
Abstract
Background:
To examine the relationship between platelet count and insulin resistance, as measured by a homeostasis model assessment of insulin resistance (HOMA-IR), in a nationally representative sample of Korean adolescents.
Methods:
The study population comprised 1133 participants (636 male and 497 female participants) aged 12–18 years selected from the 2008–2010 Korea National Health and Nutrition Examination Survey. Insulin resistance was defined as a HOMA-IR value greater than the 85th percentile. The odds ratios (ORs) and 95% confidence intervals (95% CIs) for insulin resistance were calculated using multiple logistic regression analysis.
Results:
The mean values of insulin and HOMA-IR increased proportionally with platelet count quartiles for all, male, and female participants. The prevalence of insulin resistance increased significantly with an increase in platelet count quartiles in all, male, and female participants. Compared with the ORs for individuals in the lowest platelet count quartile, the ORs (95% CIs) for insulin resistance in individuals in the highest quartile was 2.90 (1.39–6.07) for all, 2.98 (1.14–8.31) for male, and 2.14 (0.88–5.32) for female participants, after adjusting for age, gender (for all participants), household income, residential area, family history of diabetes mellitus, and overweight [85th percentile ≤ body mass index (BMI) <95th percentiles for age and gender] or obesity (BMI ≥95th percentile).
Conclusion:
Platelet count was positively associated with insulin resistance in Korean adolescents. These findings suggest that platelet count could be a useful indicator for identifying adolescents with insulin resistance.
Introduction
I
Only a few standard methods for quantifying insulin resistance exist. Although the homeostasis model assessment of insulin resistance (HOMA-IR) is used for this purpose, the measure is not routinely utilized in clinical practice. Therefore, a simple and more accessible marker for predicting insulin resistance would be useful for early identification of individuals with insulin resistance. Emerging evidence also suggests that some hematologic parameters may be useful for identifying adults who are susceptible to cardiovascular disease and insulin resistance. 11,12 Among the different aspects of a complete blood count, the platelet count is affordable and easy to interpret, and the measure is ordered routinely in clinical practice. Previous studies have shown that higher platelet counts, even within the normal range, are related to insulin resistance in adult populations. 13 –15 However, very few studies have evaluated the association between platelet count and insulin resistance in a general pediatric population. Therefore, in this study, we investigated whether platelet count is associated with insulin resistance, as measured by HOMA-IR, in a nationally representative sample of Korean adolescents.
Methods
Survey overview and study population
In this cross-sectional study, we used data acquired from the 2008–2010 Korea National Health and Nutrition Examination Survey (KNHANES), which is performed by the Korea Centers for Disease Control and Prevention. KNHANES is a nationwide, representative, population-based survey conducted to assess the health and nutritional status of Koreans. The survey comprises three components: health interview, health examination, and nutrition survey. From 2008 to 2010, the target population of the survey was noninstitutionalized civilians residing in South Korea. The sampling units comprised households that were selected through a stratified multistage probability sampling design based on geographic location, age, and gender distribution. Sampling weights, which were representative of the probability of being sampled, were assigned to each participant to ensure that the results represented the overall South Korean population.
In total, 29,235 participants were included in the 2008–2010 KNHANES, which included data from 2728 adolescents aged 12–18 years. Of these 2728 adolescents, we excluded those who had not fasted for 8 hr before blood sampling (n = 269) and those with missing data for fasting plasma glucose, insulin, and/or platelet count (n = 1177). Of the remaining subjects, those meeting any of the following criteria were excluded (n = 147): anemia according to age and gender, platelet count <150,000/mL or >400,000/mL, and leukocyte count <4000 cells/μL or ≥10,000 cells/μL. Participants with a plasma glucose level ≥126 mg/dL and/or a history of diabetes mellitus were also excluded (n = 2). After these exclusions, 1133 participants (636 male and 497 female participants) were included in the final analysis. The KNHANES was approved by the Institutional Review Board of the Korea Centers for Disease Control and Prevention (approval numbers: 2008-04EXP-01-C, 2009-01CON-03-2C, and 2010-02CON-21-C). In addition, this study complied with the ethical principles of the Declaration of Helsinki.
Measurement of anthropometric and laboratory data
At the time of the 2008–2010 KNHANES, survey recipients were informed that their household had been chosen randomly for voluntary participation in a nationwide representative survey performed by the Korea Centers for Disease Control and Prevention, and that they had the right to withdraw at any time in accordance with the National Health Enhancement Act supported by the National Statistics Law of Korea. Written informed consent was acquired from all participants who agreed to participate. Blood tests were performed for participants aged ≥10 years, and consent was obtained to use the blood samples in further studies.
Trained medical staff conducted anthropometric measurements in accordance with a standardized procedure. Weight and height were measured to the nearest 0.1 kg and 0.1 cm, respectively, with participants wearing light indoor clothing and no shoes. Body mass index (BMI) was calculated as weight (kg) divided by the square of height (m2). Systolic and diastolic blood pressures were measured three separate times at 5-min intervals with a standard mercury sphygmomanometer (Baumanometer; W.A. Baum Co., Inc., Copiague, NY), and the mean of the second and third measurements was used for analysis.
Blood samples were collected from the antecubital vein after each participant had fasted overnight for a minimum of 8 hr. Platelet and leukocyte counts were obtained using an automated blood cell counter (XE-2100D; Sysmex, Kobe, Japan). Fasting serum insulin levels were measured using a 1470 WIZARD gamma-counter (PerkinElmer, Turku, Finland). Fasting plasma glucose, total cholesterol, high-density lipoprotein cholesterol, and triglycerides levels were measured with an Automatic Analyzer (Hitachi 7600; Hitachi Co., Tokyo, Japan).
Definitions of terms
Overweight was defined as 85th percentile ≤ BMI <95th percentiles for age and gender, and obesity was defined as BMI ≥95th percentile for age and gender according to the 2007 Korean Children and Adolescents Growth Standard. 16 HOMA-IR was determined using the following equation: fasting plasma glucose (mg/dL) × fasting insulin (μIU/mL)/405. In this study, insulin resistance was defined as a value greater than the 85th percentile of HOMA-IR (>3.86 in all, >3.86 in male, and >3.85 in female participants). Family history of diabetes was defined as having at least one parent with diabetes mellitus.
Statistical analysis
Sampling weights were used to account for the complex design of the KNHANES. Accordingly, we obtained valid estimates that represented all Korean adolescents, and avoided biased estimates. Platelet count quartiles were categorized as follows: Q1, ≤240; Q2, 241–271; Q3, 272–305; and Q4, ≥306 × 103/μL in all adolescent participants; Q1, ≤235; Q2, 236–265; Q3, 266–300; and Q4, ≥301 × 103/μL in adolescent male participants, and Q1, ≤247; Q2, 248–279; Q3, 280–311; and Q4, ≥312 × 103/μL in adolescent female participants. Characteristics of the study participants according to platelet count quartiles were compared using a weighted chi-squared test for categorical variables and a weighted one-way analysis of variance (ANOVA) test for continuous variables. The mean differences and proportion differences between groups were determined using post hoc analysis of weighted ANOVA test and chi-squared test using Bonferroni corrections. The odds ratio (OR) and 95% confidence intervals (CIs) for insulin resistance were calculated using multiple logistic regression analysis after adjusting for confounding factors across platelet count quartiles. All statistical analyses were performed using SPSS statistical software, version 23.0 (SPSS, Inc., Chicago, IL). Statistical significance was set at P < 0.05.
Results
This study included 636 adolescent male and 497 adolescent female participants. The prevalence of overweight and obesity was 14.2% and 5.7% among male participants and 11.3% and 6.6% among female participants, respectively. Table 1 presents the characteristics of the study participants according to their platelet count quartiles. Table 2 gives the characteristics of the study participants according to their gender-specific platelet count quartiles. The mean fasting plasma glucose level and the proportion of an overweight status and obesity were highest in the fourth quartile for male participants. The mean triglyceride level was the highest in the fourth quartile for female participants. The mean values of insulin, HOMA-IR, and leukocyte count increased proportionally with platelet count quartiles for both male and female participants.
Data are presented as mean (standard error) or percentage (standard error). P values were obtained by using weighted one-way ANOVA for continuous variables or weighted chi-squared test for categorical variables. Post hoc analysis of weighted ANOVA test for mean difference between groups: a, Q1 versus Q2; b, Q1 versus Q3, c: Q1 versus Q4; d, Q2 versus Q3; e, Q2 versus Q4, and f, Q3 versus Q4.
ANOVA, analysis of variance; HDL-C, high-density lipoprotein cholesterol; HOMA-IR, homeostatic model assessment of insulin resistance; TG, triglyceride.
Data are presented as mean (standard error) or percentage (standard error). P values were obtained by using weighted one-way ANOVA for continuous variables or weighted chi-squared test for categorical variables. Post hoc analysis of weighted ANOVA test for mean difference between groups: a, Q1 versus Q2; b, Q1 versus Q3, c: Q1 versus Q4; d, Q2 versus Q3; e, Q2 versus Q4, and f, Q3 versus Q4.
Figure 1 illustrates the prevalence of insulin resistance according to platelet count quartiles. The prevalence of insulin resistance increased with increasing platelet count quartiles as follows (Q1, Q2, Q3, and Q4, respectively): 6.8%, 11.6%, 17.2%, and 22.1% for all participants; 5.9%, 9.6%, 19.5%, and 24.2% for male participants; and 8.7%, 9.9%, 14.7%, and 19.9% for female participants.
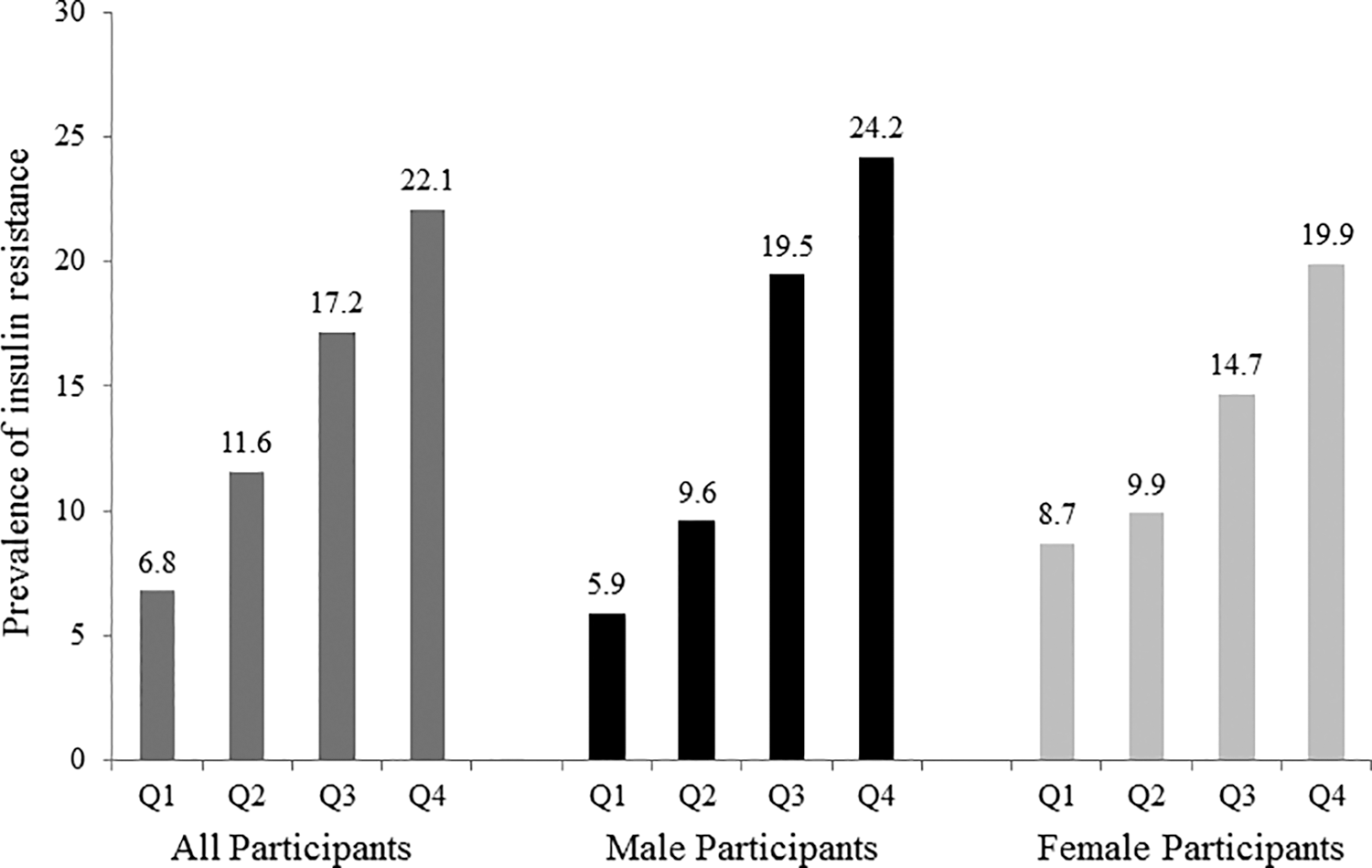
Prevalence of insulin resistance according to platelet count quartiles.
Table 3 gives the ORs (95% CIs) of insulin resistance according to platelet count quartiles, determined using multiple logistic regression analysis. Compared with the ORs for individuals in the lowest platelet count quartile, the ORs for insulin resistance in individuals in the highest quartile were 2.90 (1.39–6.07) for all, 2.98 (1.14–8.31) for male, and 2.14 (0.88–5.32) for female participants, after adjusting for age, gender (for all participants), household income, residential area, family history of diabetes mellitus, and overweight (85th percentile ≤ BMI <95th percentiles for age and gender) or obesity (BMI ≥95th percentile).
Model 1: adjusted for age.
Model 2: adjusted for age, gender (for all participants), household income, residential area, and family history of diabetes mellitus.
Model 3: adjusted for age, gender (for all participants), household income, residential area, family history of diabetes mellitus, and overweight (85th percentile ≤ BMI <95th percentiles for age and gender) or obesity (BMI ≥95th percentile).
BMI, body mass index.
Discussion
In this nationally representative cross-sectional study, we found that platelet count was positively associated with insulin resistance in Korean adolescents after adjusting for potential confounding variables. The positive associations were prominent particularly in boys, but the significant associations were attenuated and disappeared after additionally adjusting for BMI in girls. In a previous study, Taniguchi et al. reported that platelet count was independently associated with insulin resistance in nonobese Japanese patients with type 2 diabetes mellitus. 13 Furthermore, Samocha-Bonet et al. found that overweight, obese, and morbidly obese women in Israel had significantly elevated platelet counts. 17 In addition, Kotani et al. and Fang et al. demonstrated that higher platelet counts are associated with metabolic syndrome, indicating that platelet count may act as a surrogate marker of metabolic syndrome. 14,15 Our findings are consistent with the results of these previous studies, showing an association between platelet count and cardiometabolic risk factors. Moreover, our results suggest that platelet count could be a useful marker for identifying adolescents with insulin resistance. Thus, our results expand on earlier findings regarding the association between platelet count and insulin resistance. We believe that this is the first large population-based study investigating the relationship between platelet count and insulin resistance, as measured by HOMA-IR, in the general pediatric population.
The previously assessed methods for insulin sensitivity include the euglycemic insulin clamp model, oral glucose tolerance test, HOMA-IR, fasting glucose/insulin ratio, and quantitative insulin sensitivity check index. 18 –23 However, the technology may be too invasive or comparatively more difficult to perform. Moreover, serum insulin level is not routinely measured in standard clinical practice. On the contrary, platelet count is inexpensive and easy to interpret, and the measure is ordered routinely in clinical practice.
Several possible mechanisms could underlie the significant association between platelet count and insulin resistance in adolescents. Obesity, a state that is characterized by excessive adipose tissue and typically associated with insulin resistance, 24 usually involves oversecretion of several adipokines, including a megakaryocytic growth factor (thrombopoietin), by omental adipose tissue. 25 Considering that thrombopoietin oversecretion is associated with hyperinsulinemia/insulin resistance as well as platelet activation, the relationship between platelet count and insulin resistance may be mediated by thrombopoietin. 25 –27
Another important factor to consider is chronic low-grade inflammation. Insulin resistance is increasingly being recognized in subclinical inflammatory states. 28,29 Increased levels of inflammatory markers such as leukocytes, interleukin 6, and C-reactive protein are believed to be independent predictors of cardiovascular disease and insulin resistance. 30 –32 In addition, growing evidence suggests that platelet count is also an inflammatory marker. 33 Indeed, in this study, leukocyte count (a marker of inflammation) increased proportionally with an increase in platelet count quartiles. This finding suggests that the association between platelet count and insulin resistance may be explained by low-grade chronic inflammation.
This study has several limitations that should be considered when interpreting the results. First, only one platelet count measurement was included in the analysis; thus, it was not possible to determine whether an acute and brief episode of hemostasis affected the findings reported herein. Second, because this was a cross-sectional study, we were not able to establish a causal relationship between platelet count and insulin resistance, which should be investigated in future prospective studies. Third, we defined insulin resistance as a HOMA-IR value greater than the 85th percentile. As mentioned previously, HOMA-IR is a generally accepted method for quantifying insulin resistance in epidemiological studies. However, there are no definitive HOMA-IR cutoff values for identifying insulin resistance. Finally, we did not take into consideration the physiological effects of puberty on insulin resistance. Studies have indicated that transient insulin resistance occurs during puberty. 34 Unfortunately, because information on the pubertal stages of participants was not included in the KNHANES data set, the pubertal stage of the participants was not directly considered in the analysis. To minimize this limitation, however, we analyzed the data subdivided by gender, and included age as a confounding variable in the multiple logistic regression analysis. Further research is required to elucidate the relationship between platelet count and insulin resistance according to pubertal stage, with a comparison between adolescent female and male participants. Despite these potential limitations, a nationally representative sample of Korean adolescents was used in this study, which supports the general applicability of the present findings. A large sample of healthy participants from both genders allows for an appropriate empirical study on the relationship between platelet count and insulin resistance and strengthens the validity of the findings.
In conclusion, a higher platelet count was revealed to be positively associated with an increased risk of insulin resistance in Korean adolescents. The current findings contribute to our understanding of the relationship between platelet count and insulin resistance in adolescents. The findings of this study suggest that the platelet count, a simple inexpensive measure included in complete blood count testing in routine clinical practice, could be a useful measure for identifying adolescents with insulin resistance. Moreover, our findings indicate that physicians should consider the possibility of insulin resistance in adolescents with higher platelet counts.
Footnotes
Author Disclosure Statement
No competing financial interests exist.