
Abstract
Background and Aims:
Saxagliptin as one of dipeptidyl peptidase-4 (DPP-4) inhibitors can effectively improve glycaemic control in type 2 diabetes mellitus, and nesfatin-1 is regarded as a very important factor in regulating feeding behavior and energy homeostasis. In this trial, we observed the effect of saxagliptin on regulating nesfatin-1 secretion and ameliorating insulin resistance and metabolic profiles in type 2 diabetes mellitus.
Methods:
One hundred two type 2 diabetes participants (M/F = 48/54) were investigated. Fifty-one (M/F = 24/27) of them as the treatment group were treated with oral glucose-lowering agents including saxagliptin, the other 51 (M/F = 24/27) as the control group were treated with oral glucose-lowering agents excluding any DPP-4 inhibitors. The parameters of serum nesfatin-1, C-peptide, homeostasis model assessment-β (HOMA-β) function, HOMA insulin resistance (HOMA-IR), glycosylated hemoglobin A1c (HbA1c), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), body mass index (BMI), and blood pressure (BP) at baseline, month 3, 6, and 12 were observed and compared respectively.
Results:
Saxagliptin significantly upregulated nesfatin-1 secretion (P < 0.001 at 3-, 6-, and 12-months vs. baseline), increased serum C-peptide (P < 0.05, 0.001, and 0.001 at 3-, 6-, and 12-months vs. baseline), improved HOMA-IR and function of HOMA-β (P < 0.001 at 3-, 6-, and 12-months vs. baseline) and metabolic profiles (P < 0.001 with HbA1c at 3-, 6- and 12-months; P < 0.001 with LDL-C at 6- and 12-months; P < 0.001 and 0.01 with HDL-C at 6- and 12-months vs. baseline), declined BMI (P < 0.05 at 6- and 12-months vs. baseline) and BP (P < 0.001 with systolic BP (SBP), and mean BP at 6- and 12-months, P < 0.01 with diastolic BP at 6- and 12-months vs. baseline).
Conclusions:
Saxagliptin could upregulate nesfatin-1 secretion and ameliorate insulin resistance and metabolic profiles in type 2 diabetes mellitus. Saxagliptin had the potential to play fundamental by upregulating nesfatin-1 secretion besides lowering glucose by inhibiting the degradation of glucagon-like peptide-1.
Introduction
A
Nesfatin-1, which was initially identified in rats, is composed of 82 amino acids and derived from a nucleobindin 2 (NUCB2) precursor. 8 NUCB2 mRNA and nesfatin-1-immunoreactive neurons are regulated by fasting and refeeding. 9 Nesfatin-1 is considered a feeding regulator and has the ability to suppress food intake, which can be blocked by the administration of anti-nesfatin-1 antibody. 8 Nesfatin-1 plays a pivotal role in postprandial glucose regulation by inhibiting feeding, gastric emptying, gastric contractions, and inter-digestive migrating contractions. 9 There have been controversial results regarding the nesfatin-1 levels in diabetic patients, and significantly lower fasting plasma nesfatin-1 levels were reported in type 2 diabetes patients, 10 whereas higher plasma levels of nesfatin-1 in newly diagnosed type 2 diabetes patients were reported too. 11
Methods
Participants and study design
Figure 1 shows the number of participants screened. To investigate the effect of saxagliptin on regulating nesfatin-1 secretion and ameliorating insulin resistance and metabolic profiles, n = 102 Han Chinese type 2 diabetes participants (M/F = 48/54) were assessed for eligibility from the Out Patient Department from February 2012 to March 2015. According to gender, duration of disease, and age, they were divided into treatment group (n = 51, M/F = 24/27) with saxagliptin (5 mg every day) (Bristol-Myers Squibb Company, NJ) and metformin, and a control group (n = 51, M/F = 24/27) with acarbose and metformin. All participants were treated with lifestyle modification for diet and exercise at the same time.
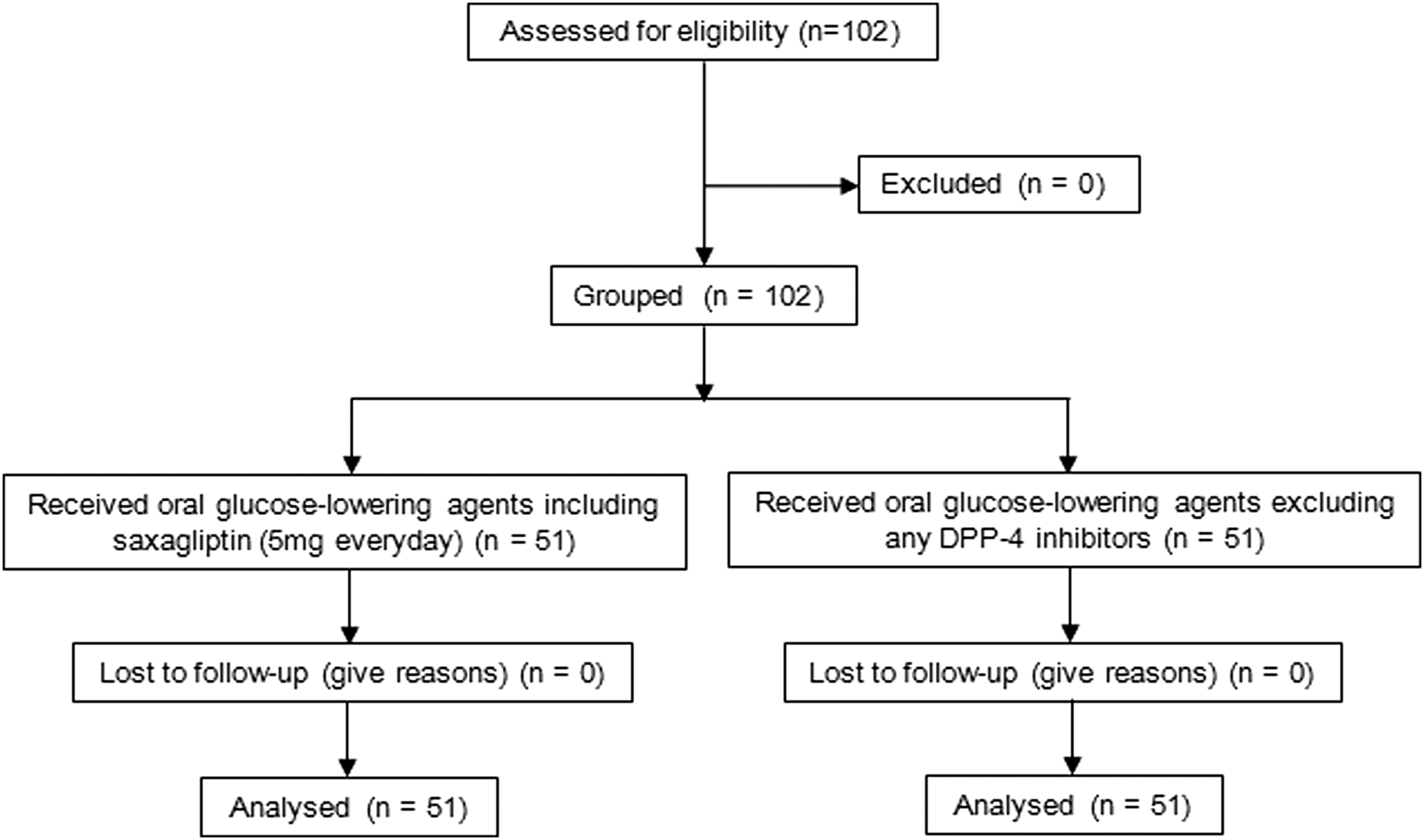
Flow chart of study protocol.
Diagnostic criteria for type 2 diabetes were fasting glucose level ≥7.0 mmol/L or 2-h postprandial plasma glucose level ≥11.1 mmol/L or glycosylated hemoglobin A1c (HbA1c) levels ≥6.5%. 12 Inclusion criteria for the study were HbA1c levels 7.0%–8.5%. Exclusion criteria included allergy or hypersensitivity to any of the drug's components, established cardiovascular disease (patients at least 40 years of age and had a history of a clinical event associated with atherosclerosis involving the coronary, cerebrovascular or peripheral vascular system), heart failure NYHA class III and IV, eGFR <90 mil/min/1.73 m2, child B/C with liver function, malignant disease, active infectious disease, pregnancy, or breastfeeding.
We confirm that all methods were performed in accordance with the relevant guidelines and regulations.
Anthropometry
Height and weight were obtained using standardized conventional methods while the participant was standing erect and barefoot. Body mass index (BMI) was calculated as weight in kilograms (kg) divided by height in squared meters (m2). Right brachial artery BP in the recumbent position of each participant was taken 30 min after complete rest using a standardized mercurial sphygmomanometer.
Sampling procedures
After overnight fasting (for at least 8 hr), blood samples were drawn by standard cubital venipuncture at 8:00 am at inclusion and after 3-, 6-, and 12-months of follow-up. Serum and plasma for determination of selected parameters were prepared by centrifugation within 1 hr at 2500 g for 10 min and 4°C at 3000 g for 20 min, respectively. The samples were stored at −70°C until analyses.
Laboratory analyses
Serum nesfatin-1 was detected by sandwich EIA utilizing the commercial enzyme-linked immunosorbent assay kit (IBL-AMERICA) (Bio-Rad 680, IDS) according to the manufacturer's instructions. The EIA kit showed high specificity for nesfatin-1 but no cross-reactivity with ghrelin, angiotensin, visfatin, or NUCB2. Serum connecting peptide (C-peptide) and insulin were tested with chemiluminescence (Light Emitting Device E170, Roche Chemistry), HbA1c was identified with HPLC (HLC-723G7, TOSOH), and other parameters were investigated with immune scattering turbidimetry (Roche P800 automatic biochemical analyzer, Roche Chemistry).
The homeostasis model assessment for insulin resistance (HOMA-IR) was calculated as fasting insulin (IU) × fasting glucose (mmol/L)/22.5, and HOMA-β function (%) was calculated as 20 × fasting insulin (IU)/(fasting glucose-3.5). 13 All participants completed the full 52-week observation.
Statistical analysis
Sample size was based on a trial by von Hurst et al. 14 The results were expressed as the mean ± standard deviation. Variables exhibiting a non-Gaussian distribution were logarithmically transformed. Paired t-test within group and independent t-test between groups were undertaken to compare values over time. All statistical comparisons were performed with the Statistical Package for the Social Sciences 22.0 (SPSS, Inc.). Differences were considered to be statistically significant when P < 0.05.
Results
The characteristics of participants were shown in Table 1, parameters of all type 2 diabetes mellitus participants according to follow-up were presented in Table 2, the changes of parameters between the treatment and control groups were displayed in Table 3. There were no significant differences in the parameters between the treatment and control groups at baseline.
BMI, body mass index; CP, connecting peptide; DBP, diastolic blood pressure; HbA1c, glycosylated hemoglobin A1c; HDL-C, high-density lipoprotein cholesterol; HOMA-IR, homeostasis model assessment-insulin resistance; LDL-C, low-density lipoprotein cholesterol; MBP, mean blood pressure; SBP, systolic blood pressure.
P < 0.05, # P < 0.01, & P < 0.001 (compared with baseline).
P < 0.05, β P < 0.01, γ P < 0.001, δ P = 0.001 (compared with group control).
Corrected netatin-1, corrected for the change of BMI = Nesfatin-1/BMI.
P < 0.05, # P < 0.01, $ P = 0.001, & P < 0.001 (compared with control group).
Group C, control group; Group T, treatment group.
Compared with baseline according to follow-up, saxagliptin significantly upregulated nesfatin-1 secretion, increased serum C-peptide, improved HOMA-IR and the function of HOMA-β and metabolic profiles of glucose and lipids, and decreased BMI and BP.
Compared with baseline according to follow-up in control group, nesfatin-1 secretion decreased but the differences were not significant; serum C-peptide and the function of HOMA-β decreased and HOMA-IR increased significantly at 12-months respectively; Subtle changes were found in BP.
The differences of the levels of serum nesfatin-1, serum C-peptide, HbA1c, lipids, and mean BP at 12-months were significant compared with control group. The differences in changes of parameters between treatment and control groups were significant according to follow-up.
Discussion
There have been no studies regarding the effect of saxagliptin on regulating nesfatin-1 secretion, and our research indicated for the first time that in type 2 diabetes mellitus, saxagliptin upregulated nesfatin-1 secretion, which might improve metabolism in these patients.
As a DPP-4 inhibitor, saxagliptin effectively modulated glucose metabolism by selectively inhibiting the catalysis of DPP-4. A major mechanism of DPP-4 inhibitors was increased concentrations of biologically activated GLP-1 and GIP over 24 hr. 15 GLP-1, which is secreted by L-cells in the distal gut and quickly deactivated by DPP-4, is a serine-type protease composed of 766 amino acid and found in many tissues. 16 GLP-1 increases the cAMP levels, insulin mRNA, insulin release, 15 β-cell proliferation and resistance to apoptosis, 17 inhibits glucagon secretion 2 and gastric emptying, 18 promotes glucose disposal in peripheral tissues, decreases feelings of hunger, and reduces energy intake. 19 Clinical research on type 2 diabetes has shown that a DPP-4 inhibitor could improve β cell activity and insulin release, 2 reduce the inactive-insulin to active-insulin ratio, 20 and suppress glucagon release and hepatic glucose production. 2 All of these effects of DPP-4 inhibitors might be mediated by GLP-1.
Although DPP-4 inhibitors were thought to lower weight-neutral glucose, regardless of whether they were used as mono-therapy or adjuvant therapy, 21 our research indicated that saxagliptin reduced BMI and improved lipid metabolism, which were postulated to be caused by improved insulin resistance, inhibited intestinal triglyceride absorption, promoted chylomicron triglyceride clearance, 22 increased lipid metabolism, reduced lipoprotein secretion, 23 and decreased palatable food intake via GLP-1 suppression of the mesolimbic dopamine signaling pathway. 24 Nonetheless, these proposed mechanisms have not been elucidated. We hypothesize that these effects of saxagliptin on weight loss and lipid metabolism improvement are also correlated with upregulated nesfatin-1 secretion, but the underlying mechanism remains to be further investigated.
Nesfatin-1 was widely expressed in a rat hypothalamic nuclei 8 and peripheral cells. 25 Research revealed that nesfatin-1 played a pivotal role in regulating insulin secretion, glucose homeostasis, and whole-body energy balance. Nesfatin-1 could potentiate glucose-induced insulin secretion and improve insulin sensitivity by promoting Ca2+ influx via L-type Ca2+ channels, independent of protein kinase A and phospholipase A(2). 26,27 As a satiety molecule in the hypothalamus, nesfatin-1 reduced cumulative and dark-phase food intake via a corticotropin-releasing factor 2 [CRF(2)]-receptor-dependent pathway. 20,26 The satiety effect was associated with melanocortin signaling, 28 which was mediated by leptin, 29 thereby increasing the corticotropin releasing hormone, thyrotropin releasing hormone levels, and histamine turnover. 30 As an emptying suppressor, nesfatin-1 not only inhibited gastric emptying but also reduced gastric contractions, especially cyclical interdigestive migrating contractions, in the fasted state. 9,26 Nesfatin-1 could also increase spontaneous physical activity, whole-body fat oxidation and the carnitine palmitoyltransferase I mRNA levels in brown adipose tissue, 26 and stimulate free fatty acid utilization in skeletal muscle via the AMPK-ACC pathway. 31 In addition, nesfatin-1 has the ability to upregulate preproglucagon mRNA/GLP-1 and GIP mRNA/GIP secretion in STC-1 cells. 32 These effects of nesfatin-1 contribute to weight loss, lipid improvement, and improved glucose metabolism in type 2 diabetes mellitus. Although saxagliptin upregulated nesfatin-1 secretion, and serum nesfatin-1 was negatively correlated with BMI neither in the treatment nor control group, as reported previously for BMI in obese children, 33 these effects of saxagliptin are not certainly correlated with upregulated nesfatin-1.
There have been controversial clinical results of nesfatin-1 levels in type 2 diabetes. Reductions in both nesfatin-110 and islet NUCB2 mRNA 34 in type 2 diabetes mellitus were reported, and elevated plasma nesfatin-1 was found in subjects with impaired glucose tolerance and patients with newly diagnosed type 2 diabetes mellitus. 11 Nevertheless, our current research indicated that the serum nesfatin-1 levels were negatively correlated with HOMA-IR and HbA1c and positively correlated with HOMA-β function and serum C-peptide in both the treatment and control groups. Saxagliptin could upregulate nesfatin-1 in the treatment group but not in the control group, which might explain the role of saxagliptin in improving glucose metabolism in type 2 diabetes.
Some researchers have reported that nesfatin-1 could increase BP by impairing sodium nitroprusside-induced cyclic guanine monophosphate production and decreasing the plasma levels of endothelial nitric oxide (NO) synthase. 35 The fasting plasma nesfatin-1 levels were significantly higher in hypertensive patients, especially in overweight/obese hypertensive patients, and could be a risk factor for obesity-associated hypertension. 36 But our research indicated that saxagliptin could upregulate nesfatin-1 secretion in type 2 diabetes mellitus, and the levels of nesfatin-1 were negatively correlated with BP. Besides the effect of upregulating nesfatin-1 secretion, saxagliptin could increase NO bioavailability, 37 improve NO release, reduce inflammation, 38 decrease peripheral vascular resistance, 39 and increase left ventricular function. 40 All these roles above and the effects of saxagliptin on ameliorating insulin resistance and metabolic profiles, reducing body weight might contribute to lower BP.
Conclusions
Taken together, we concluded that saxagliptin upregulated nesfatin-1 secretion; improved β-cell function, insulin resistance, and metabolic profiles of glucose and lipids; and lowered BMI and BP in type 2 diabetes mellitus. As a DPP-4 inhibitor, saxagliptin has the potential to play fundamental roles in type 2 diabetes mellitus by upregulating nesfatin-1 secretion and lowering glucose by inhibiting the degradation of GLP-1. It is still unknown how saxagliptin upregulates nesfatin-1 secretion and whether the increased level of nesfatin-1 was caused by increased GLP-1 or was the direct effect of saxagliptin. Previous research using STC-1 cells showed that nesfatin-1 increased GLP-1 and GIP secretion. 35 More investigations should be done to probe the role of DPP-4 inhibitors and the underlying mechanisms of nesfatin-1 in type 2 diabetes mellitus.
Study limitations
There are several important limitations of our study. First, the participants assessed in this study were only Han Chinese, it was unknown whether the effect of saxagliptin on nesfatin-1 secretion in type 2 diabetes mellitus was different or not in different ethnic groups. Second, this study was a clinical trial focused on the effect of saxagliptin on regulating nesfatin-1 secretion, the mechanism of this effect is unknown and needs to be investigated.
Ethics approval and consent to participate
Ethical approval was obtained from the Medical Ethics Committee of Jiangsu Jiankang Vocational College and informed consent was obtained from each patient.
Clinical trials registration
At the time of publication, the authors became aware that the trial must be recognized by the WHO International Clinical Trials Registry Platform, hence the delay in the registration of this study with
Consent for publication
All the authors involved have signed the consent for publication.
Availability of data and material
The data in this trial were partly restricted because of participant privacy.
Footnotes
Authors' Contributions
K.C. conceived the study, and participated in its design and coordination, and helped to draft the article. K.C., T.Z., J.W., and Q.M. carried out examinations. K.C., T.Z., J.W., and Q.M. were involved in drafting the article or revising it critically. All authors read and approved the final article.
Author Disclosure Statement
No conflicting financial interests exist.