 weeks (both P < 0.001). Weight loss was sustained over time, and at 52 weeks, body weight was not different to that at 6 weeks, but remained significantly lower than that at baseline (−4.4 ± 5.4 kg; P < 0.001) (Table 2 and Fig. 1).
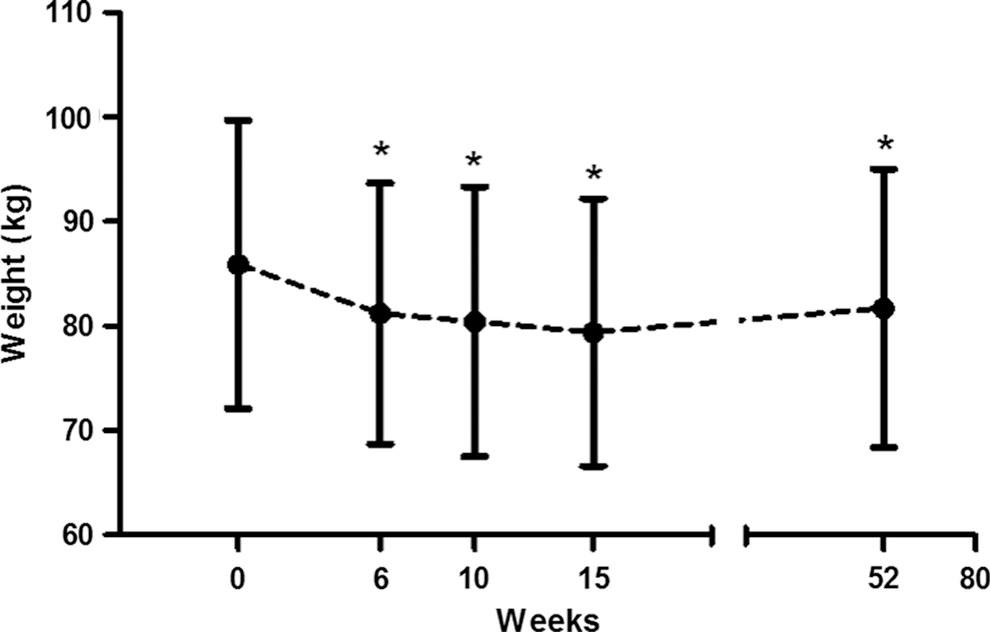
Change in body weight from baseline to 1 year. *Bonferroni correction set P < 0.0036 by linear mixed models.
Data are expressed as adjusted means from linear mixed models (SE).
Bonferroni correction significant at P < 0.0036.
n = 88, b n = 55, c n = 8, d P < 0.001.
SE, standard error.
Compared with the matched controls, the intervention group achieved 4.28 kg more weight loss at 15 weeks. At 52 weeks, the intervention group achieved 5.63 kg more weight loss compared with the control subjects, who gained 1.23 kg (Table 2 and Fig. 2).
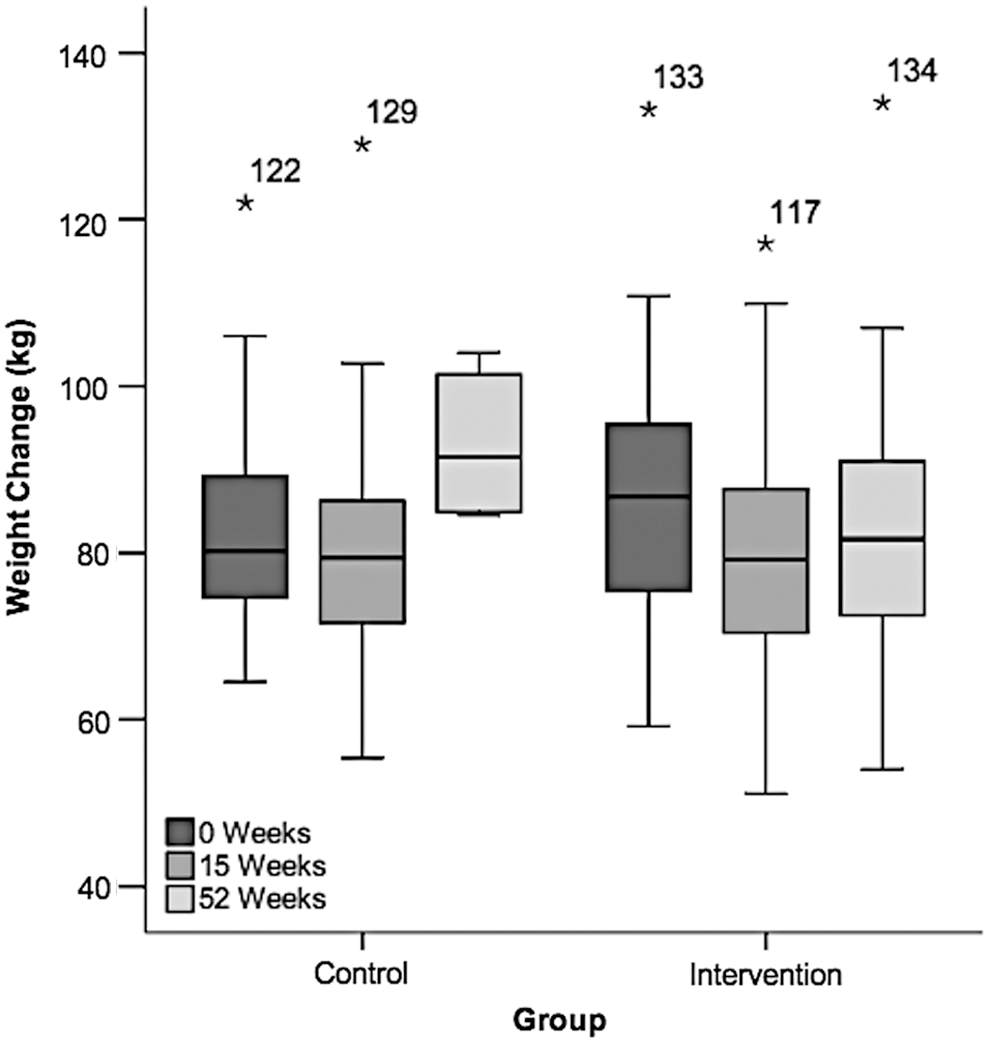
Boxplot showing the median, upper and lower quartiles, and outliers (*) for weight change from baseline to 15 and 52 weeks between the control and the intervention group. The control group presented weight gain above baseline at 52 weeks, while the intervention group maintained their weight loss at 52 weeks and remained significantly below baseline weight.
Changes in various parameters after intervention
Changes in body composition and other metabolic risk factors from baseline to 15 weeks are presented in Table 2. The percentages of body fat and visceral fat continued to decrease at 15 weeks (−6.0 ± 5.4% and −3.4 ± 2.7 kg, respectively, both P < 0.001). Fat-free mass decreased nonsignificantly at 10 weeks and increased at 15 weeks (0.2 ± 1.5 kg; P = 0.172). Fasting plasma glucose levels decreased at 15 weeks compared with the baseline value (−5.7 ± 14.6 mg/dL; P < 0.001). Lipid parameters, except HDL-cholesterol and triglycerides, showed significant improvements after intervention.
In-app activities and changes in weight and body composition
Multiple linear regression analyses, controlling for age and gender, were used to examine the association of in-app activities, including meal and exercise logging, total articles read, and group activities, with change in weight and body composition at weeks 6 and 15 (Table 3). Being male was associated with weight loss at week 6 (β = 2.461; P < 0.001) and among in-app actions, only the total number of articles read predicted weight loss at the same time point (β = 0.010; P = 0.020). At week 15, gender and the number of articles read showed significant effects as in week 6. In-app actions at 1 year did not predict weight loss, but being male continued to be a significant predictor of weight increase (β = 3.417; P = 0.003). The percentage of body fat loss was also associated with gender (β = 1.034; P = 0.025) at week 6. Furthermore, percent body fat loss was predicted by in-app meal logging at week 6 (β = 0.008; P = 0.016). At week 15, the logged incidence of exercise activity was the main predictor of percentage body fat loss (β = 0.046; P = 0.008) and the number of meals logged was marginally significant (β = 0.012; P = 0.061). The fat-free mass change was explained by group activity at week 15 and visceral fat change was associated with reading articles at week 15 (β = 0.003; P = 0.032 and β = 0.008; P = 0.015, respectively) (Table 4).
In-app activities and changes in metabolic syndrome risk factors
We also performed multiple regression analyses to examine in-app behavior in the prediction of changes in metabolic syndrome risk factors (Table 5). Age was associated with an increase in HDL-cholesterol levels (β = −0.173; P = 0.044) and being male was associated with a decrease in waist circumference (β = 4.954; P < 0.001). However, changes in metabolic syndrome risk factor were not explained by the models, including in-app actions.
Changes in metabolic syndrome risk factors
Figure 3 shows the decrease in the number of participants with several metabolic syndrome risk factors. Thirty-four percent of the subjects with elevated blood pressure at baseline achieved normal values after intervention. Waist circumference was reduced to normal values in 53% of the participants. Blood glucose level decreased in 24% of the participants with high blood glucose initially. Twenty percent of those with elevated triglyceride levels achieved normal levels and 32% achieved normal HDL-cholesterol values. Overall, the participants who were diagnosed with metabolic syndrome decreased by 50%.

Changes in the prevalence of metabolic syndrome and its components after 15 weeks of intervention. *P < 0.008 (after Bonferroni correction) by chi-squared tests between baseline and after intervention.
Discussion
In this study, a 15-week behavioral smartphone weight loss intervention with coaching for overweight or obese adults showed clinically significant weight loss effects (5.5% at 6 weeks and 7.5% at 15 weeks). Furthermore, after the intervention ended, weight loss was maintained at 1 year (5.2%), which was similar to the weight loss at 6 weeks. This weight loss was significantly higher at 15 and 52 weeks compared with matched controls. Regarding in-app activities, meal logging predicted the body fat loss at 6 weeks, while exercise logging was associated with body fat loss at 15 weeks.
Previous studies have demonstrated significant weight loss and long-term maintenance after lifestyle intervention. 25 –27 One weight loss maintenance study included 1032 overweight and obese adults who had previously lost at least 4 kg body weight during a 6-month intervention program. 25 Subsequently, subjects were assigned randomly to an interactive technology-based intervention or self-directed control. The study showed that 30 months after the weight loss intervention, the group randomized to continued contact and an interactive technology-based follow-up had regained less weight than the self-directed group, with a difference of 1.2 kg. The participants in our study maintained more than 4 kg weight loss relative to baseline and 5.6 kg compared with matched controls, who gained 1.23 kg at 1 year. This result supports the implementation of long-term follow-up with coaching for maintaining significant weight loss.
Change in body composition is another important aspect of weight loss; total body fat and its distribution are associated with metabolic syndrome. 28 –30 In our study, the percentage of body fat decreased significantly at weeks 6 and 15 (−3.3% and −6.0%, respectively) as did visceral fat (−2.3 and −3.4 kg, respectively). It is well known that visceral obesity is associated with a higher risk of metabolic syndrome. 31 Furthermore, a loss in fat-free mass is known to be associated with poor metabolic health and loss of normal body function. 32,33 In our study, there were small losses in fat-free mass at weeks 6 and 10, but small increases at week 15, although weight loss and percentage body fat loss continued to decrease. Physical activity supports improvements in fat-free mass and body fat loss; thus, long-term monitoring and supporting adherence to healthy behaviors such as exercising are important for maintaining decreased fat mass and increased muscle mass. Furthermore, efforts to estimate body-composition changes in digitally assisted and in-person weight loss interventions are important to improve our understanding of weight change and metabolic health over time in such interventions.
The clinical implication of this study is that the participants' metabolic syndrome risk factors were controlled successfully by a smartphone app intervention, mainly with few in-person interventions. Many previous weight loss programs showed metabolic risk control over more than 6 months of intense offline interventions. 34,35 In one post hoc analysis of a 6-month randomized trial with 96 overweight or obese people, the users of an app for self-monitoring of physical activity increased their physical activity levels and had a significantly lower BMI than nonapp users. 18 Our group has also shown that a multidisciplinary smartphone healthcare system equipped with a rule engine for clinical decision support, and integrated with a physical activity-monitoring device and dietary feedback into a comprehensive package, was effective in achieving glycemic control without hypoglycemia in patients with diabetes. 36,37 Another recent study on subjects with multiple metabolic impairments showed that interactive web-based interventions on dietary intake, physical activity, and health-related quality of life (QOL) for 6 months improved physical activity, dietary habits, and QOL, 21 but they did not adopt a real-time feedback system using smartphone apps.
In contrast with previous studies, one of the key factors of our study was that both offline and smartphone app interventions were provided to participants. Furthermore, human coaching was available to the intervention group using the smartphone app. Studies evaluating digital interventions for weight loss have shown that a human coaching component is important in motivating adherence to intervention and in improving and maintaining weight loss. 38,39 The degree of coaching (e.g., professional, mentoring, or peer) was shown to impact the magnitude of weight loss, where those coached professionally lost weight more than the other groups. 40 In our study, all intervention participants received group motivation weekly from professional coaches to help improve engagement and adhere to newly learned behavior. Our results suggest a potential for smartphone weight loss intervention used as a scalable and cost-effective metabolic syndrome management tool.
Our study had some limitations. First, the number of subjects was relatively small. Second, there was no randomized control group in our study; however, data from an adequately matched control group were available and used for comparison in the analyses for weight loss at 15 and 52 weeks. Third, the duration of the study (15 weeks) was relatively short. However, body weight information was obtained at 1 year after the 15-week intervention.
In conclusion, a 15-week smartphone app focusing on weight loss with behavioral coaching in overweight or obese Korean adults compared with matched controls showed clinically significant weight loss, which was sustained up to 1 year. These data suggest that an advanced smartphone app with a sophisticated program that guides behavioral modification is a useful tool to maintain weight loss in overweight or obese people. Based on the findings of our study and others, we recommend longitudinal follow-up to assess long-term weight loss maintenance. A randomized controlled trial comparing the smartphone intervention with human coaching conditions with a control group receiving standardized care (physician-based usual care) would also shed light into the true efficacy of such smartphone app interventions for weight loss.
Footnotes
Acknowledgments
We would like to thank all participants for their contribution to this study. We also thank Kelsey Wuensch for her editorial assistance and Dr. David González Barreto at the University of Puerto Rico, Mayagüez, for his statistics guidance. The smartphone application was given to participants at no cost by Noom, Inc. (Seoul, South Korea). The company had no role in the study design, data collection, analysis, and article preparation or publication. The authors take full responsibility for the contents of this article.
Authors' Contribution
T.T.-R. wrote the article and conducted the data analyses. T.T.-R., D.-H.L., Y.K., A.M., T.J.O., K.M.K., H.C.J., and S.L. researched data and contributed to the experimental design and discussion. T.T.-R., Y.K., D.H.L., and S.L. drafted the article. All authors edited and revised the article and approved the final version. S.L. is responsible for the integrity of the work.
Author Disclosure Statement
T.T.-R., Y.K., and A.M. are employed by Noom, Inc. The other authors have no conflicts of interest.