
Abstract
Background:
Metabolic syndrome (MetS) is closely linked with type 2 diabetes mellitus (T2DM) and cardiovascular diseases. The T2DM is one of the major causes of mortality and public health concern in Mexico. Some studies reported MetS prevalence in different regions from Mexico. However, a systematic report or meta-analysis on MetS prevalence is not available. The aim of this study was to estimate the pooled prevalence of MetS among apparently healthy Mexican adults.
Methods:
A systematic review was done of scientific articles published and available from different sources, including MEDLINE/PubMed, Web of Science, Cochrane Library, LILACS, and SCIELO. The overall prevalence of MetS and prevalence based on different diagnostic criteria [National Cholesterol Education Program-Adult Treatment Panel III (NCEP-ATP III), International Diabetes Federation (IDF), American Heart Association/National Heart, Lung, and Blood Institute (AHA/NHLBI), and World Health Organization (WHO)] were pooled using a random-effects model, and the results were presented in a forest plot. The study was performed based on the criteria of Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA).
Results:
Altogether, 15 studies were included in the systematic meta-analysis. The estimated prevalence of MetS, based on different criteria, was as follows: IDF 54% (95% CI 0.44–0.63), AHA/NHLBI 48% (95% CI 0.34–0.62), ATP III 36% (95% CI 0.30–0.42), and WHO 31% (95% CI 0.04–0.81). According to the Der Simonian–Laird random-effects model, a pooled prevalence of MetS in Mexico was 41% (95% CI 0.34–0.47).
Conclusions:
This study reported a high prevalence of MetS among healthy Mexican adults, in comparison with reports from other countries, including United States and Latin America. An urgent need to control and prevent MetS and its consequent health complications in Mexican populations is recommended.
Introduction
M
AHA/NHLBI, American Heart Association/National Heart, Lung, and Blood Institute; AO, abdominal obesity based on WC; ATP III, Adult Treatment Panel III; BMI, body mass index; HDL-C, high-density lipoprotein-cholesterol; IDF, International Diabetes Federation; IR, insulin resistance; M, men; MetS, metabolic syndrome; T2DM, type 2 diabetes mellitus; W, women; WC, waist circumference; WHO, World Health Organization.
Diverse diseases have been linked to MetS, but cardiovascular diseases (CVDs) and type 2 diabetes mellitus (T2DM) have been more widely studied and reported to be associated with MetS. 4 Some authors also related MetS to chronic renal diseases, nonalcoholic fatty liver disease, polycystic ovary syndrome, and cancer, among other noncommunicable diseases. 5 –8
The insulin resistance and abnormal regulation of lipid metabolism are some of the several mechanisms involved in the pathogenesis of MetS. 9 Moreover, MetS is a multifactorial disorder, and therefore age, body weight, socioeconomic status, and other lifestyle factors are involved directly or indirectly in the pathogenesis of the syndrome. 10 Globally, the estimated prevalence of MetS in the adult population that have been reported was ∼20%–25%. 11,12 The growing prevalence of T2DM, hypertension, CVD, and obesity has been paralleled to the increasing prevalence of MetS. 13 Especially, the MetS prevalence is growing rapidly among children and young adults worldwide. 1 Despite the differences in the standard criteria (ATP III, IDF, AHA/NHLBI, and WHO) to diagnose MetS, it is well accepted that the prevalence of MetS is increasing in low-, middle-, and high-income countries. 14
In this study, we intend to access maximum possible reports on the prevalence of MetS in Mexican healthy adult populations. Therefore, estimation of MetS prevalence and identification of the associated factors will enable us to recommend policies for the prioritization and implementation of interventions through Mexican national and regional health and welfare programs to combat and prevent MetS. The present systematic review and meta-analysis summarize the recent prevalence and trends of MetS among healthy adults aged 18 years and above from Mexico.
Methods
Study design and search strategy of data sources
A systematic review and meta-analysis were performed using published articles on the prevalence of MetS in Mexican adults. The studies were identified through Internet search using the sources of MEDLINE/PubMed, Web of Science, Cochrane Library, LILACS, and SCIELO. The search terms were taken from the Medical Subject Headings library of PubMed. The following keywords were used in combination: “metabolic syndrome X” (that includes other terms: Insulin Resistance Syndrome X, Syndrome X, Insulin Resistance, Reaven's Syndrome X, and Metabolic Cardiovascular Syndrome), “prevalence,” and “Mexico.” The search was also performed using the Spanish equivalents of these terms. The search was done for titles and/or abstracts. The search strategy for MEDLINE was developed first, and then adapted for the remaining sources. The gray literature was searched using Google Scholar. The searching of articles was carried out between March and July 2017.
Selection of studies
Studies were selected for the systematic review and meta-analysis if they were conducted in Mexico and reported the prevalence of MetS. A total of 192 relevant studies were identified and exported to EndNote X5 (Philadelphia); duplicates were eliminated. Then, the following inclusion criteria were applied: (1) cross-sectional studies; (2) studies that were conducted among 18 years of age or older and reportedly healthy individuals; and (3) to define MetS, studies that used any defined criteria to determine the prevalence of MetS.
The exclusion criteria for our study were as follows: (1) the reviews and letters to the editors, (2) studies that used animal models, (3) studies performed outside of Mexico, (4) the study population comprising individuals who were reported to have other health complications, (5) studies focusing on biological pathways, (6) studies with incomplete information, and (7) no abstract (Fig. 1).
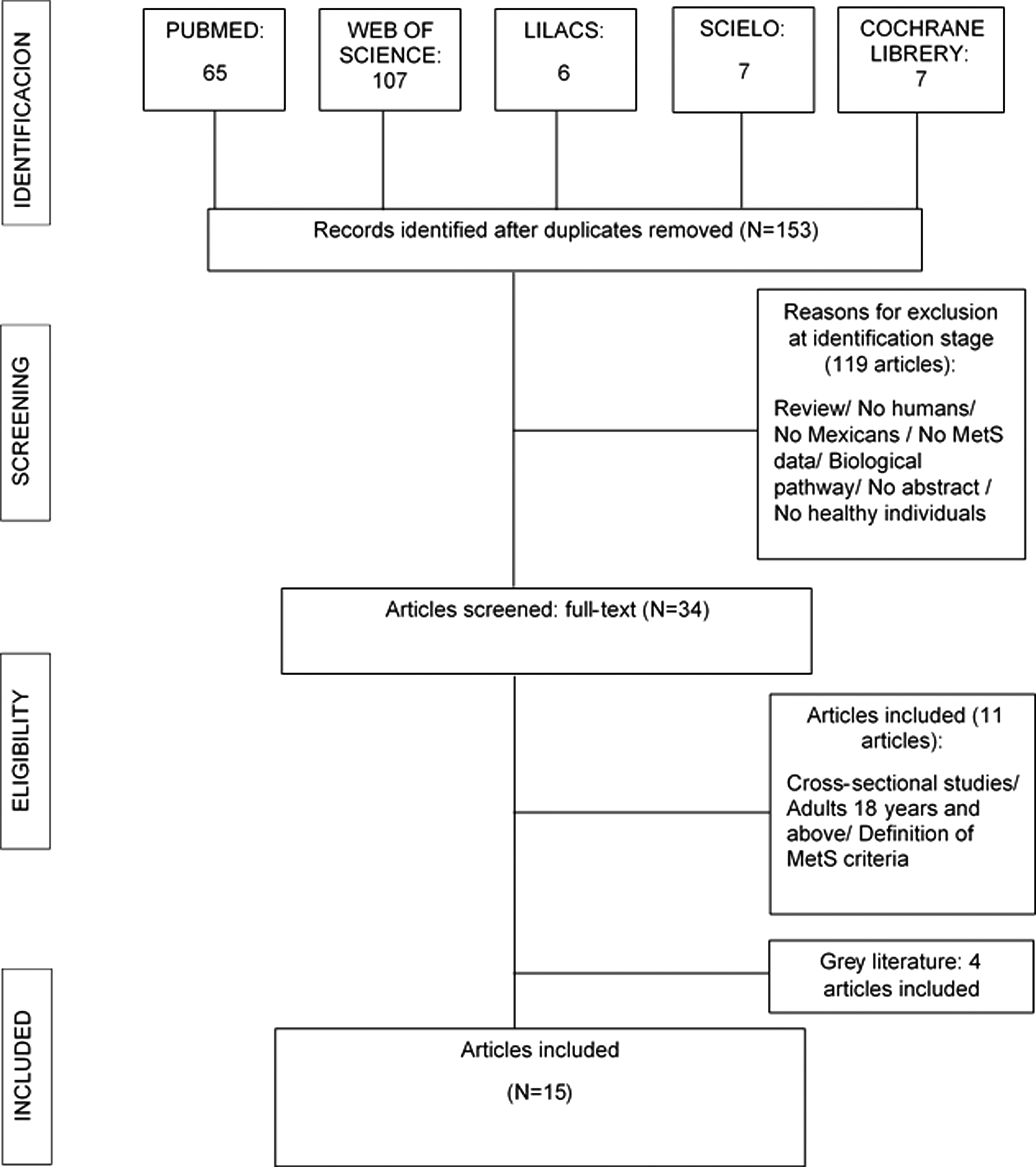
Flow diagram of studies included in the systematic review.
After preliminary screening of the titles of the studies, all abstracts were evaluated for eligibility, based on the established criteria. At this point, some studies were assessed in full length. There was no restriction in the year of publication, recruitment period, or sample size.
Data extraction
This study has been performed based on the criteria of Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 15 (Fig. 1). Data from the selected studies were extracted into a predefined form, such as first author information, year of publication, study type and location, sample size, age, and prevalence of MetS (Table 2).
BP, blood pressure; CARMELA, Cardiovascular Risk Factor Multiple Evaluation in Latin America; G, glucose; HT, hypertension; HTG, hypertriglyceridemia; N/A, not available; TAG, triglyceride.
Statistical analysis
All statistical analyses were undertaken using the software RStudio version 1.0.153. The prevalence of MetS reported in the selected cross-sectional studies among healthy Mexican adult populations was analyzed based on different diagnostic criteria used. Then, prevalence of MetS was pooled using a random-effects model and afterward presented in a forest plot. Statistical heterogeneity was assessed using the I 2 index. The statistical program was also used to determine the responsible factors for the observed heterogeneity through meta-regression.
Results
Identified studies
In total, 192 articles were identified. Altogether, 39 articles were eliminated due to duplications in the search. After applying exclusion criteria, 119 articles were eliminated. Altogether, 34 articles were reviewed in full text, and only 11 articles matched with the inclusion criteria; 4 articles were found in the gray literature and fulfilled the inclusion criteria. Finally, 15 studies were selected for the present review and meta-analysis (Fig. 1).
Description of studies
Year of publication of the studies ranged from 2004 to 2016. Thirteen of 15 studies were carried out in urban areas of Mexico. Only two studies 16,17 estimated the prevalence of MetS from Mexican rural communities showing a high prevalence of 41.1% and 45.2%, respectively. The rest of the studies were carried out in different cities of Mexico: Mexico City, Guanajuato, Guadalajara, Merida, Puebla, Baja California Norte, Morelos, and Queretaro.
Population backgrounds and the recruitment period of the participants were different in the selected studies (Table 2). Among the reports, del Pilar Cruz-Dominguez et al. (January–April 2014) 18 and Denova-Gutiérrez et al. (March–April 2006) 19 estimated MetS prevalence in samples drawn from nurses, physicians, and academic staff. The study carried out by Díaz-Cisneros et al. (February 2000) 20 estimated MetS prevalence from teachers. Goodman et al. (October 2008) 16 and Echavarría-Pinto et al. (2004) 17 conducted studies in rural communities. Escobedo et al. (September 2003–August 2005) 21 and Rojas et al. (October 2005–May 2006) 22 reported data from big cross-sectional surveys, including Cardiovascular Risk Factor Multiple Evaluation in Latin America (CARMELA) and Mexican National Survey of Health and Nutrition (ENSANUT in Spanish acronym), respectively. The authors, Jiménez et al. (June 2007–April 2008), 23 Castro-Sansores et al. (September 2008–December 2009), 24 and Gonzalez-Mejia et al. (March 2012–February 2014), 25 carried out studies among hospitalized patients who had undergone treatments for different diseases not including CVD. Authors such as García-Jiménez et al. (October 2007–April 2008), 26 Aguilar-Salinas et al. (February 2000), 27 González-Chávez et al. (2008), 28 Isordia-Salas et al. (May 2011), 29 and Gurrola-Díaz et al. (no data) 30 estimated MetS prevalence from other Mexican communities (Table 2).
Prevalence of MetS was reported based on different criteria and was also compared: Gonzalez-Mejia et al. 25 stated a MetS prevalence using ATP III, WHO, and IDF criteria, and Rojas et al. 22 used ATP III, IDF, and AHA/NHLBI criteria. In addition, Isordia-Salas et al. 29 evaluated the prevalence of MetS according to IDF and AHA/NHLBI, and Aguilar-Salinas et al. 27 reported prevalence based on ATP III and WHO criteria. In another study, González-Chávez et al. 28 described MetS prevalence using ATP III, IDF, and WHO criteria (Table 2).
The overall prevalence of MetS was estimated from pooled information of 15 selected studies. However, four subgroups were allocated based on different criteria: ATP III subgroup was integrated by 12 studies, and WHO subgroup consisted of 3 studies. Moreover, five studies were allocated to IDF subgroup, and finally three studies were classified in AHA/NHLBI subgroup (Table 2). It was interesting to observe that in eight studies, proportion of women was higher than men, and in six reports the proportions of women and men were not described. Six studies reported prevalence of MetS by sex.
Factors associated with MetS
The inter-relationships between different risk factors and the presence of MetS were analyzed in 6 of 15 studies. The risk of MetS increased significantly with the consumption of sweetened beverages 19 and alcohol. 16 It was found that high concentrations of C-peptide, 25 TNF-α, 30 leptin, 26 and uric acid 23 were positively associated with MetS. Individuals who consumed more than two servings of sweetened beverages per day showed a greater risk of having MetS (two times). 19 Goodman et al. 16 revealed that drinking alcohol at least once a week had a positive correlation with the MetS (P = 0.003). In addition, Castro-Sansores et al. 24 reported association of MetS with degrees of hepatic fat infiltration, and del Pilar Cruz-Dominguez et al. 18 showed an association between excess weight (overweight and obesity) and MetS.
Components of MetS in Mexico
The prevalence of the components of MetS was reported in 12 studies; among these Escobedo et al., 21 Jiménez et al., 23 and Isordia-Salas et al. 29 reported the prevalence of the components separately for men and women. The prevalence of AO was reported in 10 studies. The AO showed to be more prevalent among urban individuals in the Mexico City, based on IDF criteria (100%). 29 Differences in the prevalence of AO in adults varied ∼36%. The prevalence of increased glucose levels was reported in 10 studies; based on IDF criteria, Isordia-Salas et al. 29 showed the highest prevalence of increased glucose levels (67.3%) among men. However, levels of increased glucose levels varied from 7% 20 to 45.8%. 16 The prevalence of hypertension was reported in 11 studies; AHA/NHLBI criteria presented the highest prevalence of hypertension with 50.2% for women and 65.2% for men. 29 However, del Pilar Cruz-Dominguez et al. 18 using the ATP III criteria showed the lowest prevalence of hypertension (2.2%) among healthy individuals from Mexico City. Prevalence of increased levels of triglycerides was reported in 10 studies; using the ATP III criteria, Escobedo et al. 21 showed the highest prevalence of 85.7% in women and 93% in men. Ten studies reported prevalence of low HDL-C (Table 2).
Meta-analysis
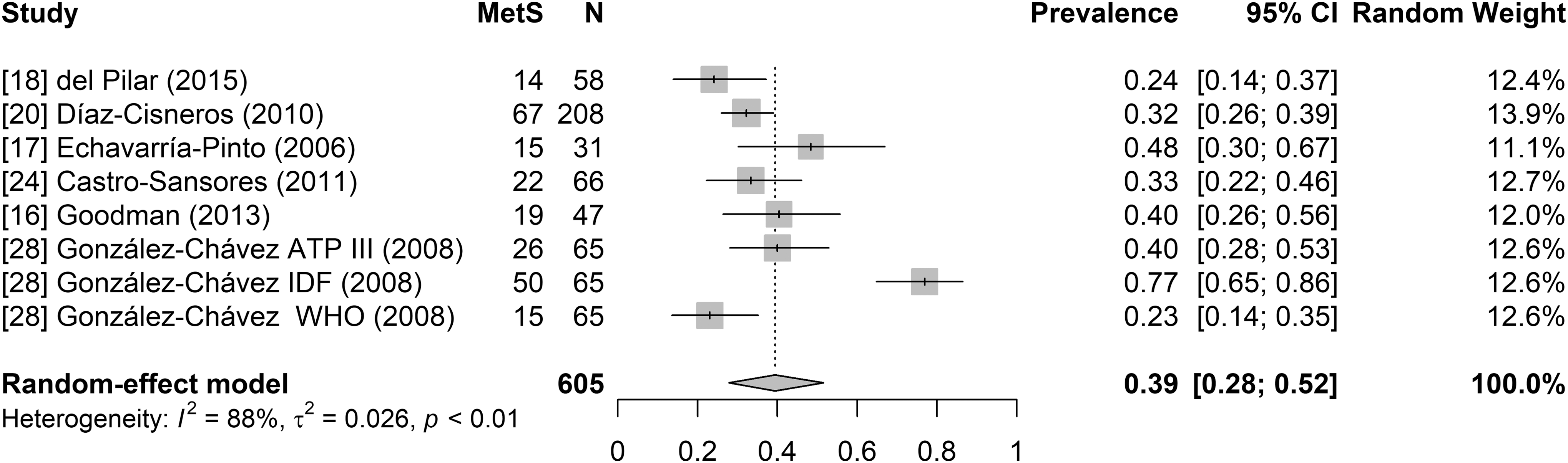
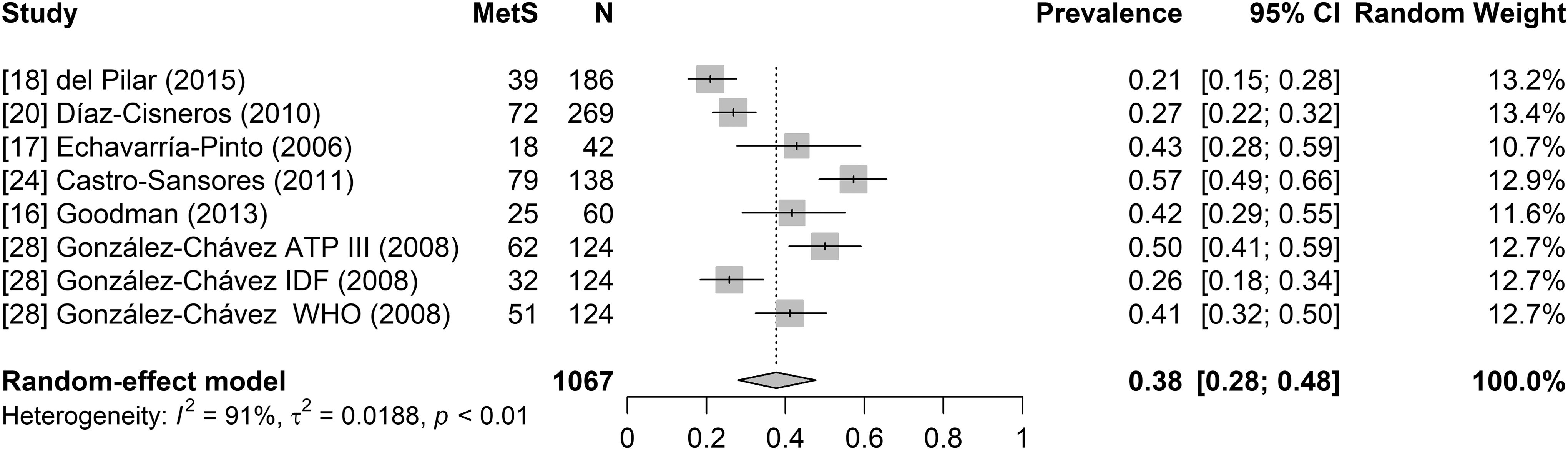
Twelve studies presented a prevalence of MetS using the ATP III criteria, five studies defined MetS according to IDF, three studies used WHO criteria, and three studies defined MetS according to AHA/NHLBI. The observed prevalence of MetS varied between 31% and 54% based on different criteria. The estimated prevalence of MetS for ATP III subgroup was 36% (95% CI 0.30–0.42) (Fig. 2), and for IDF subgroup it was 54% (95% CI 0.44–0.63) (Fig. 3); for WHO subgroup, it was 31% (95% CI 0.04–0.69) (Fig. 4), and for AHA/NHLBI subgroup it was 48% (95% CI 0.34–0.62) (Fig. 5). According to the Der Simonian–Laird random-effects model, the pooled prevalence of MetS in healthy adult Mexican populations was 41% (95% CI 0.34–0.47) (Fig. 6). The results showed that studies using IDF criteria presented the highest prevalence and WHO criteria reported the lowest prevalence. Differences in the prevalence of MetS among adults varied ∼23%. Furthermore, six studies reported prevalence of MetS by sex; men showed a prevalence of 39% (95% CI 0.28–0.52) and women 38% (95% CI 0.28–0.48) (Figs. 7 and 8).

Forest plot of the studies of population using ATP III. ATP III, Adult Treatment Panel III.
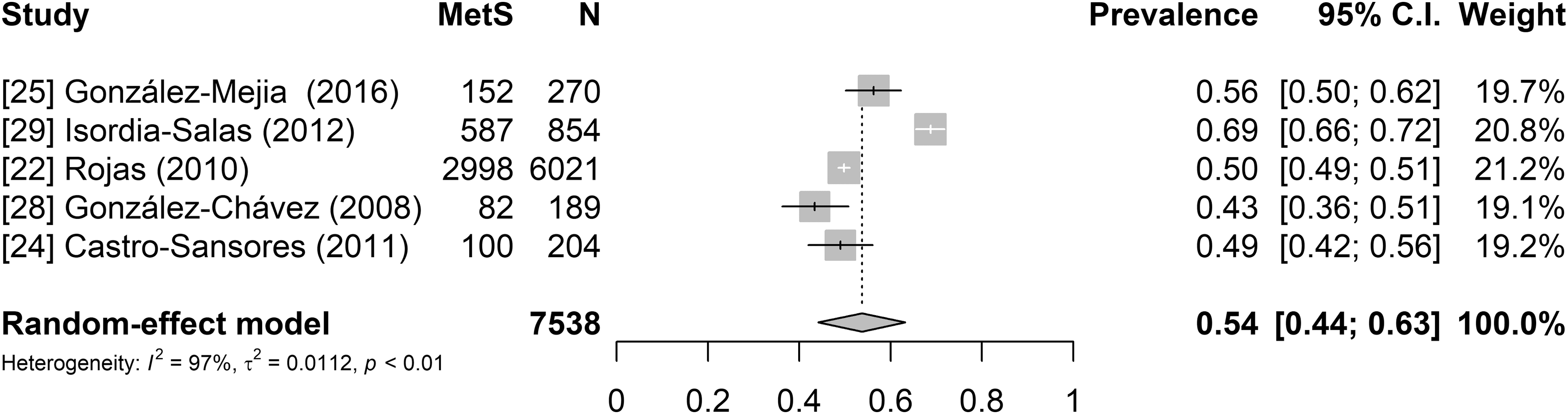
Forest plot of the studies of population using IDF. IDF, International Diabetes Federation.
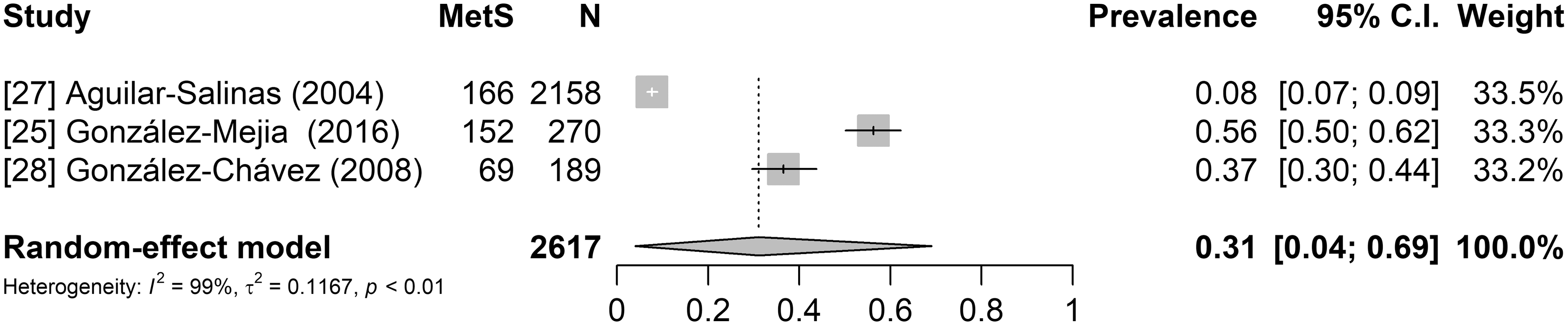
Forest plot of the studies of population using WHO. WHO, World Health Organization.
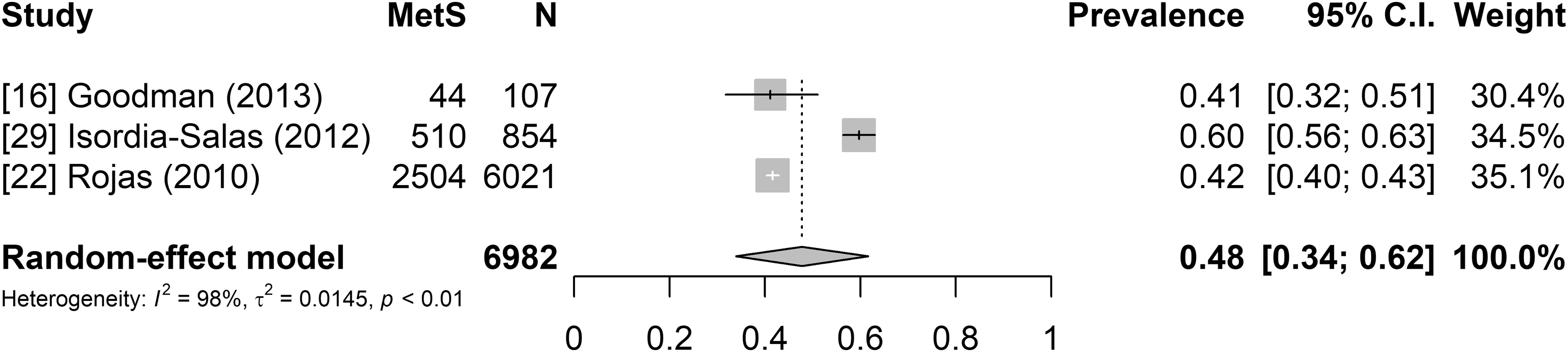
Forest plot of the studies of population using AHA/NHLBI. AHA/NHLBI, American Heart Association/National Heart, Lung, and Blood Institute.
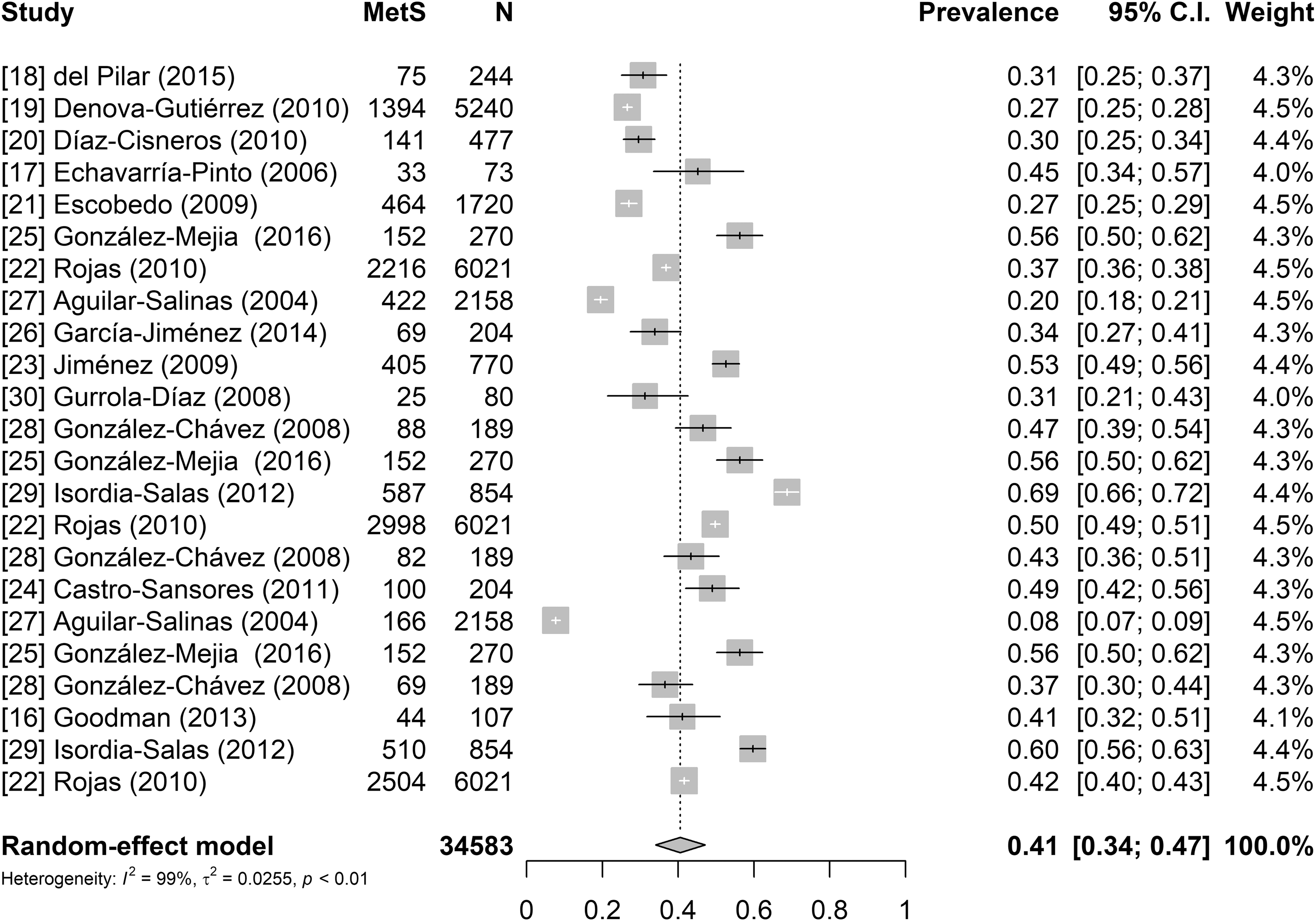
Forest plot of the pooled prevalence of the studies among healthy Mexicans.
Forest plot of the studies of men population.
Forest plot of the studies of women population.
A meta-regression analysis was performed to take the different criteria into account. In the univariate meta-regression analysis, only the variables of ATP III and IDF criteria were found to be significantly associated with heterogeneity (P = 0.0001, P = 0.0052, respectively) (Table 3).
Significant P values: 0***, 0.001**.
Discussion
Several studies have reported the prevalence of MetS representing different population characteristics, ethnic backgrounds, locations, and so on. Consequently, studies have shown a high degree of variability in MetS prevalence. This variation could be affected by the different MetS criteria, age, and sex or even by the sampling design used. Differences in the criteria of MetS definition were observed in the literature of MetS. For example, estimated prevalence of MetS in African populations was reported to vary from as low as 0% to as high as 50% or even higher, depending on the population settings and the criteria of MetS definition used. 31 In Turkey, the MetS prevalence was found to be 36.6% according to ATP III and 44% according to IDF. 32 Furthermore, in Spain, remarkable difference in the estimated MetS prevalence was observed based on WHO (17.9%) and ATP III (23.5%) criteria. 33
This study found a combined MetS prevalence of 41% among healthy Mexican adults (Fig. 6); the frequency ranged from 31% to 54%, depending on the MetS definition used. This pooled prevalence was higher than that reported in the United States (34.2%) 34 and in Latin America (24.9%). 35 Based on the information obtained in this study from Mexico, the prevalence of MetS following different criteria was 54% for IDF, 48% for AHA/NHLBI, 36% for ATP III, and 31% for the WHO (Figs. 2 –6). Therefore, it appears that some of the differences in the reported prevalence were due to the differential diagnostic criteria for MetS.
In our meta-analysis, according to the ATP III criteria, low HDL-C was the most frequent component of MetS (53%) followed by AO (48%), which suggests an emergent need for better monitoring after diagnosis (Table 2). In Mexico, anthropometric measurements are not always part of the routine medical evaluation; it is common to check only the body mass index. However, evaluation of AO, based on waist circumference measurement, is not frequent. In a study from the United States, the most prevalent component of MetS was AO, estimating frequency of 56.1%, and this trend was much higher among adult women than men. 36 In agreement with Murguía-Romero et al., 37 low HDL-C was found to be an important component to estimate MetS prevalence among young Mexicans, showing 55% in women and 28.6% in men.
Difference between the estimated prevalence of MetS using the IDF and AHA/NHLBI criteria was very small, but the estimated values using ATP III and WHO criteria were remarkably higher. The highest estimated MetS frequency using WHO criteria might be explained by the fact of low number of studies that followed the criteria. Both studies presented big differences in the estimated MetS frequencies (13.6% and 56.3%) 25,27 (Table 2).
In our study, it was found that differences in the frequencies of the components of MetS were even greater. This might be explained, at least to some degree by the sociodemographic backgrounds of the studied populations. Another compounding factor was the difficulty in the comparability of the studies that were mostly performed in urban areas, and only two studies were carried out in rural areas. Eleven of 15 studies were performed in the central region of Mexico; this leads to an issue of unavailability of information from the other regions of the country. Only two studies included samples from the general population of Mexico. 22,27 All studies included apparently healthy individuals. No significant difference (P > 0.05) in the prevalence of MetS was found among women and men (38% and 39%, respectively).
Some of the limitations in our study are as follows: unavailability of large-scale data from different Mexican States, some studies were conducted in different population backgrounds, for example, hospital workers (nurses and physicians), and differences in the cutoff values to diagnose MetS, based on standard criteria (ATP III, IDF, WHO, and AHA/NHLBI).
Conclusion
To decrease the MetS prevalence in Mexico, early interventions in the lifestyle habits are needed and recommended. Therefore, the actions could help reducing and controlling the complications due to MetS. Particularly, CVD and T2DM are the main causes of mortality in Mexico. To the best of our knowledge, this is the first published systematic review and meta-analysis evaluating studies on the prevalence of MetS and its components, at least from healthy Mexican adult populations. This meta-analysis shows a high prevalence of MetS in healthy Mexican adults, despite the use of different criteria for MetS diagnosis. The lack of consensus on the diagnostic criteria for MetS is an important issue in this area of research. More information on the clinical criteria of the MetS components and their inter-relationships will provide greater insights into the problem, and contribute to the planning and implementation of public health strategies. Therefore, primary preventive care could be used to reduce its prevalence and impacts on human health.
Footnotes
Acknowledgment
We are very grateful to Mr. Julio Vega for helping with the statistical analysis.
Author Disclosure Statement
No competing financial interests exist.