
Abstract
Background and Aim:
Excess visceral fat accumulation results in altered release of adipokines. The aim of this study was to examine the relationship between new adipokines (omentin-1 and vaspin), insulin resistance, and serum inflammatory markers in obese subjects with metabolic syndrome (MS).
Patients and Methods:
The study included a total of 121 obese children (79 females and 42 males, aged 12–17 years old). The obese subjects were divided into two groups based on the presence or absence of MS criteria (MS group and non-MS group). Serum omentin-1, vaspin, and high-sensitivity C-reactive protein (CRP) were measured in addition to the other glucose metabolism parameters.
Results:
MS was diagnosed in 45 obese children and 76 children did not meet the MS criteria. Serum omentin-1 (289.5 ± 51.9 ng/mL vs. 268.2 ± 60 ng/mL, P = 0.03) levels were significantly lower in the MS group compared to the non-MS group. Serum vaspin levels (1058.3 ± 118 pg/mL vs. 1178.6 ± 158 pg/mL, P = 0.02) were higher in the MS group than the non-MS group. CRP levels correlated well with both the adipokines (r = −0.236, P = 0.04 for omentin-1 and r = 0.296, P = 0.008 for vaspin), although these adipokines did not show statistically significant correlations with fasting glucose–insulin levels, homeostasis model assessment of insulin resistance, and 2 hr postload glucose level.
Conclusions:
Higher vaspin and lower omentin-1 levels were determined in obese MS children compared to non-MS children and these adipokines were significantly correlated with high CRP values. These data support the view that adipokines in MS children contribute to increased inflammation markers before abnormal glucose metabolism.
Introduction
I
Omentin and vaspin have recently been discovered as visceral fat-specific secretory proteins and have been postulated to play a significant role in the relationship between human obesity and its related metabolic disorders such as nonalcoholic fatty liver disease, polycystic ovary syndrome, obstructive sleep apnea, and mental health disorders. 4 –6
Vaspin has been identified as an adipokine with insulin-sensitizing effects, which was discovered to be predominantly secreted from visceral adipose tissue in a rat model of type 2 diabetes. 7 The administration of vaspin to obese mice improved glucose tolerance and insulin sensitivity and led to the reversal of altered expression of insulin resistance. 8 Elevated serum vaspin concentrations have been shown to be correlated with obesity and impaired insulin sensitivity in adult studies. 9,10 Youn et al. have recently shown that vaspin mRNA expression in adipose tissue is related to parameters of obesity and glucose metabolism in adults. 9
Omentin-1, which is highly and selectively expressed in visceral adipose tissue, has been suggested to be an anti-inflammatory molecule and is thus assumed to have paracrine and autocrine roles in improving insulin sensitivity. 11 Moreover, recent clinical studies have focused on the influence of the novel adipokine omentin-1 on vascular health. In these studies, circulating omentin-1was seen to have a negative correlation with atherosclerotic parameters. 12,13 In human clinical studies, serum omentin-1 levels were found to be significantly decreased in metabolically unhealthy patients, such as those with MS and type 2 diabetes mellitus. 14,15
Excessive circulating glucose and triglycerides caused by an energy imbalance, lead to adipocyte hypertrophy and hyperplasia and consequently, various stresses and inflammatory processes develop within adipose tissue. Pediatric studies have shown that elevated C-reactive protein (CRP) levels correlate with cardiovascular risk factors, including adiposity and blood pressure, supporting the importance of inflammation in the early phases of atherosclerosis. 16,17 In the National Health and Nutrition Examination Survey data set, it was also confirmed that the CRP values in children with MS are elevated.
It has recently been suggested that new adipokines (omentin and vaspin) might have a strong relationship with obesity, insulin resistance, atherosclerosis, inflammation, and MS. Although adult studies have focused on the abnormal levels of vaspin and omentin in MS patients, particularly with reference to body mass index (BMI) and markers of insulin sensitivity, the regulation of these molecules and their relationship with other adipokines in pediatric obese patients have not been specifically studied. In this study, it was aimed to determine the levels of serum omentin-1 and vaspin levels in pubertal obese children diagnosed with MS and to make a comparison with age-matched obese children. In addition, an assessment was made of the relationships between these adipokines, CRP, and glucose metabolism parameters derived from fasting blood samples and oral glucose tolerance test (OGTT) measurements.
Materials and Methods
The study included 121 Turkish children (79 females and 42 males, ages 12–17 years) who presented at the Pediatric Endocrinology Outpatient Clinic of Konya Training and Research Hospital, and were diagnosed as obese. Two groups were formed based on the presence or absence of MS criteria defined in the International Diabetes Federation (IDF) consensus report (MS and non-MS groups). 18 Of the obese children, two were older than 16 years and so we used the percentiles that corresponding to the IDF recommendations used for older adolescents and adults (16+ years old) were used in these cases.
Patients with a BMI of ≥95th percentile according to reference curves for Turkish children and adolescents were accepted as obese. Waist circumferences were compared against healthy age-matched Turkish reference data. 19,20 The pubertal development stages were assessed by a single pediatric endocrinologist using the criteria of Tanner stages. Staging for sexual maturation was >2 in all patients (Tanner stages II–V). Children were excluded if they had a prior major illness, including type 1 or type 2 diabetes, took medications, or had a condition known to influence body composition, insulin action, or insulin secretion (e.g., glucocorticoid therapy, hypothyroidism, and Cushing's disease). The study was conducted in accordance with the Declaration of Helsinki, and the study was approved by the institutional review board (Konya Training and Research Hospital Ethics Committee). Informed consent was obtained from all the parents or legal guardians and their children.
Blood samples and insulin sensitivity index
Blood samples were drawn at admission and centrifuged at 2500g for 15 min at 4°C within 30 min of collection. The serum was stored at −80°C until analysis. Plasma insulin was measured using the IMMULITE immunoassay (IMMULITE Diagnostic Products Corporation, Los Angeles, CA). Plasma concentrations of total cholesterol, triglycerides, low-density lipoprotein cholesterol (LDL-cholesterol), and high-density lipoprotein cholesterol (HDL-cholesterol) were measured using routine enzymatic methods with an Olympus 2700 Analyzer (Olympus Diagnostica GmbH, Ireland). High-sensitivity CRP levels were measured with the latex-enhanced turbidimetric immunoassay (HiSensCRP LTIA, HBI Co., Ltd.), with an inter-assay coefficient of variation of 7.2%. Insulin resistance was defined as the levels of the homeostasis model assessment of insulin resistance (HOMA-IR) greater than 3.16. 21
Serum omentin-1 concentrations were measured with a sandwich enzyme-linked immunosorbent assay (ELISA; Immuno-Biological Laboratories CO., Ltd., Gunma, Japan), according to the manufacturer's instructions. Omentin assay sensitivity was 0.4 ng/mL and inter-assay and intra-assay coefficients of variation were <6% and <2.7%, respectively. Serum vaspin levels were determined by radioimmunoassay (Linco Research, St. Charles, MO). Vaspin assay sensitivity was 12 pg/mL and inter-assay and intra-assay coefficients of variation were <6% and <4%.
OGTT and definition of MS
Seventy five grams OGTT according to the American Diabetes Association criteria was performed in all subjects. Venous blood samples were obtained with venipuncture after overnight fasting at 0 and 120 min to measure serum glucose and insulin levels in the morning. The IDF definition of MS for children aged 10 years or older includes waist circumference ≥90th percentile for age and gender and the presence of two or more of the following findings: 1—Triglycerides ≥150 mg/dL; 2—HDL-cholesterol <40 mg/dL; 3—Systolic blood pressure ≥130 mmHg, diastolic ≥85 mmHg; and 4—Plasma glucose ≥5.6 mM or ≥100 mg/dL or known type 2 diabetes. 18
Statistical analysis
Statistical analyses were performed using SPSS version 21 software (SPSS, Chicago, IL). Data were expressed as mean ± standard deviation. Differences in the means of variables were tested using both parametric and nonparametric tests depending on the distribution of the variables. The strength of association between variables was calculated using Pearson's method for parametric variables and the Spearman Rho correlation test for nonparametric comparisons. A value of P > 0.05 was considered statistically significant.
Results
The clinical and biochemical characteristics of the study subjects are presented in Table 1. Of the total 121 obese children, 45 (37%) children were diagnosed with MS. All the subjects with normal glucose tolerance had fasting plasma glucose <5.6 mM and 2 hr postload plasma glucose <7.8 mM. Although there were no significant differences in some MS components such as systolic-diastolic blood pressure, total-cholesterol, HDL-cholesterol, LDL-cholesterol, aspartate transaminase (AST), and HbA1c levels, the major significant differences seen between the groups were age, BMI, triglycerides, fasting glucose–insulin level, 2 hr postload glucose–insulin level, HOMA-IR, alanine transaminase (ALT), and CRP. Serum CRP (4.2 ± 1.5 mg/L vs. 3.1 ± 4.7 mg/L, P = 0.04) levels were significantly higher in the MS group when compared to the non-MS group (Table 1). The MS obese group was subdivided according to their pubertal status as mid and late puberty. No significant difference was detected in parameters such as lipids, fasting glucose, fasting insulin, and HOMA-IR values (3.3 ± 2.5 vs. 4.2 ± 2.7; P = 0.08). This could have been due to relatively small number of cases identified as having MS-consistent criteria.
Data are given as mean ± SD, difference at P < 0.05 level.
ALT, alanine transaminase; AST, aspartate transaminase; BMI-SDS, body mass index-standard deviation score; hsCRP, high-sensitivity C-reactive protein; HDL-cholesterol, high-density lipoprotein cholesterol; HOMA-IR, homeostasis model assessment of insulin resistance; LDL-cholesterol, low-density lipoprotein cholesterol; MS, metabolic syndrome.
Serum omentin-1 (289.5 ± 51.9 ng/mL vs. 268.2 ± 60 ng/mL, P = 0.03) levels were lower in the MS group and vaspin levels (1058.3 ± 118 pg/mL vs. 1178.6 ± 158 pg/mL, P = 0.02) were significantly higher in the MS group when compared to the non-MS group (Table 1 and Fig. 1). Serum omentin-1 levels in the MS group were significantly associated with age, BMI, triglycerides (r = −0.276, P = 0.011), and CRP levels (r = −0.236, P = 0.04) (Table 2 and Fig. 2). The other metabolic parameters of total cholesterol, LDL-cholesterol, HDL-cholesterol, blood pressure, HOMA-IR, fasting glucose, and insulin levels were not significantly correlated with omentin-1 levels (Table 2). Serum vaspin levels were also significantly correlated with age, BMI, triglycerides (r = 0.235, P = 0.02), and CRP (r = 0.296, P = 0.008) in MS children (Table 2 and Fig. 2). Vaspin levels were not significantly correlated with the other metabolic parameters such as HDL-cholesterol, blood pressure, HOMA-IR, fasting glucose–insulin levels, and OGTT-derived measurements (Table 2).
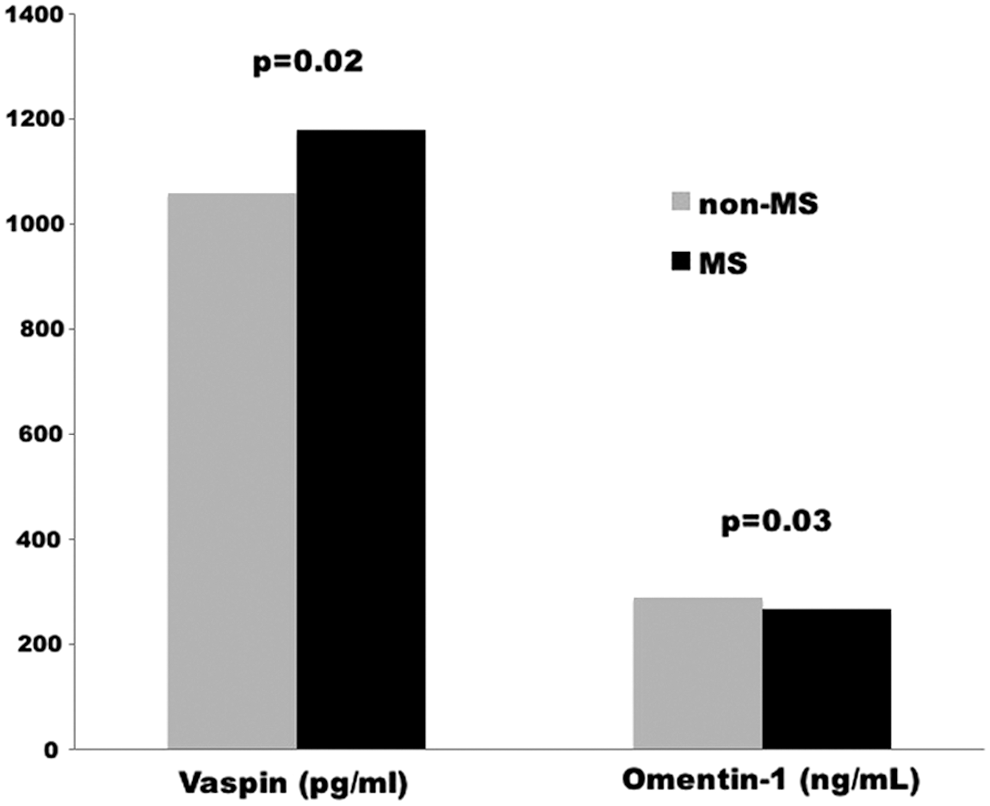
Comparison of serum vaspin and omentin-1 levels in MS and non-MS groups. MS, metabolic syndrome.
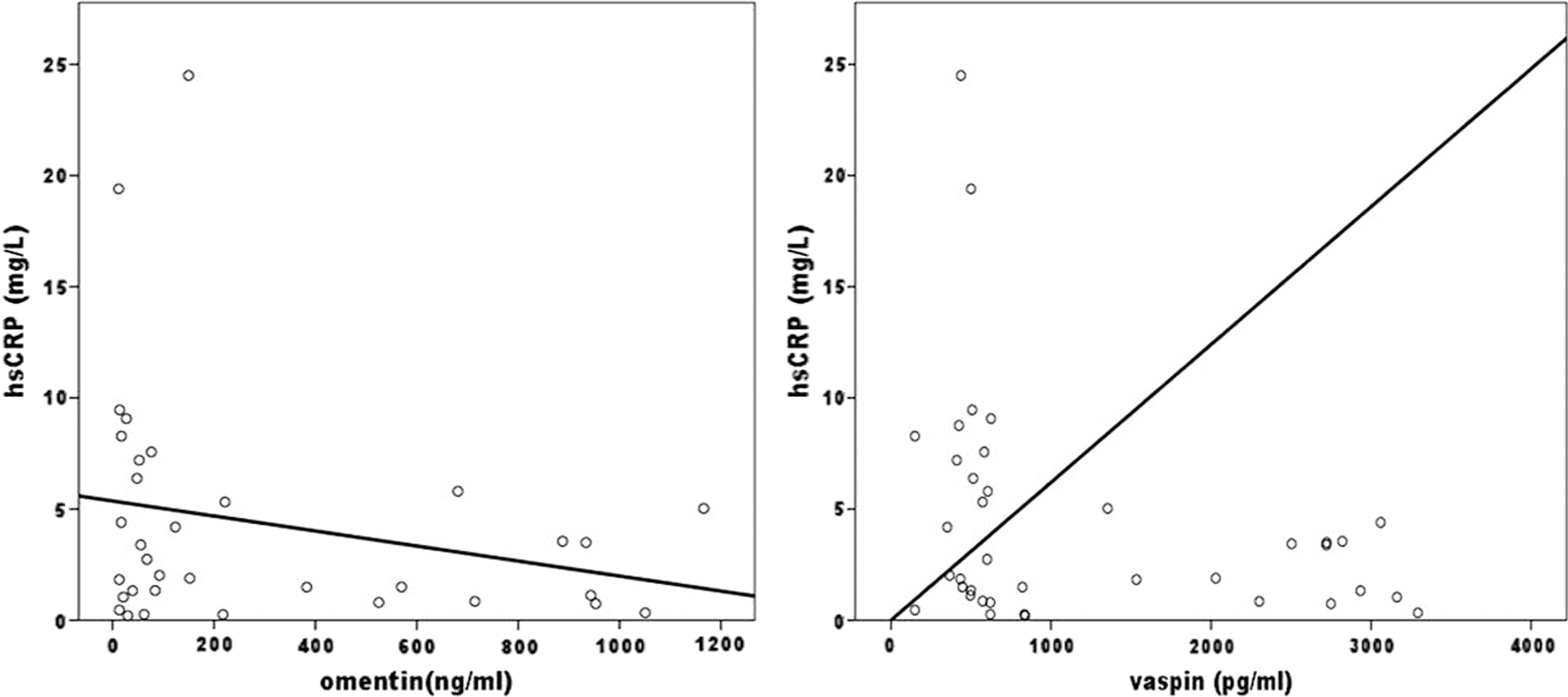
Correlations between CRP and serum omentin-1 (r = −0.236; P = 0.04) and vaspin levels (r = 0.296; P = 0.008) in MS children.
Discussion
A dysregulation of adipokines has been associated with obesity, type 2 diabetes, hypertension, inflammation, cardiovascular disease, and a series of pathological changes in a number of organs. Vaspin and omentin-1 have been defined as new adipokines and are thought to be associated with hyperinsulinemia, inflammation, and MS components. The main findings of this study were that vaspin levels were higher and omentin-1 levels were inversely lower in the obese MS group than in the non-MS children. It was also observed that omentin-vaspin-MetS relationships in obese children with MS are modulated by chronic inflammation indicated by CRP.
Adult studies have shown an association between elevated vaspin serum concentrations and obesity and impaired insulin sensitivity. A study by Choi et al. reported that plasma vaspin concentrations were correlated with BMI in males with MS compared to those without MS. 22 In cases of obesity and insulin resistance, the increase in unknown proteases is thought to be antagonized by a potential compensatory mechanism created by the increased vaspin level. 23 In this study, higher vaspin levels were determined in the group of obese MS children than in the non-MS subjects. However, the vaspin levels were independently correlated to CRP levels in the pubertal MS children, but not the glucose metabolism markers such as fasting glucose, HOMA-IR, and 2 hr postload. These data support that vaspin levels have not yet revealed any correlation to glucose metabolism in the pubertal period. In this study, serum adipokine levels were correlated with BMI, triglycerides, and systemic markers of inflammation, such as CRP at an early age before glucose metabolism. Several epidemiological studies have shown that circulating CRP, which is a known marker of chronic inflammation, is also an independent risk factor for type 2 diabetes mellitus, in addition to atherosclerotic heart diseases. 16,17 The data of this study indicated that obesity and these adipokines are closely associated with inflammation rather than glucose metabolism impairment in the pubertal period.
Several reports have shown that circulating omentin-1 in serum reflects its expression in visceral adipose tissue, which decreases in parallel with the increase of visceral obesity. 15,24 Yang et al. reported that omentin-1 enhances insulin-stimulated glucose uptake in human adipocytes and may regulate insulin sensitivity. 24 Furthermore, prolonged insulin–glucose infusion has been shown to lead to significantly decreased plasma omentin-1 levels in healthy individuals. 15 Moreno-Navarrete speculated that hyperinsulinemic conditions and peripheral adiposity may reduce omentin-1 production in morbidly obese subjects. 25 Similar to previous studies, in this study, circulating omentin-1 levels were significantly decreased in MS children compared with non-MS obese children. In adult studies, plasma omentin-1 levels have been reported to be inversely correlated with BMI, fat mass, triglycerides, and fasting plasma insulin, and positively correlated with insulin sensitivity, adiponectin, HDL-cholesterol, and endothelial function. 26 In this study, no association was observed between serum omentin levels and the development of MS components such as fasting glucose/insulin levels, HOMA-IR, and 2 hr postload glucose levels found in the pubertal period. Similiar to vaspin, omentin-1 had an association with CRP, but a negative correlation. These studied adipokines of vaspin and omentin-1, produced by adipose tissue in obese children, may have different and even conflicting roles in the anti-inflammatory effect. In a study of patients with newly diagnosed type 2 diabetes mellitus, Pan et al. suggested that in human endothelial cells, levels of CRP and tumor necrosis factor alpha-induced nuclear factor-kappa B activation were significantly decreased by omentin-1. 11 These studies suggest that omentin-1 may improve insulin resistance and suppress vascular inflammation. To the best of our knowledge, this study is the first to show a direct association between vaspin-omentin levels and an increased inflammatory state in obese children diagnosed with MS.
This study had some limitations, which will provide opportunities for future research. First was the lack of pubertal distribution of the subjects because of the small number of obese cases with MS. Second, as there was no nonobese control group, it was difficult to assess precisely the exact levels of adipokines. Third, there still remains an important variation of omentin-1 level assays. Fourth, there was no evaluation of lifestyle factors such as exercise and diet that may influence the level of adipokines. Despite these limitations, this study has established that statistically different levels of these adipokines were determined in obese children with MS and the non-MS obese group.
In conclusion, although elevated vaspin and decreased omentin levels were determined in obese children with diagnosed MS, no relationship was observed between serum levels of these adipokines examined and MS components. Serum omentin-1 had a negative correlation with BMI and a positive correlation with CRP levels in obese children with MS. Based on the findings of this study, vaspin and omentin-1 levels can be considered to be highly correlated to inflammation in obese children with MS rather than insulin resistance, lipids, and abnormal glucose metabolism.
Footnotes
Acknowledgment
This study was financially supported by Konya Training and Research Hospital, Konya, Turkey.
Author Disclosure Statement
No conflicting financial interests exist.