
Abstract
Background:
Our prior study showed that patients with sleep disorders had poor blood pressure (BP), glycemic control, and more severe complications. Therefore, sleep is very important for diabetic control. Our work was to investigate whether individualized diabetes sleep education significantly improve sleep quality and glycemic control in type 2 diabetic patients who sleep after midnight and potential mechanism by a randomized parallel interventional study.
Methods:
T2D patients were randomly recruited to an intervention or control group. Patients received structured special diabetes sleep education program with 3-month follow-up. Pittsburg Sleep Quality Index (PSQI) was scored for each participant. Demographic data, HbA1c, biochemical, and some hormones were also examined. SPSS 13.0 was used for statistical analysis.
Results:
One hundred patients were approached, and 45 were enrolled into our trial. Eventually, 31 patients completed the study. Patients in the intervention group greatly improved their sleep hygiene. After intervention, PSQI scores were lowered significantly (−1.48 ± 0.88 vs. −0.51 ± 0.71, P < 0.001), as well as significant reduction of HbA1c (−1.5 ± 0.55 vs. −1.11 ± 0.47, P < 0.05). Fasting plasma glucose was also lowered significantly. Homeostasis model assessment of insulin resistance was reduced significantly (−1.29 ± 0.97 vs. 1.04 ± 0.91, P < 0.01). Serum concentrations for interleukin (IL)-6, cortisol, and ghrelin were decreased significantly. Ghrelin (coefficients −0.65, P < 0.001), cortisol (coefficients −0.38, P < 0.05), and IL-6 (coefficients 0.452, P < 0.05) were correlated with HbA1c improvement. The change of ghrelin was negatively associated with the improvement of HbA1c.
Conclusion:
Diabetes sleep education could improve sleep quality, better blood glucose and BP, and decrease insulin resistance through healthier sleep hygiene. Lower serum concentration of ghrelin might be partly involved in the reduction of HbA1c.
Introduction
A
Our prior study showed that patients with sleep disorders had poor blood pressure (BP) and glycemic control and more severe complications. 5 Other cross-sectional studies identified a higher risk of diabetes among people with sleep problems. 6 –8 Therefore, sleep appears to be important for diabetic control. To date, sleep education has been reported as an effective nonpharmacological intervention for workers with insomnia. 9 However, few studies have examined the efficacy of such education intervention in patients with type 2 diabetes.
In this study, we conducted a randomized parallel interventional study to investigate whether individualized diabetes sleep education significantly improves sleep quality and glycemic control in type 2 diabetic patients who fall asleep after midnight.
Research Design and Methods
Participants and study design
Between February and August 2014, a statement explaining the study procedure, a consent form, and Pittsburg Sleep Quality Index (PSQI) questionnaire were distributed to 100 inpatients with type 2 diabetes (1999, WHO). The inclusion criteria were as follows: (1) Age is from 18 to 70 years, (2) T2DM (WHO, 1999), (3) Sleep after midnight and Sleep duration below 6 hr accessed by PSQI, and (4) HbA1c >8%. Same glucose lowering medicines for participants were maintained during study period. Patients were excluded if they met one or more of the following criteria: (1) Type 1 diabetes (2) Below 18 years (3) Night shift work within 3 months (4) Jet lag within 1 month (5) Sleep apnea; Taking medication for insomnia; Mental disease; Serious acute and chronic complications, including renal and liver failure, cardiovascular diseases, diabetic peripheral neuropathy, diabetic foot, malignancy tumor; and Other endocrinological diseases, such as thyroid diseases (6) Language communication barrier (7) Alcoholism or addictive smoking history (8) Taking care of infants (9) Pregnancy or lactation (10) Hypoglycemia
Patients were randomly allocated to an intervention or control group. Diabetes sleep education, combined with conventional diabetes education, was provided for patients in intervention group, and only conventional diabetes education was provided for patients in control group with equal time. Conventional diabetes education included systematic lectures about the diabetes process, nutritional and exercise planning, glucose monitoring, and knowledge of complications and psychosocial issues. All patients also completed a questionnaire regarding their lifestyle. The follow-up period was 3 months. This study was approved by the Ethics Committees of Tianjin Medical University. The trial registration number is ChiCTR-TRC-13003906 on Chinese Clinical Trial Registry.
Intervention
The intervention group received a structured program provided by a team consisting of two trained educators, a diabetic specialist, and a sleep specialist. Part 1, Conventional diabetes education (three sessions, 30 min/session). Part 2, Lectures about relationship between Sleep problems and diabetes (two sessions, 30 min) composed of education on common sleep problems and how it can affect blood glucose and diabetic complications. Part 3, Modified F.E.R.R.E.T. behavioral approaches 10 (30 min) through in-depth interview to make individual guidance.
Sleep education was also based on Chinese Guidelines for prevention and treatment of insomnia, including: (1) Don't drink anything 30 min before bed, (2) Stay away from food and caffeine 3 hr before bed, (3) No alcohol or smoking 3 hr before bed, (4) No electronic media (e.g., iPods, TV watching) at least 30 min before bed, and (5) No exercise 3 hr before bed.
Measurements
Outcome
The main outcome was the difference of the changes in PSQI score before and after intervention between groups. The PSQI is a subjective measure that evaluates sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction over the 1-month period. Overall sleep quality is determined by calculating global PSQI score (0–21 points), with a score of 6 or more indicating poor sleep quality; the higher the score the poorer the quality.
The other main outcome was the difference of the changes in HbA1c between the two groups before and after intervention. HbA1c is a form of hemoglobin that is measured primarily to identify the average plasma glucose concentration over the previous 2–3 months before the measurement. HbA1c has been recognized as a gold criterion to evaluate the control level of blood glucose in diabetes and strongly associated with chronic diabetic complications. The level of HbA1c was examined by high performance liquid chromatography in our study.
The secondary outcome was the difference of the changes in BP, body mass index (BMI), homeostasis model assessment of insulin resistance (HOMA-IR), and the differences of the changes in the serum concentrations of fasting plasma glucose, leptin, ghrelin, high sensitivity C reactive protein (hsCRP), interleukin (IL)-6, tumor necrosis factor (TNF)-α, growth hormone, and cortisol between the two groups before–after intervention. The serum concentrations of leptin, ghrelin, IL-6, TNF-α, growth hormone, and cortisol were determined by ELISA kit, respectively.
Randomization
Random group assignments were performed using a simple randomization. A random number was generated using a computer by a research assistant who had no direct contact with the participants.
Statistical analysis
SPSS 13.0 was used for all analysis. All statistical tests were two sided, with a significance level set at 0.05. Student's t-test and χ2 test were used for the analysis of baseline data. Paired Student's t-test, χ2 test, and further covariance for continuous variables with baseline values set as the covariate were used to analyze the compliance and differences in changes of the parameters between groups. The baseline variables in ANCOVA included: For the change of HbA1c, we set age, duration of diabetes, and BMI at baseline as covariables, since patients with different age, duration, and BMI may influence the A1c control. For the change of PSQI, we set age, sex, duration of diabetes, BMI, and HbA1c at baseline as covariates to minimize the confounding effect. For the change of systolic BP (SBP), we set age, sex, duration of diabetes, BMI, and HbA1c at baseline as covariates. For the change of HOMA-IR, we set age, sex, duration of diabetes, BMI, HbA1c, and PSQI at baseline as covariates. For the change of hsCRP, we set age, sex, duration of diabetes, and BMI at baseline as covariates. For cortisol, ghrelin, and IL-6, we set age, sex, and BMI at baseline as covariates. The statistical power was increased after the adjustment of these baseline variables since these variables may influence the outcomes. Partial correlation and linear regression analysis were used to explore the correlation between the serum factors and HbA1c changes.
Results
Study population
We approached 100 inpatients at first, and only 45 patients were enrolled into our trial (other 55 patients did not agree to participate into the study after knowing the detail). All these 45 patients were randomly allocated to intervention (25) or control group (20). There were nine dropouts in the intervention group during the study period, including two who had business trip, five who refused intervention due to strict study principle, and two for unknown reason. Five dropped in control group, including three who underwent administrative relocation and two for unknown reason. Eventually, 31 patients (15 for control group, 16 for intervention group) completed the study (shown as Fig. 1).
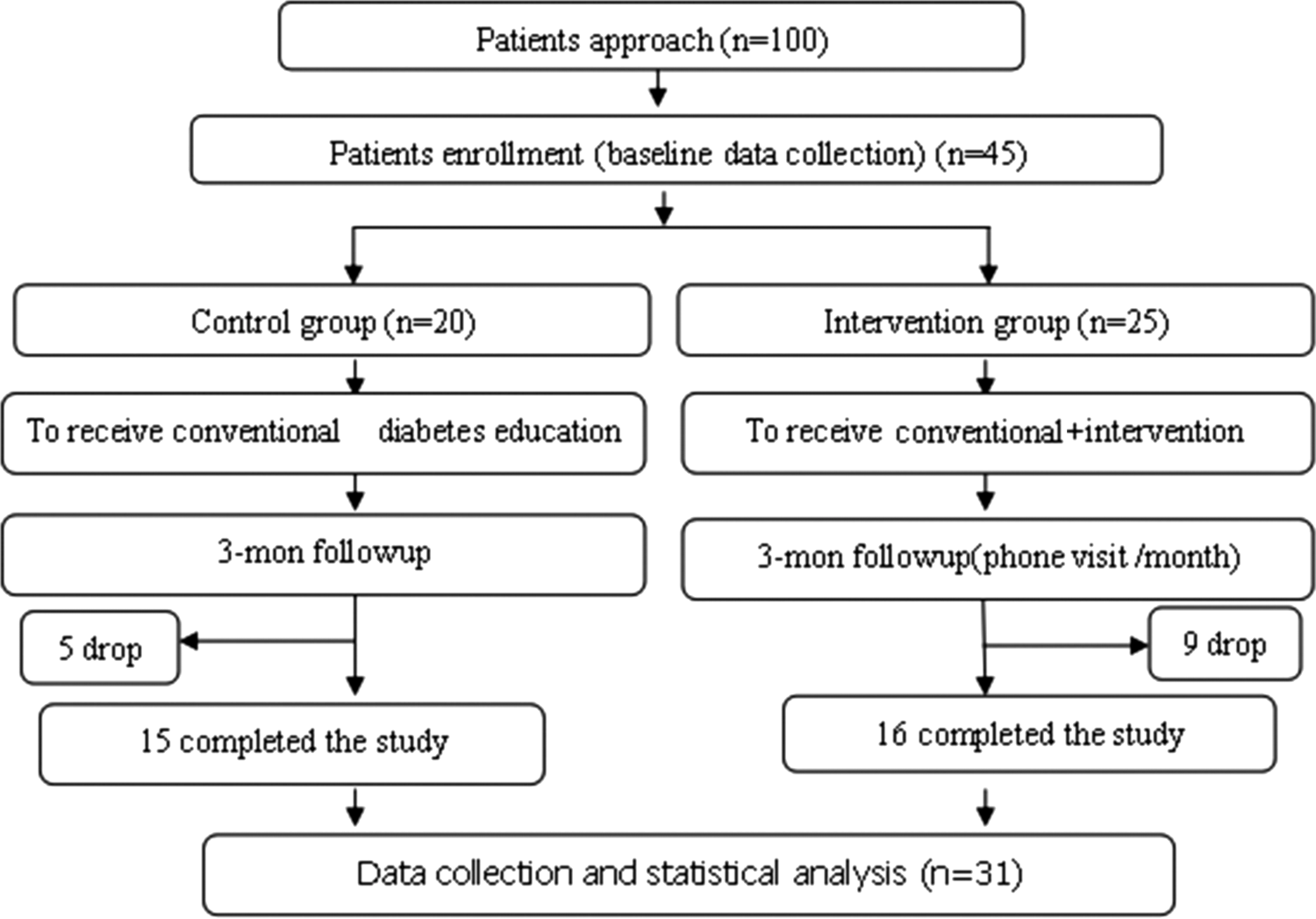
Flow diagram of the study. Forty-five patients from 100 approached inpatients were included into our trial (other 55 patients did not agree to participate in the study after knowing the details), followed by random allocation to intervention (25) and control group (20). Nine dropped in intervention group, including two who had business trip, five who refused intervention due to strict study principle, and two for unknown reason. Five dropped in control group, including three who underwent administrative relocation and two for unknown reason. Eventually, 31 patients (15 for control group and 16 for intervention group) completed the study.
Demographic characteristics
Baseline demographic characteristics of the patients are shown in Table 1. There were no differences in age, duration of diabetes and BP, and glucose control between the two groups. There were a large portion of overweight/obese patients in intervention group (11/16) and control group (13/15). Patients in both groups had poor glucose control and insulin resistance, although there was no statistical difference between the groups at baseline. Patients in both groups had poor sleep quality, since mean PSQI scores were higher than 6, based on the evaluation methods.
P > 0.05.
BMI, body mass index; DBP, diastolic blood pressure; FPG, fasting plasma glucose; HOMA-IR, homeostasis model assessment insulin resistance; PSQI, Pittsburg sleep quality index; SBP, systolic blood pressure.
Sleep hygiene at baseline
We investigated the sleep hygiene using self-made questionnaire at baseline, with no differences between groups (shown as Table 2). Definitions for items: if the binges happen in the dinner or night and the frequencies are more than thrice a week, we think binges will have most adverse effect on sleep. Therefore, we tick “yes” in the questionnaire as a sleep habit. When the length of time for the use of electronic devices was more than 1 hr, people's sleep will be affected obviously. Therefore, we tick “yes” as a sleep habit in the questionnaire. Most of patients in both groups had business binges (93.3% and 87.5%, respectively). Eighty percent of the patients in control group (12/15) used electronic devices for more than 1 hr before bedtime and 68.7% (11/16) for intervention group; 10 patients in the control group and 11 patients in the intervention group had coffee or smoke 3 hr before bed.
Serum concentrations of interested factors at baseline
We examined the serum concentrations of interested factors, including hsCRP, cortisol, IL-6, TNF-α, Ghrelin, growth factor, and leptin (shown as Table 3). There were no significant differences for all the factors between two groups (P > 0.05).
hsCRP, high sensitivity C reactive protein; IL, interleukin; TNF, tumor necrosis factor.
Change of sleep hygiene after intervention
We re-evaluated sleep hygiene for both groups after intervention. Numbers of patients who changed their behaviors are shown as Table 4. Great changes were seen through our diligent and determined efforts after 3 months. The percentage of attendance versus scheduled attendance to the clinic in intervention group is higher significantly (91.7% vs. 71.1%, P < 0.05). Patients in both groups changed their unhealthy sleep habit after education. For intervention group, eight patients decreased the frequencies of business binges from more than thrice a week to less than once a week. Nine patients discontinued the use of electronic devices for more than 1 hr before bed. Nine patients also ceased coffee or smoking 3 hr before bed. Two patients improved their sleep environment. For control group, we surprisingly observed slight improvement. Three patients cut out the business binges, and two patients did not use electronic devices. One patient quit smoking. The results above showed that after intervention, patients changed their habits significantly, especially by stopping electronic devices and stimulants before bed (P < 0.01).
P < 0.01.
Main outcomes after intervention
Variations in PSQI scores measured before and after intervention in two groups are shown as Table 5. Mean PSQI scores were decreased by 1.68 points in the intervention group and by 0.41 points in the control group, resulting in significant difference in variation of 1.27 between the groups, with the same pattern after adjustment for age, duration of diabetes, and BMI at baseline as covariates. Mean HbA1c was reduced by 1.62% in the intervention group and by 1.01% in the control group, resulting in significant difference in variation of 0.61% between groups, with the same significance after adjustment for age, duration of diabetes, and BMI.
Result from covariance analysis: age, sex, duration of diabetes, BMI, and HbA1c at baseline as covariates.
Result from covariance analysis: age, duration of diabetes, and BMI at baseline as covariates.
Secondary outcomes after intervention
Physical parameters, inflammatory factors, hormones, and adipokines were measured before and after the intervention (shown as Table 6). Change of BMI and HOMA-IR between groups after intervention was significantly decreased by 0.68 (kg/m2) and 0.45, respectively. For BP, SBP reduction between the two groups before–after intervention was significant, but not for diastolic BP. After adjustment for age, sex, duration of diabetes, BMI, and HbA1c, the significant difference disappeared. As for the examined inflammatory factors, we found significant decrease between the two groups in concentrations of hsCRP (by 2.96 mg/L) and IL-6 (by 4.46 ng/L), but no statistical difference for TNF-α. We also observed significant drop in serum concentration of cortisol (by 83.1 nM) and ghrelin (by 0.748 μg/L) between two groups after intervention, but no differences for growth factor and leptin. After adjustment for age, sex, duration of diabetes, and BMI, there was no difference between the two groups in hsCRP.
Result from covariance analysis: age, sex, duration of diabetes, BMI, and HbA1c at baseline as covariates.
Result from covariance analysis: age, sex, duration of diabetes, BMI, HbA1c, and PSQI at baseline as covariates.
Result from covariance analysis: age, sex, duration of diabetes, and BMI at baseline as covariates.
Result from covariance analysis: age, sex, duration of diabetes, and BMI at baseline as covariates.
Result from covariance analysis: age, sex, and BMI at baseline as covariates.
Result from covariance analysis: age, sex, and BMI at baseline as covariates.
Correlation and regression analysis
To investigate the relationship between change of HbA1c and other factors, we further run partial correlation and linear regression analysis (shown as Table 7). Results from partial correlation analysis indicated that change of serum IL-6 was positively correlated to HbA1c (r = 0.452, P < 0.05), and ghrelin and cortisol were negatively correlated to HbA1c (r = −0.6572, P < 0.001; r = −0.3824, P < 0.05) after adjustment for age, gender, BMI, and duration. Variation of serum ghrelin was the only factor, which was independently and negatively associated with HbA1c change from linear regression analysis. The regression model is ΔHbA1c = −1.472 – 0.658 × Δ ghrelin (R 2 = 0.433) (P = 0.000).
Controlling for age, gender, BMI, and duration.
P < 0.05, *** P < 0.001.
Discussion
The prevalence of diabetes has increased significantly in recent decades and is now reaching epidemic proportions in China. New therapies to fight diabetes emerge in large numbers as the rapid development of science and technology. But physicians and scientists are facing these embarrassing circumstances: target control rate for diabetes is not going up simultaneously as expected. We have to take other factors beyond medicines into account, such as patients' compliance, lifestyle, stress, and sleep. Numerous epidemiological studies have shown that sleep disturbances, including short sleep duration, sleep quality, and long sleep duration, have all been linked to poor health outcomes, increasing the risk of developing metabolic diseases and cardiovascular events. Beyond the duration of sleep, the timing of sleep may also have consequences. 11 Reutrakul et al. 12 analyzed 194 patients with type 2 diabetes and found the association of sleep timing (late evening sleep) with poorer glycemic control independent of sleep disturbances. These results drove us to conduct this trial to test systematic education as a potential complementary treatment. In this study, we targeted type 2 diabetes in those who sleep after midnight and provided structured and systematic diabetes sleep education program for 3 months. Our findings showed that sleep hygiene and sleep quality were greatly improved through intervention, and A1c level was significantly lowered. We also detected improvements in inflammatory markers and hormones, which may be of benefit toward improving glucose control.
To the best of our knowledge, this is the first prospective randomized controlled trial investigation exploring the effect of diabetes sleep education on type 2 diabetes patients who sleep after midnight, although the sample size was small. At the beginning of the study, 100 patients were approached. But most of them could not stand the strict study principles or could not stick to modified F.E.R.R.E.T. rules. Eventually, only 31 patients completed the study. Most studies about sleep and diabetes are cross-sectional. 7 In addition, we are the first to investigate the potential mechanism which could partly explain A1c change.
There may be several reasons why A1c decreased as a result of the intervention (shown as Fig. 2). First, we developed structured and systematic education programs for patients. Diabetes educators in this study were certificated and sophisticated for education and were fully trained by sleep specialists. Second, since study principles led to better lifestyle, patients' sleep habit (mainly stopping electronic devices and stimulants before bed) was greatly changed, leading to better sleep quality. In the study period, the investigators kept in close touch with patients, which made better adherence. Third, BMI reduction leads to decreased insulin resistance and increased insulin sensitivity. It is consistent with the previous study which shows that sleep participates in the regulation of body weight. 13 Therefore, we could have A1c reduced through our great efforts.
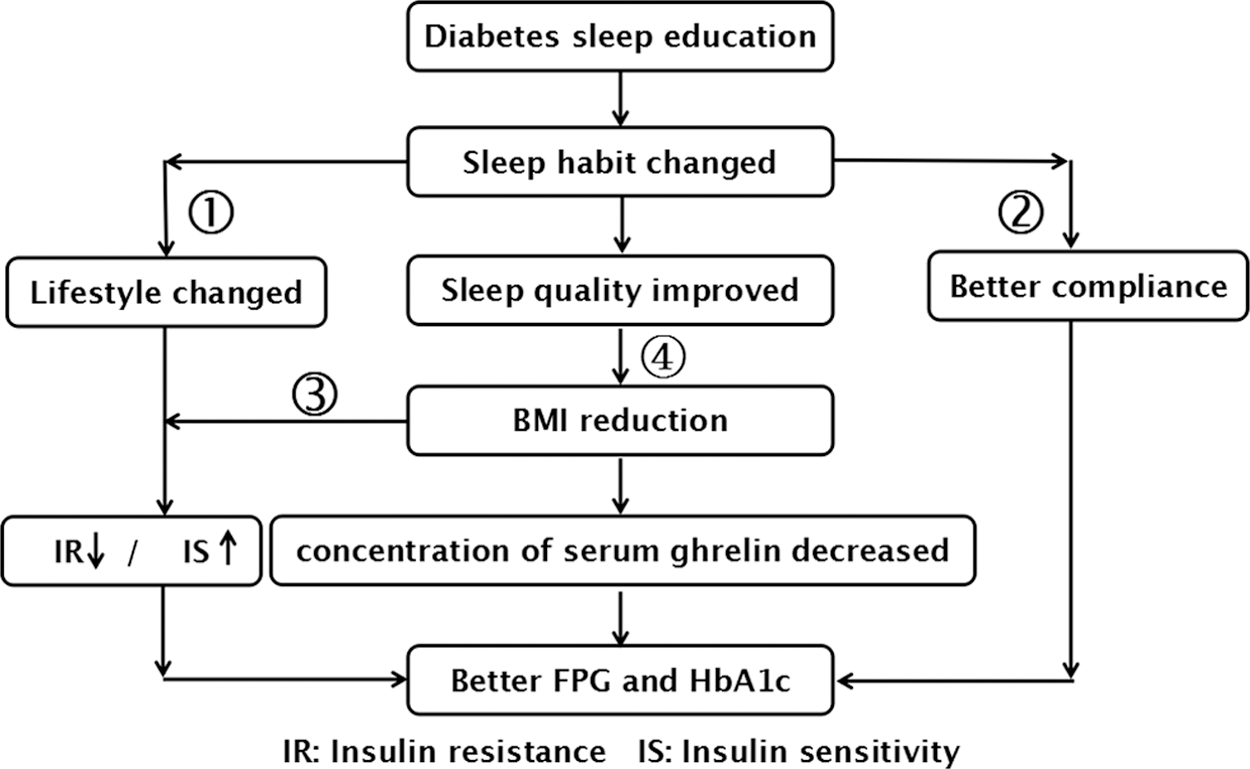
Explanation for A1c improvement. We figured that A1c improvement was contributed by the combination of the following factors. First, we developed structured and systematic education programs for patients. Diabetes educators in this study were certificated and sophisticated for education and were fully trained by sleep specialists. Second, since study principles led to better lifestyle, patients' sleep habits were greatly changed, leading to better sleep quality. In the study period, the investigators kept in close touch with patients, which made better adherence. Third, BMI reduction after intervention led to decreased insulin resistance and increased insulin sensitivity. It is consistent with previous study which shows that sleep participates in the regulation of body weight. Therefore, we could have A1c reduced through our great efforts. BMI, body mass index.
Briançon-Marjollet et al. 14 summarized current knowledge on the metabolic alterations associated with the most prevalent sleep disturbances and focused on various endocrine and molecular mechanisms underlying the associations among inadequate sleep quality, quantity and timing with impaired glucose tolerance, insulin resistance, and pancreatic β-cell dysfunction. The role of the hypothalamic-pituitary-adrenal axis, circadian pacemakers in peripheral tissues, adipose tissue metabolism, sympathetic nervous system activation, oxidative stress, and whole-body inflammation are main mechanisms. Park and Chung found that plasma levels of IL-1β, IL-6, IL-10, and TNF-α were significantly higher in the patient groups, with the high-disability group exhibiting the highest values (P ≤ 0.001). The plasma cytokine levels were significantly correlated with PSQI scores (P < 0.05). 15 In this study, we also examined factors involved in these pathways, including hsCRP, cortisol, growth factor, leptin, IL-6, TNF-α, and ghrelin. Our findings showed that after intervention, the serum concentrations of IL-6, cortisol, and ghrelin were significantly lowered as the decreased PSQI scores, even after adjustment for age, BMI, and sex. Furthermore, factor IL-6, cortisol, and ghrelin were correlated to A1c improvement. Recently, Sotos-Prieto et al. found significant inverse associations between healthy lifestyle score and IL-6 and TNF-α. 16 Therefore, we believe that modified lifestyle can improve sleep quality and A1c level.
Results from linear regression analysis showed that only ghrelin was negatively associated with HbA1c change. Ghrelin is a 28-amino acid peptide secreted mainly from the X/A-like cells of the stomach. Ghrelin is found in circulation in both des-acyl (dAG) and acyl (AG) forms. AG acts on the GH secretagogue receptor (GHSR) in the central nervous system to promote feeding and adiposity and also acts on GHSR in the pancreas to inhibit glucose-stimulated insulin secretion. Ghrelin, as part of molecular regulatory interface among energy metabolism, neuroendocrine, and neurodegenerative processes, takes part in lipid and glucose metabolism, in higher brain functions such as sleep–wake state, learning, and memory consolidation. It influences mitochondrial respiration and shows neuroprotective effect. Ghrelin is a potential therapeutic target for obesity and type 2 diabetes mellitus. 17 Sleep restriction compared with normal sleep significantly increases ghrelin levels. The increase in ghrelin is associated with higher consumption of calories. Elevated ghrelin may be a mechanism by which sleep loss leads to increased food intake and the development of obesity. 18
Several limitations in the present study warrant mention. First, this is a pilot study, and the drop rate is relatively higher compared to other study 19 due to some reasons as mentioned. In further study, patient compliance must be improved by more elaborative communication. Second, PSQI, used to assess the sleep quality, is a subjective criterion. It is better to use more accurate ways such as polysomnography in future study. Third, the study period is too short to minimize respondent burden. Fourth, the simple randomization method we used might have bias for randomization. Based on the size or confounding factors, more proper methods should be adopted in future. Finally, the hormone examinations were detected just before and after intervention, not for their rhythm.
Conclusion
In the present study, we conducted a randomized control trial involving type 2 diabetes in those who sleep after midnight, to explore whether or not diabetes sleep education significantly improves sleep quality and glucose control. We found that intervention by combined education (diabetes and sleep education) could greatly improve sleep quality, benefit glycemic control and SBP, and decrease the degree of insulin resistance, possibly partly due to the decrease of serum ghrelin. A RCT using more accurate approaches with longer study period and larger sample size should be considered.
Footnotes
Acknowledgments
The authors gratefully acknowledge the invaluable support from Prof. George L. King and Prof. Williams Hsu from Joslin Diabetes Center for project design and writing. Funding: This work was supported by Novo Nordisk, while Novo had no role in the design, analysis, or writing of this article. The work was also supported by National Science Foundation of China (Grant No. 81470187, 81273915, 81072922) and National Science Foundation for Young Scholars of China (Grant No. 81100596).
Authors' Contributions
Dr. Mingzhen Li contributed to carry it out, analyze the data, and write the article. Dr. Daiqing Li contributed to analyze the data and write the article. Dr. Yunzhao Tang, Lingling Meng, and Cuixiu Mao contributed to patient recruitment and to carry it out. Prof. Lirong Sun contributed to formulate research question. Prof. Baocheng Chang contributed to carry it out. Prof. Liming Chen contributed to formulate research question and study design.
Disclosure Statement
No conflicting financial interests exist.