
Abstract
Background:
Although obesity is an independent risk factor for coronary artery disease (CAD), observational studies have found that persons with obesity have a better prognosis in established CAD compared with those with a normal body weight, suggesting that the underlying risk factors might differ between the two groups. In this study, we studied risk factors for CAD in persons with and without obesity in a Middle Eastern setting where obesity is endemic.
Methods:
Five hundred and fifty-six patients referred for elective coronary catheterization at Prince Hamza Hospital, Amman were included in a cross-sectional study. Patients with CAD (n = 353; 63.5%) were compared to patients with a normal coronary angiography (n = 203; 36.5%). Associations between CAD and baseline variables were assessed in multivariate logistic regression models.
Results:
In persons with obesity, male sex [adjusted odds ratio (AOR) = 2.62, 95% confidence interval (CI): 1.37–4.99], increasing age (45–54 years: AOR = 5.00, 95% CI: 2.01–12.48; 55–64 years: AOR = 3.77, 95% CI: 1.39–10.23; ≥65 years: AOR = 13.87, 95% CI: 4.62–41.63), diabetes mellitus (AOR = 2.79, 95% CI: 1.49–5.22), and smoking (AOR = 2.25, 95% CI: 1.12–4.50) were strong and significant predictors of CAD. The same risk factors were identified in persons without obesity, but in addition, waist circumference (per 1 cm increment: AOR = 1.04, 95% CI: 1.01–1.07) was a significant predictor of CAD in this group.
Conclusions:
Sex, age, diabetes mellitus, and smoking predicted CAD in all patients. Waist circumference only predicted CAD in persons without obesity, suggesting that normal-weight central obesity might be an important risk factor in this setting.
Background
C
Obesity has increased steadily over the past decades and is now recognized as one of the largest health challenges the world is facing. 4,5 Although high-income countries got the first wave of the obesity pandemic, the second wave has hit low- and middle-income countries with unprecedented strength. Today, several middle-income countries like Mexico, Argentina, Libya, Jordan, Egypt, and South Africa report that more than 25% of the adult population are suffering from obesity, which is a major transition compared to only two decades ago. 6
Obesity is a recognized risk factor for CAD, 7,8 and it is usually defined as a body mass index (BMI) above 30 kg/m2. 9 This definition, however, has obvious limitations as fit individuals with high muscle mass can have the same BMI as unfit individuals with high fat mass. Other measures of obesity have been suggested, including simple indicators such as waist circumference, waist-to-height ratio, and waist-to-hip ratio. 10 Indeed, it has been shown that these indicators add prognostic information, which is not captured by the use of BMI alone. 10,11
Observational studies have found that persons with obesity have a better prognosis in established CAD compared to those with a normal body weight, suggesting that the underlying risk factors might differ between the two groups. 12,13 In this study, therefore, we aimed to explore whether risk factors for CAD differed between individuals with BMI below and above 30 kg/m2. Specifically, we wanted to assess the role of waist circumference in a Middle Eastern setting. Although studies on the association between obesity and CAD have been performed elsewhere, cultural differences in food habits, smoking and physical activity, and ethnic differences in susceptibility to certain risk factors 14 might apply between different parts of the world. Hence, we believe this study can provide new data and inform public health efforts in the region.
Methods
Study setting and participants
Jordan is a middle-income country situated in the Middle East, a region of the world where the prevalence of obesity is among the highest in the world. Indeed, the prevalence of obesity in the adult Jordanian population is estimated at 23.7% in men and 39.6% in women, respectively. 6 Simultaneously, the prevalence of T2DM is higher in the Middle East than in any other region of the world, and steadily increasing from 5.9% in 1980 to 13.7% in 2014. 15
This study was carried out at Prince Hamzah Teaching Hospital, a referral hospital in the capital Amman. Participants were recruited from the catheterization section of the cardiology department between January and December 2015. The department offers elective coronary angiography services to patients with clinical suspicion of CAD (stable angina, ischemic heart disease, chest pain, and positive cardiac stress test). Patients with acute coronary syndrome are treated elsewhere and therefore not included in this study. Individuals who were pregnant or lactating, or who suffered from kidney disease, liver disease, or gastrointestinal disease were excluded. All patients provided written informed consent to participate in the study. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki, and the study was approved by the Institutional Review Board Ethics Committee at Prince Hamzah Hospital.
Data collection
Patients were admitted the day before undergoing coronary angiography. Sociodemographic data, previous health issues (hypertension, diabetes mellitus, and dyslipidemia), smoking status, and family history of cardiovascular disease were recorded by trained research assistants using standardized questionnaires.
Anthropometric measurements
Body weight was measured to the nearest 0.1 kg, with minimal clothing and without shoes, using a calibrated scale (Seca, Hamburg, Germany). Height was measured to the nearest 1 cm with participants in standing position without shoes using a calibrated portable measuring rod. BMI was calculated as the ratio of weight in kilograms to the square of height in meters and was categorized according to the classification system established by the National Institutes of Health: normal body weight, 18.5–24.9; overweight, 25.0 to 29.9; and obese, ≥30.0. 9 Waist circumference was measured by tape at the narrowest level between the lowest rib and the iliac crest at the end of normal expiration in standing position. All anthropometric measurements were carried out by a trained dietitian.
Coronary angiography
The procedure was performed by trained invasive cardiologists using standard technique. In brief, the catheter was inserted into the radial artery using a Seldinger technique, and the tip was advanced to the aortic sinus cusp. X-ray images of the transient radio-contrast distribution within the coronary arteries were carried out to visualize the arterial tree. The degree of obstruction was estimated as percentage of the arterial lumen by comparing the area of narrowing to an adjacent normal artery.
Statistical analysis
The outcome of interest was CAD. Consistent with prior studies, CAD was defined as ≥20% stenosis of one or more coronary arteries. 16,17 This definition was chosen to capture all patients with atherosclerotic coronary heart disease, and not only those with symptomatic disease.
Differences in baseline variables between patients with and without CAD were estimated using chi-square tests for categorical variables and Student's t-tests for continuous variables. Odds ratios (OR) with its corresponding 95% confidence intervals (CI) were estimated using logistic regression models. Univariable logistic regression was computed for the following variables: age, sex, BMI, waist circumference, smoking, diabetes mellitus, hypertension, dyslipidemia, and a family history of cardiovascular disease. Variables with a P-value below 0.2 in univariable analyses were included in the multivariable logistic regression model, using a forward stepwise method. Multi-collinearity was excluded using Spearman's correlation coefficient with a cutoff at 0.7. All tests were two-sided and the significance level was set at P < 0.05. Data were analyzed using SPSS for Windows version 23.0 (SPSS, Inc., Chicago). The results were reported in accordance with the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) statement guidelines. 18
Results
Baseline characteristics
Out of 556 participants who underwent coronary catheterization, 353 (63.5%) had CAD and 203 (36.5%) had a normal coronary angiography. Most participants (n = 395, 70.9%) were male, and median age was 55 years (interquartile range 47–64). Previous hypertension, DM, and dyslipidemia were reported by 263 (47.3%), 215 (38.7%), and 32 (5.8%) study participants, and 287 (51.6%) were current or previous smokers. The mean BMI and waist circumference of the study participants was 29.9 kg/m2 [standard deviation (SD) 6.3] and 106.0 cm (SD 15.5), respectively. Overall, measures of obesity were slightly lower in men compared with women: the mean BMI was 29.1 (SD 6.6) versus 31.9 (SD 5.1) kg/m2 (P < 0.001), and the mean waist circumference was 105.1 (SD 16.0) versus 108.1 (SD 13.7) cm (P = 0.042), respectively.
Two hundred and forty (43.2%) individuals had a BMI of ≥30 kg/m2 and were classified in the obesity group. Hypertension, T2DM, and a family history of cardiovascular diseases were significantly more common in persons with obesity, whereas individuals without obesity were more likely to be men and smokers (Table 1).
Mean (SD).
BMI, body mass index; CVD, cardiovascular disease; SD, standard deviation.
Associations with CAD
In individuals without obesity (BMI <30 kg/m2), sex, age, hypertension, diabetes mellitus and waist circumference were significantly associated with CAD in univariable analysis. In multivariable analysis, adjusted for the other variables in the final model, male sex, increasing age, diabetes mellitus, and waist circumference were strong and independent predictors of CAD, whereas smoking was borderline significant (Table 2).
Bold values are statistically significant, P < 0.05.
Univariable logistic regression analysis.
Multivariable logistic regression analysis, adjusted for the other variables listed.
Mean (SD).
CAD, coronary artery disease; CI, confidence interval; OR, odds ratio.
In persons with obesity (BMI ≥30 kg/m2), sex, age, smoking, diabetes mellitus, and BMI were significantly associated with CAD in univariable analysis. In multivariable analysis, male sex, increasing age, smoking, and diabetes mellitus remained strong and independent risk factors for CAD (Table 3). Waist circumference, however, was not associated with CAD in this group.
Bold values are statistically significant, P < 0.05.
Univariable logistic regression analysis.
Multivariable logistic regression analysis, adjusted for the other variables listed.
Mean (SD).
Waist circumference was an independent predictor of CAD only in persons with BMI below 30 kg/m2 (Fig. 1). The OR of CAD was 1.04 (95% CI: 1.01–1.07, P = 0.013) per 1 cm increment, which corresponds to a 40% increased odds of CAD when the waist circumference increased by 10 cm.
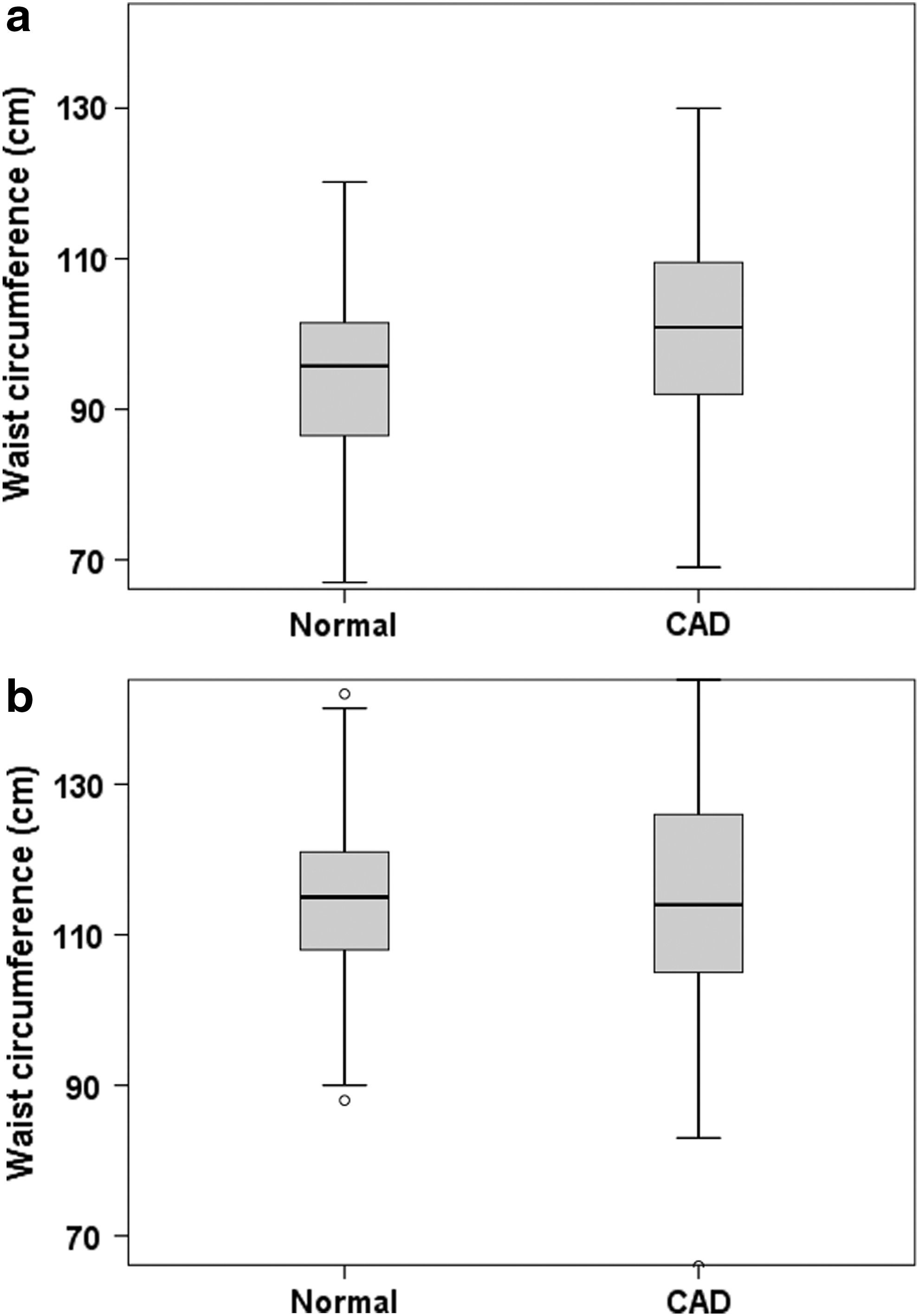
Box plots of waist circumference in patients with and without coronary artery disease in persons with
Discussion
In this study, we found that certain well-established risk factors for CAD, such as male sex, increasing age, diabetes mellitus, and smoking, predicted CAD both in individuals with and without obesity in a Middle Eastern setting. Interestingly, however, waist circumference appeared to be of relevance only in persons without obesity, in whom the risk of CAD increased with 40% for each 10 cm increment in waist circumference.
Central obesity has been recognized as an independent risk factor for CAD in previous studies, 7,19,20 but there is less data on the risk profile of individuals with increased waist circumference yet a normal body weight. Of note, although not reporting central obesity directly, data from the Third National Health and Nutrition Examination Survey (NHANES III) showed that healthy women with a BMI below 25 kg/m2, but high body fat content, had a 2.2-fold increased risk of cardiovascular mortality compared to women with low body fat content. 21 Moreover, in individuals with established CAD, normal-weight central obesity appears to be associated with a poorer outcome. Indeed, in a large study of more than 15,000 patients from three continents, Coutinho et al. found that individuals with a normal BMI yet a high waist circumference had the worst long-term survival rates in individuals with CAD. 22 And in a more recent study, Sharma et al. reported that normal-weight central obesity was associated with a higher mortality risk among elderly patients with CAD. 23
The accumulation of visceral adipose tissue, which promotes the development of insulin resistance, dyslipidemia, and hypertension, is considered a key component in the pathogenesis of T2DM and the metabolic syndrome, which in turn predispose to CAD. 24 Since BMI is unable to distinguish body fat from muscle mass, it is an imperfect indicator of cardiovascular risk. Measurement of waist circumference (or other measures of central obesity), on the other hand, appears to be a more logical approach to assess cardiovascular risk profile. However, in the latest guidelines from the American College of Cardiology, measurement of central obesity is not recommended as part of the baseline evaluation of cardiovascular risk. 25
Current guidelines recommend increased physical activity and dietary interventions to persons with obesity. This has a documented effect on weight loss and visceral fat reduction in subjects without metabolic-related disorders, but the beneficial effect on central obesity in persons with T2DM or dyslipidemia is less certain. 26 Given the growing evidence of the hazards of central obesity on both cardiovascular risk and mortality, future studies should identify effective interventions to model body composition in persons at high risk. This is particularly important in a country like Jordan, where central obesity has been reported in more than half of the adult population. 27
In the current study, individuals without obesity were more likely to be men and smokers. This might explain the higher prevalence of CAD in this group compared to individuals with obesity. Previous studies have found conflicting results regarding the effect of smoking on body weight; however, most larger studies have found an inverse relationship. 28,29 Interestingly, however, smoking appears to be associated with increased waist circumference. 30 Hence, we cannot exclude that the observed effect of waist circumference on CAD in our study could–at least partly–be explained by variations in smoking habits.
This study had some limitations. First, it was a cross-sectional study and thus can only report associations, not causation. 31 However, the risk factors identified are well in line with results from our studies, and we believe our results are valid. Second, being a hospital-based study from a tertiary center, the patients seen in our setting might not be representative of all CAD patients in the country. Ideally, therefore, our findings should be confirmed in larger population-based studies in the Middle East.
In conclusion, we found that traditional risk factors including age, sex, diabetes mellitus, and smoking predicted CAD in Jordan, both in individuals with and without obesity. Waist circumference, however, was only relevant in those with a BMI below 30 kg/m2, indicating that individuals with normal-weight central obesity might be a group of particular risk of CAD. Our study suggests that measures of central obesity should be included in the risk stratification of patients in this setting.
Footnotes
Acknowledgments
We thank the patients who participated in the study, and the hospital management for facilitating the data collection. This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Author Disclosure Statement
No competing financial interests exist.