
Abstract
Background:
Little is known about how the frequency of physical activity in adults influences the occurrence of metabolic syndrome (MetS), and whether there are gender differences within these effects.
Methods:
In this study, 3368 residents from the established “Landseed Cohort” underwent three waves of health examinations, and those who did not have MetS at baseline were selected and analyzed using a multiple Poisson regression model. By calculating the adjusted relative risk (ARR), the linear and nonlinear relationships between the frequency of physical activity and risk of developing MetS were examined for male and female participants.
Results:
The prevalence of MetS was fairly stable across the three waves (ranging from 16.24% to 16.82%), but the incidence dropped from 7.11% to 4.52%. The risk of MetS in women was 10 times higher than that in men (ARR = 10.06; 95% CI = 6.60–15.33), and frequent exercise was shown to help prevent it. The frequency of exercise had a linear dose–response effect in females and an exponential protective effect in males on the occurrence of MetS. Exercising more than four times a week for females and twice or more a week for males effectively reduced the risk of developing MetS.
Conclusions:
The frequency of physical activity in adults was negatively related to the risk of developing MetS, and this relationship differed based on gender. The protective effect of physical activity on MetS was linear in females and exponential in males.
Introduction
M
Physical activity is one of the most important protective factors for MetS. It is generally believed that the more exercises one does, and the longer and more intense the exercise is, the lower the risk an individual has of developing MetS. Conversely, a lack of exercise (such as long sedentary periods) results in a higher chance of developing MetS, 5 reflecting a dose–response relationship. However, recent studies of CVDs have shown that in coronary heart disease (CHD) patients, the relationship between exercise time and CHD death has a reversed J-shape, 6 implying that the impact of exercise on MetS may not be linear. The reversed J-shaped relationship indicates that protecting against MetS requires that the frequency of exercise reach a certain threshold. However, it is neither effective nor harmful if there is insufficient exercise. 7
For middle-aged people, long-term sedentary lifestyles are more common than in the young due to deteriorating physiological function and transformations of work and life patterns. As a result, it is not rare for there to be a lack of exercise, leading to a higher risk of MetS. Some middle-aged people are unable to exercise sufficiently due to the status of their MetS. 8 Others identify that they are gradually losing physiological function with age, and thus pay greater attention to exercise than in the past, hoping to strengthen their body and reduce their risk of developing chronic disease. For the latter group, the strong desire for good health may lead to excessive exercise. Therefore, in cross-sectional studies, this behavior could lead to the mistaken conclusion that exercise is associated with an increased risk of MetS. To avoid the false inferences that may be caused by this type of correlation, it is possible to effectively clarify the causal relationship between the frequency of exercise and MetS using a longitudinal study design. Apart from detecting causal relationships, longitudinal designs also are advantageous as they provide incidence measures; they are effective at determining variable patterns over time and offer high accuracy when observing changes compared with cross-sectional studies. 9
Recently, studies have reported gender differences in the prevalence rates 10 and components 11,12 of MetS. The survey results from the NHANES III (1988–1994) and NHANES 1999–2006 12,13 studies demonstrate that, regardless of age range, increases in the prevalence of MetS in women are higher than that in men. Interestingly, gender differences were also found in leisure-time physical activities. Women were less active than men 14 and tended to engage in less intense activities. 15 These results suggest that gender-specific factors should be taken into consideration when discussing the mechanisms of MetS development and strategies for its treatment and prevention, 10 including those that are unfavorable or less protective for women. However, there is a lack of relevant information in the literature.
The clarification of different types of exposure-disease relationships has a significant impact on public health prevention and intervention strategies. For this reason, large-scaled, longitudinal studies can provide a larger volume of useful information than small-sample cross-sectional studies. In addition, understanding the specific gender-related factors and mechanisms can provide more effective health solutions for each gender. Following from this, the present study used the large-scale community cohort that was established by Taiwan Landseed Hospital to conduct a secondary data analysis. The study aimed to demonstrate the possible mechanisms and causality between the frequency of physical activity and MetS in middle-aged males and females.
Methods
Participants
The “Landseed Cohort” is a large-scale, long-term follow-up study. Through the “Community-to-Point Combined Screening Service,” a platform for preventive medicine services is provided in the Taoyuan Pingzhen District of Taiwan, and a community health database has been established. Since 2006, 15,000 individuals were randomly selected from 18 (population: 80,700) out of the 46 districts (population: 194,189) and were invited to be subjects. Each year, the selected individuals were invited to undergo the screening service. The inclusion criteria for this study were as follows: (1) participants should be residents who have been living in Taoyuan Pingzhen district since December 31, 2005; (2) participants should be aged 30 years or older; (3) participants must have completed the three waves of screening and have complete files. Data from 2007 to 2011 were used for the analyses.
Of the 15,000 individuals, a total of 5757 people were enrolled in the follow-up, and of these, 3644 in total completed the three waves of screening. As this study used incidence cases to explore the relationship between the frequency of physical activity and MetS, people who developed MetS (n = 276) during the first wave of screening were excluded. This left a total of 3368 participants who were included in the analysis (Fig. 1). This study was approved by the Institutional Review Board of Landseed Hospital. All participants gave their signed informed consent.
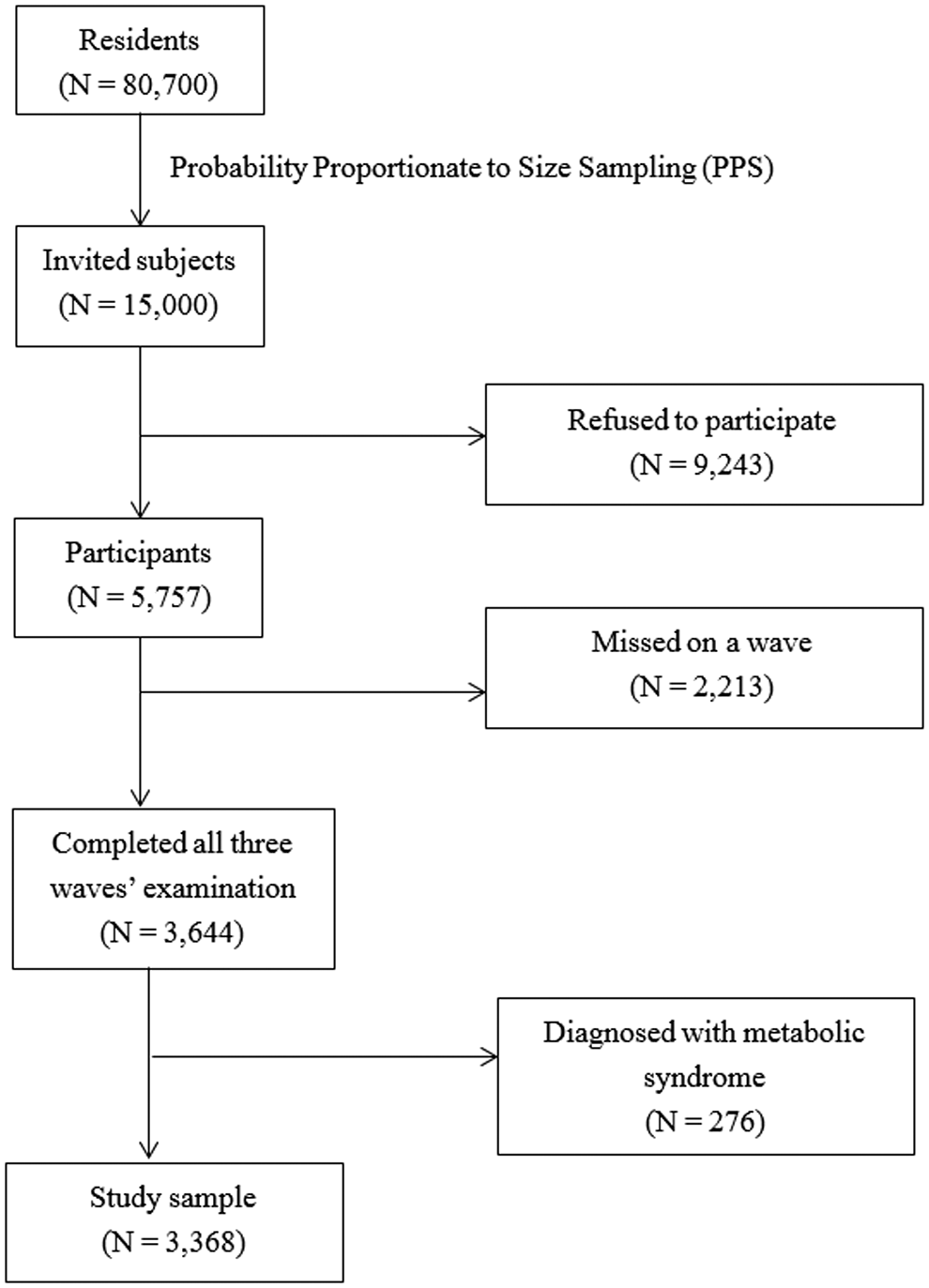
Flowchart of selecting study sample.
Measures
Metabolic syndrome
The incidence of MetS in this study was assessed according to the National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III). Considering differences between ethnic groups, Taiwan's National Health Agency recommended the use of a waist circumference greater than 90 cm in males and greater than 80 cm in females as the standard to define abdominal obesity. This study ascribes to this recommendation. The first wave of screening ruled out people who had already developed MetS from follow-up. People who met the criteria during the second or third wave were classified as MetS cases. People who were not diagnosed after the three waves of screening were defined as the healthy group.
Frequency of physical activity
The frequency of physical activity was assessed based on the number of times per week that the participant engaged in exercise. For example, if one participant regularly exercised twice a day, he or she would be asked to self-report 14 activities per week in the screening questionnaire. This study treated the number of exercise activities as a continuous variable. Nevertheless, the frequency of physical activity was divided into tertiles to preliminarily understand its distribution. As the Taiwan Sports Administration has long used “7 days/week exercising three times for 30 min, with the exercise heart rate reaching 130 beats/min” (a.k.a. the 7333 criteria) as the definition of regular exercise, the present study followed this criteria and stratified those who exercised 0–3 and 4–7 times/week into two different groups. In addition, individuals who exercised 8 or more times a week were somewhat special and thus were assigned to a third group.
Control variables
To avoid interference from confounding factors, this study took nine potential confounding factors into consideration in the analysis: lifestyle, eating habits, family disease history, personal disease history, drug use, health food consumption habits, marital status, Health Rating Scale (Depression Rating Scale), Quality of Life Questionnaire (SF-36), and basic demographic data. Data for the control variables were derived from the results of self-administered questionnaires.
Data analysis
In this study, the influence of the frequency of physical activity on MetS was analyzed using the GENMOD statistical program in SAS. After controlling for the confounding variables, the adjusted relative risks (ARRs) and 95% CIs of the influence of physical activity on MetS were calculated with a multiple Poisson regression model. The first and second quadratic variables of the frequency of physical activity were introduced into the model to test for linear and nonlinear relationships. The regression equation is as follows:
where Met is metabolic syndrome, PA is the frequency of physical activity, and Cf represents the confounding factors.
In addition, using the results obtained from the above model, Sigma Plot 12 was used to plot and show the relationship between the frequency of physical activity and MetS risk.
Results
Of the 3368 individuals included in the study, there were slightly more women (n = 1898, 56.35%) than men (n = 1470, 42.25%). Men were significantly older, had more years of education, higher personal yearly income, were more likely to be smokers, drinkers, and betel nut chewers, had heavier workloads, and engaged in less exercise than women (Table 1). Compared with the total sample included in this study, those who were excluded from wave 1 to wave 2 (n = 1118) did not significantly differ on the distribution of the study variables except for their younger age (Appendix Table A1). Similarly, the characteristics of those excluded from wave 2 to wave 3 (n = 995) did not differ from the total sample included in this study except for their younger age, higher proportion of current smoking, and lower proportion of moderate physical load work. The paucity of variables that were distributed differently between the final and excluded samples implies, to some extent, that the study had internal validity.
Low education: ≤9 education year; high education: ≥9 education year.
“other” including not married, separated, divorced, or widowed.
P < 0.01.
P < 0.001 (astericks showing on female column represent variables were significantly different between sex).
Across the three waves of screening, the point prevalence of MetS was fairly stable; between 16.24% and 16.82% (Fig. 2), while the cumulative prevalence rate across the three waves of screening was 25.95%. In contrast, the incidence rate fluctuated substantially. The incidence increased 7.11% from the first wave to the second wave; however, comparing the second wave to the third wave, the incidence dropped to 4.52%, and the cumulative incidence rate of the three waves of screening was 11.59%.
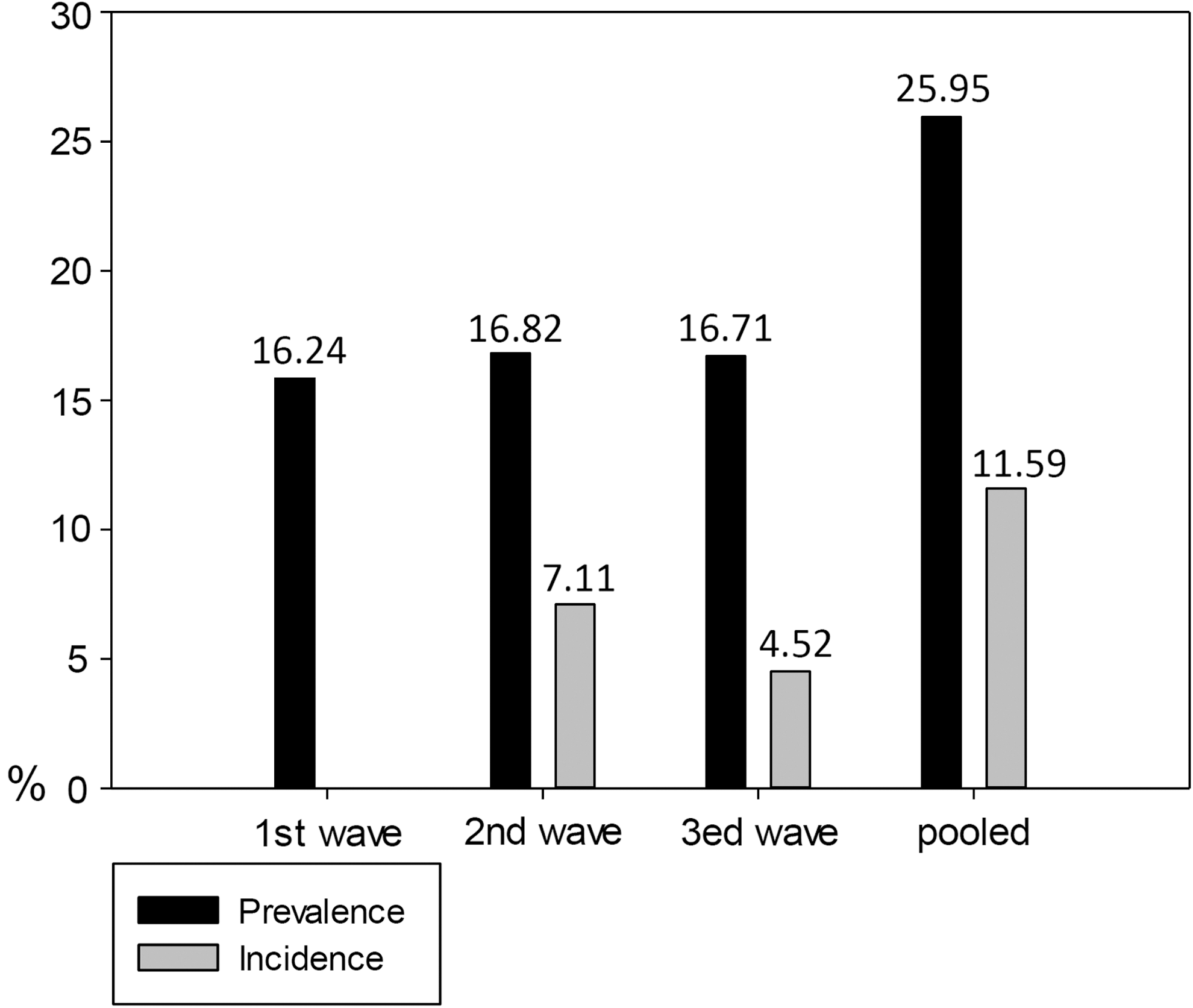
Prevalence and incidence of metabolic syndrome across three waves.
Data from the three waves of screening were evaluated with a multiple regression model, introducing the nine potential confounding factors into the model. This study found that the risk of developing MetS was 10 times higher in women than men (ARR = 10.06; 95% CI = 6.60–15.33%; Table 2). In light of this, we further examined the data from males and females separately in the table, with the aim of clarifying the gender differences. Across the sample, the risk of MetS was 1.65 times higher in those older than 50 years than in those younger than 50 years (ARR = 1.65; 95% CI = 1.01–2.74). The risk of developing MetS was higher in active smokers than nonsmokers (ARR = 1.81; 95% CI = 1.04–3.12). The frequency of physical activity had both linear (ARR = 0.99; 95% CI = 0.98–0.99) and exponential (ARR = 0.93; 95% CI = 0.86–0.99) protective effects. The results for females were similar to the results for the whole sample, but active drinkers had a significantly higher risk of MetS (ARR = 1.89; 95% CI = 1.04–3.46). Interestingly, none of the study variables showed a significant relationship with the incidence of male MetS, and the impact of the frequency of physical activity on MetS was, although not significant, different from that found for women.
P < 0.05.
ARR, adjusted relative risk.
To understand the differential effect physical activity has on MetS between genders, we analyzed the risk of MetS under various frequencies of physical activity in males and females, respectively. As shown in Figure 3 the frequency of physical activity had a linear protective effect on the occurrence of MetS in females, and exercising more than four times a week effectively reduced the risk of MetS (ARR <1.0). However, the impact of the frequency of physical activity on MetS displayed an exponential trend in males, and exercising twice or more per week effectively reduced the risk of MetS (ARR <1.0).

Adjusted relative risk of weekly frequency of physical activity on the occurrence of metabolic syndrome, by gender.
Discussion
The participants included in this study were community residents who were slightly older than general population, with a good lifestyle, but low socioeconomic status. After three waves of screening, the study found that MetS had a stable point prevalence rate, but the incidence rate decreased significantly. Female gender, older age, and current smoking were risk factors for MetS, and physical activity was a protective factor against it. In addition, the study also found that the relationship between the frequency of physical activity and MetS was linear in females, but had a nonlinear exponential trend in males.
The prevalence of MetS in the sampled community in Taiwan was 16%–17%, which is similar to the rate found by previous large-scale national studies in Taiwan (ranging from 13.4% to 16.4% according to different criteria), 16 but is lower than the US estimate. For example, the National Health and Nutrition Examination Survey (NHANES) noted that the prevalence rate of MetS among adults aged 20 years and older in the United States over the past two decades was 22.9%–36.1%. 17,18 This difference may be attributed to differences in the degree of industrialization between the two countries. In general, compared to eastern countries, the diet and lifestyle in western countries may make people more susceptible to MetS. 19 In addition, race and genetics may also be factors that contribute to differences in the prevalence of MetS between Taiwan and other countries. For example, a survey sampling multiple ethnicities in Malaysia indicated that those of Chinese ethnicity had the lowest susceptibility to MetS. 20
Decreases in the incidence of MetS in this study may be due to an increase in the awareness of the disease among some of the participants. This may have resulted in lifestyle changes or the decision to undertake treatment for symptoms, further reducing the incidence rate in the second and third wave of screening. The decreased incidence may also be due to the fast progression of MetS during initial stages of the syndrome, which gradually slowed in later stages. 21 The argument may be made that the changes to the incidence rates in the final sample may be attributed to the excluded subjects, who may be more likely to have MetS. However, this may not be the case because the majority of the variables were distributed consistently between the final and excluded samples, implying that the final sample was representative of the main cohort.
Another major finding of this study was that the higher the frequency of physical activity per week an individual had, the lower their chances were of developing MetS. This further suggests that physical activity has a protective effect on MetS. It is noteworthy, however, that this protective effect had a different mechanism in males and females. The risk to females of developing MetS decreased linearly with increases in the frequency of physical activity per week, consistent with results from previous studies on menopausal women aged between 45 and 75 years old. 22,23 Yet, for men, the frequency of physical activity and the risk of developing MetS showed a reversed J-shaped relationship. In males who exercised less than four times a week, with each additional incremental increase in the frequency of physical activity, the risk of MetS decreased significantly. However, for males who exercised more than four times a week, each additional increase in the frequency of exercise contributed to a smaller reduction in the risk of developing MetS. In addition, women needed to exercise more than four times a week to be able to reduce MetS, compared with exercising only twice a week in men.
The protective effect of physical activity against developing MetS is obvious, and this protective effect increases significantly with increases in the frequency of physical activity. This suggests that exercise is very effective in reducing the incidence of developing MetS in men. Previous studies have found that out of all age groups and genders, older men with obesity have the highest cardiovascular mortality risk. 24 This indicates that the risk of cardiovascular and metabolic disease could be significantly reduced in middle-aged men if they can reduce their weight through exercise. In contrast, women need higher-frequencies of exercise to accumulate physiological advantages and effectively reduce the incidence of MetS. This partly explains why the risk of MetS in this study was 10 times higher in females than in males. Moreover, because the age with the highest prevalence of MetS occurs earlier in men than in women, 25 the use of hormone replacement therapy among postmenopausal females may reduce the effects of physical activity on changing the HDL concentration. 26 Thus, the higher risk of MetS in women in this study may be due to having older female participants.
Previous research has shown advantages for males in the relationship between physical activity and MetS, and this may be attributed to differences in preferences for exercise between males and females. 15 Compared with females, males are more likely to engage in outdoor and higher intensity exercise, which results in higher vitamin D concentrations and reduced systolic pressure levels. As moderate-intensity exercise 27 reduced systolic pressure 28 and high vitamin D concentrations 29 are associated with a lower risk of MetS, exercise preferences may partly explain why male physical activity is more effective in improving MetS. There is still very little literature explaining gender differences in the impact of the frequency of physical activity on developing MetS, and the present findings require further validation by other studies in the future.
There are several limitations in this study. The first is that the study sample was from a slightly older population. As there were no data available to compare between nonparticipating citizens and participants, the low response rate in this study may have resulted in a potential selection bias that could hamper the generalizability of the findings from this study to the target population. As such, although the results may be used as a reference for middle-aged people, they cannot be used to draw conclusions about either the general population or the MetS population. It should also be cautious to interpret our incidence data for there could be an immortal time bias associated to those who persisted to wave 2 and 3, which may affect external validity of estimated incidence rate. The second limitation is that different physical activity patterns did not appear to have the same protective effect on MetS. 30 Measurement of physical activity in this study was limited to evaluating frequency; the intensity and duration of physical activity were not available for assessment. In the future, studies could include and distinguish the effects of a larger variety of physical activities and discuss their impact on MetS in males and females.
In conclusion, the frequency of physical activity in middle-aged adults was negatively related to the risk of developing MetS, and this relationship differed based on gender. The protective effect of physical activity on MetS was linear in females and exponential in males.
Footnotes
Acknowledgments
The authors are indebted to all of the participants for their dedicated contributions.
This work was supported, in part, by the collaborative projects between Chung Shan Medical University and Landseed Hospital (CSMU-LSH-101-02 and CSMU-LSH-102-01) awarded to Dr. Hao-Jan Yang.
Author Disclosure Statement
No competing financial interests exist.
| Total sample (N = 3368) | Missing at wave 2 (N = 1118) | Missing at wave 3 (N = 995) | |
|---|---|---|---|
| Variables | n (%) | n (%) | n (%) |
| Age (mean, SD) | 60.88 (12.30) | 58.18 (15.07) ** | 55.55 (14.28) ** |
| Height (mean, SD) | 159.44 (8.09) | 159.21 (8.44) | 158.93 (8.63) |
| Weight (mean, SD) | 61.19 (5.96) | 61.88 (4.03) | 62.62 (3.69) |
| BMI (mean, SD) | 24.01 (15.78) | 24.61 (12.14) | 24.72 (11.50) |
| Education level a | |||
| Low | 1530 (45.43) | 517 (46.28) | 444 (44.63) |
| High | 1838 (54.57) | 601 (53.72) | 551 (55.37) |
| Marital status b | |||
| Married | 3048 (90.49) | 1020 (91.25) | 880 (88.44) |
| Other | 320 (9.51) | 98 (8.75) | 115 (11.56) |
| Personal income (NT dollar) | |||
| <500k | 2719 (80.73) | 893 (79.84) | 814 (81.76) |
| 500k–1 m | 555 (16.49) | 188 (16.86) | 150 (15.04) |
| 1–1.8 m | 72 (2.14) | 31 (2.80) | 23 (2.40) |
| >1.8 m | 22 (0.64) | 6 (0.50) | 8 (0.80) |
| Current smoking | |||
| No | 2889 (85.78) | 944 (84.44) | 807 (81.07) ** |
| Yes | 479 (14.22) | 174 (15.56) | 188 (18.93) |
| Current drinking | |||
| No | 3025 (89.83) | 981 (87.78) | 875 (87.92) |
| Yes | 343 (10.17) | 137 (12.22) | 120 (12.08) |
| Current betel nut chewing | |||
| No | 3301 (98.03) | 1090 (97.48) | 965 (97.01) |
| Yes | 67 (1.97) | 28 (2.52) | 30 (2.99) |
| Physical load of work | |||
| Mild | 2789 (82.82) | 914 (81.80) | 828 (83.23) * |
| Moderate | 433 (12.86) | 152 (13.58) | 106 (10.62) |
| Heavy | 146 (4.33) | 52 (4.62) | 61 (6.16) |
| Frequency of activity/week | |||
| 0–3 | 1626 (48.28) | 510 (45.61) | 480 (48.25) |
| 4–7 | 1700 (50.49) | 595 (53.22) | 502 (50.45) |
| ≥8 | 42 (1.24) | 13 (1.17) | 13 (1.30) |
Low education: ≤9 education year; high education: ≥9 education year.
“other” including not married, separated, divorced, or widowed.
P < 0.05.
P < 0.001 (astericks showing on missing wave columns represent subjects missing at that wave were significantly different from total sample on those variables.)