
Abstract
Background:
The objective of this study was to evaluate the relationship between educational level as a surrogate marker of socioeconomic status and the risk of developing metabolic syndrome (MetS).
Methods:
Study subjects were 1915 Korean adults (1193 women and 722 men) who participated in a cohort study. Educational level was categorized into two groups: (1) high education (more than 12 years of education), and (2) low education (less than 12 years of education). MetS was defined according to diagnostic criteria of the National Cholesterol Education Program (NCEP-III) and the International Diabetes Federation (IDF). Multiple logistic regression analysis and Cox proportional hazard analysis were performed to evaluate cross-sectional and prospective association between MetS or MetS components and educational level after adjusting for covariates.
Results:
The overall prevalence of MetS at baseline was 15.0% in women and 20.4% in men. Incidence of MetS over 4.52 years was 16.6 per 1000 person-year in women and 27.6 per 1000 person-year in men. The prevalence and incidence of MetS were higher in the low educational group than those in the high educational group in both sexes. At baseline, the risk of MetS (odds ratio [OR]: 1.63, 95% confidence interval [CI]: 1.05–2.53 for NCEP criteria; OR: 2.30, 95% CI: 1.41–3.76 for IDF criteria) and abdominal obesity (OR: 2.62, 95% CI: 1.75–3.93) were higher in less educated women compared with those in more educated women. In men, there was no association between Mets or MetS components and educational level. Over 4.6 years of follow-up, the risk of developing MetS in women in the low education group (hazard ratio [HR]: 1.95, 95% CI: 1.12–3.50 for NCEP criteria; HR: 2.36, 95% CI: 1.14–4.86 for IDF criteria) was significantly higher than that in the high education group. In men, low education significantly increased the risk of developing impaired fasting glucose (HR: 1.95, 95% CI: 1.12–3.40).
Conclusion:
An inverse association between educational level and MetS was found in Korean women, suggesting that socioeconomic disparities might increase the risk of MetS development, especially in women.
Introduction
M
Development of MetS has been suggested to be influenced by genetic background and life style factors. 4 –7 In addition, epidemiological studies have reported an inverse association between socioeconomic status (SES) and MetS, especially in women, suggesting the presence of socioeconomic disparity in the development of MetS. 4 –7 However, relations between SES and MetS in men are inconsistent. In addition, most previous studies were conducted with cross-sectional design, which might not ensure a causal relationship between SES and MetS.
Therefore, we conducted this study in a Korean population cohort to determine cross-sectional and prospective association between MetS and educational level as a surrogate marker of SES and to clarify whether the associations differ by sex.
Methods
Subjects and study design
Study subjects are participants in the Healthy Twin Study, which has been conducted as a part of Korean Genomic Epidemiologic Study since 2005. Participants typically included twins and their first-degree family member. Details of the study protocol and design have been published in two previous studies. 8,9
A total of 3478 individuals (2059 women and 1419 men) completed baseline questionnaire and initial measurement. Details of the study protocol of the Healthy Twin Study have been previously reported. 8 Of these participants at baseline, 1563 individuals were excluded due to the following reasons: (1) follow-up measurement was not completed (782 women and 639 men); and (2) having history of cancer, myocardial infarct, or stroke (84 women and 58 men). Thus, a total of 1915 individuals (1193 women and 722 men) were included in the final analysis of this study.
Written informed consent was obtained from all participants. The study protocol was approved by Institutional Review Board of Samsung Medical Center (approval no. 2011–10-025).
Measurements
Clinical and biochemical variables were repeatedly measured at initial visit and follow-up visit. All measurement procedures were standardized across centers by training research coordinators and research assistants with a standard protocol.
Weight and height were measured using digital balance and a stadiometer with participant wearing indoor clothing without shoes, respectively. Body mass index (BMI, kg/m2) was calculated as weight in kilogram divided by height in meter squared. Waist circumference (WC) was measured at the narrowest region between the lower margin of the rib cage and the iliac crest in a standing position. Blood pressure (BP) was measured manually using a standard mercury sphygmomanometer with participant in a sitting position.
A venous blood sample was drawn after a 12-hr (overnight) fast. Serum concentrations of glucose, total cholesterol, high density lipoprotein-cholesterol (HDL-C), low density lipoprotein-cholesterol (LDL-C), and triglyceride were measured using commercial kits in a central laboratory authorized by the Korean Association of Quality Assurance for Clinical Laboratories.
MetS was defined following two different diagnostic criteria: the 2005 revised National Cholesterol Education Program's Adult Treatment Panel III (NCEP ATP III) criteria and the criteria of the International Diabetes Federation (IDF). 10,11
Among several indicators of SES such as education, housing condition, income, and occupation, 12,13 educational level was selected as an indicator of SES for this study considering the following distinctive features of educational level: (1) it reflects SES in early life; (2) it has a role as a determinant of future occupation and income; and (3) it hardly changes during life. In addition, it is relatively easier to measure educational level than to measure other SES indicators using a questionnaire. 12
In this study, educational level, smoking status, alcohol consumption, regular exercise, and dietary intake information were obtained using a self-administered and structured questionnaire. In Korea, the public educational system is composed of 6-year elementary school, 3-year of middle school, 3-year of high school, and 2 to 4-year of college or university. We categorized educational level into two groups (<12 years or ≥12 years of school education) based on the educational system in Korea and the distribution of educational level among study subjects. Thus, 12 years of education corresponds to graduating from high school.
Smoking status was classified into three groups: never smoker (smoke less than 20 packs during whole life), ex-smoker, and current-smoker. Alcohol consumption was categorized into three groups: never drinker, ex-drinker, and current-drinker. Physical exercise was categorized into three groups depending on the frequency of moderate intensity exercise in a week (none, once or twice, and three times or more). Daily caloric intake was evaluated using a validated 103-item semi-quantitative food frequency questionnaire. 14
Statistical analysis
Metabolic and lifestyle characteristics were compared between the two educational groups for each sex by analysis of covariance (ANCOVA) test after incorporating age as a covariate for continuous variable and by chi-square test after age standardization for categorical variable. Direct age standardization was performed for categorical variables using the Korean Population Census data of 2010 as a reference population to eliminate the influence of imbalanced age distribution between educational groups.
The risk of having a MetS and each metabolic component was evaluated at baseline for the low educational group compared with that for the high educational group using logistic regression analysis after adjusting for covariates. For this analysis, age was adjusted in model 1. Smoking, alcohol, exercise, and total calorie intake were additionally adjusted in model 2.
Longitudinal change of each metabolic component between initial and follow-up visits was assessed and the extent of change between the two educational groups was compared by Student's t-test. Before conducting t-test, age-adjusted residual values of longitudinal changes in metabolic components and number of metabolic components were calculated using linear regression analysis. For this analysis, some participants who had abnormality in relevant metabolic components at baseline survey were excluded. The risk of developing MetS and abnormality in each metabolic component associated with lower level of education was evaluated for participants who were longitudinally followed using age-adjusted and multivariable-adjusted Cox proportional hazard model.
To examine whether the associations between MetS and SES differs by sex, we conducted all analyses in men and women separately. All analyses were performed using PASW Statistics 21.0 software (SPSS, Inc., Chicago, IL). For all analyses, a P-value of less than 0.05 was considered statistically significant.
Results
Age-adjusted metabolic and lifestyle characteristics measured at baseline by educational level for each sex are shown in Table 1. The mean age of the high educational group (women: 39.3 years, men: 42.4 years) was lower than that of the low educational group (women: 57.7 years, men: 55.8 years) in both sexes. In women, BMI, WC, triglyceride level, and HOMA-IR index were higher in the low educational group than those in the high educational group. However, HDL-C level and total calorie intake were lower in the low educational group than those in the high educational group in women. Current smoking and frequent exercise were more prevalent in less educated women. In men, systolic BP and the prevalence of smoking were higher in the low educational group than those in the high educational group while current alcohol consumption and frequent exercise were lower in the low educational group than those in the high educational group.
Data were presented as mean (standard error) for continuous variables and percentage for categorical variables.
P value were obtained by t-test for age, by ANCOVA test for continuous variables after adjusting for age, and by Mantel-Haenszel chi-square test for categorical variables after direct age standardization.
ANCOVA, analysis of covariance; DBP, diastolic blood pressure; HDL-C, high density lipoprotein cholesterol; HOMA-IR, homeostatic model assessment-insulin resistance; LDL-C, low density lipoprotein cholesterol; SBP, systolic blood pressure; WC, waist circumference.
Overall prevalence at baseline was 15.0% in women and 20.4% in men. Table 2 shows the prevalence of MetS in each educational group and the association between educational level and MetS at baseline examination. The prevalence of MetS by NCEP criteria in women was 8.7% for the high educational group and 33.2% for the low educational group. The prevalence of MetS by NCEP criteria in men was 18.6% for the high educational group and 28.0% for the low educational group. In women, the risk of having abnormal WC or MetS by IDF criteria was significantly higher in the low educational group compared with that in the high educational group in age-adjusted model. The association between low education and the risk of having abnormal WC or MetS became stronger after adjusting for age, smoking, alcohol, exercise, and total calorie intake. However, education level had no significant association with MetS or any metabolic component in men.
Odds ratio (95% CI) was estimated by multiple logistic regression analysis with higher (>12 years) educational group as a reference. In model 1, age was adjusted. In model 2, age, smoking, alcohol, physical exercise, and total calorie intake were adjusted.
CI, confidence interval; DBP, diastolic blood pressure; HDL-C, high density lipoprotein cholesterol; IDF, International Diabetes Federation; NCEP, National Cholesterol Education Program; OR, odds ratio; SBP, systolic blood pressure; WC, waist circumference.
Results of longitudinal changes in the level of metabolic components by educational level during the follow-up in a cohort of subjects who had no abnormality in relevant metabolic component at baseline are shown in Table 3. The mean follow-up duration was 4.6 years for women and 4.4 years for men. There was no significant difference in follow-up duration between the high and the low educational groups in either sex. In women, both systolic and diastolic BP were increased over time in the low educational group. However, they were decreased over time in the high educational group. In addition, the increase in the number of abnormal metabolic components by NCEP criteria was significantly greater in the low educational group than that in the high educational group. In men, there was no significant difference in longitudinal change between the two educational groups for any metabolic component.
Varies because the numbers of subjects who had abnormal level at baseline were inconsistent across each metabolic component.
P value for the difference in the age-adjusted residual values of longitudinal change between the two educational groups was assessed by t-test. Age-adjusted residual values were calculated using the linear regression analysis.
HDL-C, high density lipoprotein cholesterol; IDF, International Diabetes Federation; NCEP, National Cholesterol Education Program; SD, standard deviation; WC, waist circumference.
Overall incidence of MetS over 4.52 years was 16.6 per 1000 person-year in women and 27.6 per 1000 person-year in men. The risk of developing MetS and abnormality in each metabolic component in the low educational group compared to that in the high educational group is shown in Table 4. The incidence of MetS by NCEP criteria in women was 10.4 per 1000 person-year for the high educational group and 41.6 per 1000 person-year for the low educational group. In men, the incidence of MetS by NCEP criteria was 25.9 per 1000 person-year for the high educational group and 36.5 per 1000 person-year for the low educational group. In women, the risk of developing MetS by NCEP criteria and IDF criteria was increased by 1.84 and 2.30 times, respectively, in the low educational group after adjusting for age and baseline level of each metabolic component. When smoking, alcohol, physical exercise, and total calorie intake at baseline were additionally adjusted, the association between education and MetS became more evident. In men, the risk of developing MetS was not associated with educational level. Meanwhile, the risk of developing abnormality in metabolic components such as high fasting glucose and low HDL-C in men was significantly increased in the low educational group after adjusting for age and baseline level of metabolic components. However, after adjusting for smoking, alcohol, physical exercise, and total calorie intake at baseline, only the risk of developing high glucose level remained significant in men.
Hazard ratios (95% CI) were estimated by Cox proportional hazard analysis after adjusting for covariates.
In Model 1, age and the level of relevant metabolic component at baseline were adjusted. In Model 2, age, the level of relevant metabolic component, smoking, alcohol, physical exercise, and total calorie intake at baseline were adjusted.
CI, confidence interval; DBP, diastolic blood pressure; HDL-C, high density lipoprotein cholesterol; HR, hazard ratio; IDF, International Diabetes Federation; NCEP, National Cholesterol Education Program; SBP, systolic blood pressure; WC, waist circumference.
As shown in the Kaplan–Meier curve (Fig. 1), the probability of developing MetS was significantly higher in the low educational group than that in the high educational group over the follow-up time in women. However, this was not evident in men.
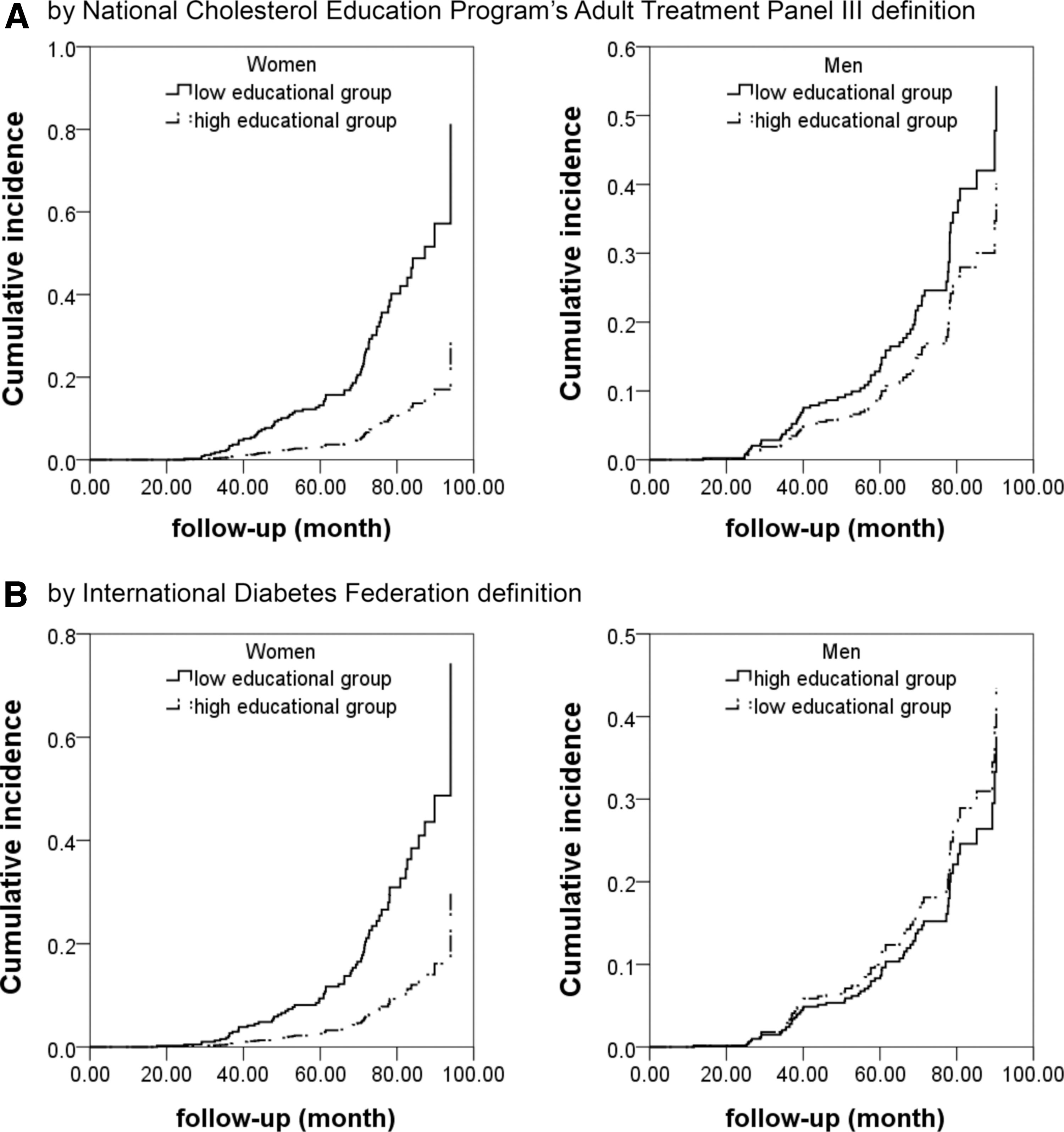
Kaplan–Meier curves for cumulative incidence of metabolic syndrome according to educational level over follow-up time.
Discussion
In this cohort study of Korean adults, we found that low educational level was associated with increased risk of prevalent and incidental MetS in women. We believe that the prospective design of this study could provide stronger evidence for the association between SES and MetS than cross-sectional studies.
It seems interesting that the relationship between SES and MetS differed by sex in both cross-sectional and prospective analyses of this study. However, the relationship between SES and MetS has been consistently found in other studies conducted in China, Poland, and Korea. 7,15 –17 A cross-sectional study 15 has found that lower educational level is associated with higher risk of MetS in Chinese women, but not in Chinese men. In another cross-sectional study, 7 the risk of MetS is also inversely associated with educational level only in women. Similarly, in a cross-sectional Korean study, educational level is negatively associated with MetS only in women. 16 Recently, Seo et al. 17 have performed a prospective study to evaluate the association of SES measured by educational level and income with the incidence of MetS in a Korean population cohort. In their study, the incidence of MetS was inversely associated with both educational level and income in women, but not in men. 17 The prospective study by Seo et al. 17 has some strength than our study, including its larger study size (2733 men and 2811 women), longer follow-up duration (mean of 6.01 years), and the use of more diverse SES marker (educational level and income). However, their study only included middle-aged population. In addition, baseline levels of metabolic components were not considered. Moreover, changes in metabolic components from baseline were not reported. Given the significant difference in baseline levels of several metabolic components between the low and high educational groups found in this study, especially in women, analysis without considering baseline levels of metabolic components might result in biased results.
Since MetS is a cluster of abnormality in several metabolic components, it might be necessary to examine relations between SES and each metabolic component to better understand the underlying mechanism of the SES-MetS relationship.
Several studies have investigated the relationship between SES and obesity. 18 –20 Interestingly, a study in French population has revealed that the prevalence of obesity is different by educational level in women while such difference is present by occupation in men. 18 A cross-sectional study in Chinese population has found that SES is positively associated with obesity in men whereas an inverse association is found in women. 19 Similarly, in a cross-sectional study of Korean population, educational level is found to be inversely associated with BMI in women, but not in men. 20 In our study, although an inverse association between educational level and abdominal obesity in women was found in cross-sectional analysis of baseline data, there was no difference in prospective change of WC between the low and high educational groups. Despite the consistent inverse relation between SES and MetS across several cross-sectional studies, the consistency in findings between cross-sectional and cohort study found in our study seems to negate the significant influence of SES on the progression of abdominal obesity in adulthood.
Several studies have reported the relationship between educational level and hypertension. 21 –23 Conen et al. have shown that educational level is inversely associated with the incidence of hypertension in women. 21 In a study by Baek, 22 the incidence of hypertension is found to be higher in less educated women than that in more educated women whereas educational level is not associated with the incidence of hypertension in men. A study in a Thailand population has also found an inverse association between educational level and the incidence of hypertension. 23 However, in our study, high BP was not associated with educational level in cross-sectional or follow-up study after adjusting for covariates, although the extent of BP increase during follow-up was higher in the low educational group than that in the high educational group in women.
Several studies have reported an inverse association between SES and diabetes. 5,24 In a cohort study in the United Kingdom, the incidence of type 2 diabetes mellitus (DM) has been found to be higher in the lower SES group that that in the higher SES group. 24 Another cohort study on the relationship between DM and SES conducted in U.S. women has also revealed that the risk of incident DM is lower in people with higher educational level. 5 Our study also found an increased risk of developing impaired fasting glucose in the lower educated group, although the finding was limited to men. Considering differences in cut-off level for diagnosis between DM and impaired fasting glucose, we could not directly compare findings of our study with findings of other studies. 5,24
The relation between dyslipidemia and SES has been scarcely evaluated. A cross-sectional study in Korean adults has shown that the association between SES and dyslipidemia is inverse in women but positive in men. 25 However, we found that low HDL-C or hypertriglyceridemia was not associated with educational level in cross-sectional or longitudinal analysis.
The significant inverse association between educational level and MetS in women without significant association between SES and each component of MetS was unexpected. This finding suggests that abnormal metabolic components are more likely to be clustered in less educated women. This hypothesis is compatible with findings regarding the number of abnormal metabolic components. In this study, the number of metabolic components was about twofold higher in less educated women at follow-up and change in the number between baseline and at follow-up was about eightfold higher in less educated women.
Several possibilities might explain the association between educational level and MetS. First, education is one of the important factors that determine life-style behavior of an individual. 12 Well-educated people are less likely to have adverse health behaviors as found in our study and adverse health behaviors are closely associated with the risk of MetS occurrence. However, results of our study showed that the inverse association between educational level and the risk of MetS persisted even after adjusting for lifestyle behaviors, suggesting that other factors might also contribute to the association between educational level and MetS. Second, educational level could be closely related to accessibility to medical care system and economically advantageous surroundings. These factors also have relations with the development of abnormal metabolic components. In this study, we could not examine such mechanism due to the lack of available data. Third, low SES might be related to higher cortisol secretion because people with lower SES are more likely to be exposed to higher stress than people with higher SES. Stress could cause perturbation of hypothalamus-pituitary-adrenal axis that regulates cortisol secretion. Increased cortisol level may increase the risk of visceral fat accumulation. Through such neuroendocrine-autonomic dysregulation, socioeconomic handicaps may cause central obesity, one of the main components of MetS. 26 –29 Fourth, interaction with mother from childhood to adolescence might play a role in the relationship between SES and MetS. Well-educated mothers may know better about nutrition, physical activity, and other aspects related to MetS. 30 Therefore, they are more likely to bring up their children with healthy lifestyle to prevent MetS. Given that educational level of an individual tends to reflect his/her parental SES, more educated people might have well-educated mothers and desirable propensity about MetS. 12 Gender differences in the relationship between MetS and SES might be related to the attitude of parents. Maternal attitude toward obesity control has been found to be influential to women, but not to men. 31
Our study has a few limitations. First, the number of participants with very high or very low educational level was insufficient. In addition, the categorization of educational level was quite rough. Thus, the association between educational level and MetS might have been underestimated. Second, we selected educational level as an index of SES because around half of women participants in our study were not involved in economic activity. Educational level, an index of SES selected for our study, might not be the best SES indicator. However, educational level tends to be considered as a more constant and more accurate measure of lifelong social status than job or family income. 32 Third, although we adjusted health-related behaviors, residual confounding by unmeasured factors might still be possible, which might bias findings of this study. Fourth, information on amount of alcohol consumption was unavailable in our data, although alcohol behaviors were adjusted by dividing subjects into three groups (never, past, and current).
Conclusion
This cohort study of Korean population revealed differential association between educational level and the risk of MetS in both sexes. The risk of MetS development was increased in women with low educational level compared with that in women with high educational level. This finding suggests that there is a socioeconomic disparity in the development of MetS, especially in women. Therefore, more efforts might be needed to reduce the risk of MetS development in people with low SES, especially in women.
Footnotes
Acknowledgment
This research was supported by a grant (2014R1A2A2A01002705) of the Basic Science Research Program through the National Research Foundation (NRF) funded by the Ministry of Science, ICT and future Planning, Republic of Korea.
Author Disclosure Statement
No competing financial interests exist.