
Abstract
Nonalcoholic fatty liver disease (NAFLD) encompasses a spectrum of disease, including hepatic steatosis, inflammation, and fibrosis. NAFLD carries the risk of progression to cirrhosis with its associated complications and hepatocellular carcinoma. It is now the most common liver disease in the Western world and its prevalence is increasing. While the association between NAFLD and type 2 diabetes has been well documented, there is significantly less understanding of the pathophysiology and progression of NAFLD in patients with other endocrine disorders affecting metabolism in various ways. Some of the more common endocrine disorders such as polycystic ovarian syndrome, growth hormone deficiency, hypothyroidism, and hypogonadism are known in clinical practice to be associated with NAFLD. Medications that alter the endocrine system such as tamoxifen and adrenal steroids have also been attributed to significant NAFLD. The key to management of NAFLD at this time are dietary changes and exercise to achieve weight loss. Unfortunately, a large proportion of the patients with these endocrine disorders are unable to achieve either. This review aims to examine and summarize the current published literature that have evaluated the association between NAFLD and the above endocrine disorders and potential therapeutic interventions in each case.
Introduction
T
Although the exact pathogenesis of NAFLD is complex, many have demonstrated the role of fatty acid metabolism and insulin resistance (IR) in the development of the disease. As a result, the relationship between Type 2 diabetes mellitus (T2DM) and NAFLD has been well documented. 3 NAFLD is strongly associated with other nondiabetic endocrine disorders as well. Unfortunately, not only does our understanding remains limited in regard to their pathophysiology but also the interest remains low (Fig. 1). In this article we delve into the current understanding of NAFLD and its relationship to nondiabetic endocrinopathies such as polycystic ovarian syndrome (PCOS), hypogonadism, growth hormone (GH) deficiency, thyroid dysfunction, and medications that affect the endocrine pathways such as adrenal steroids and tamoxifen.
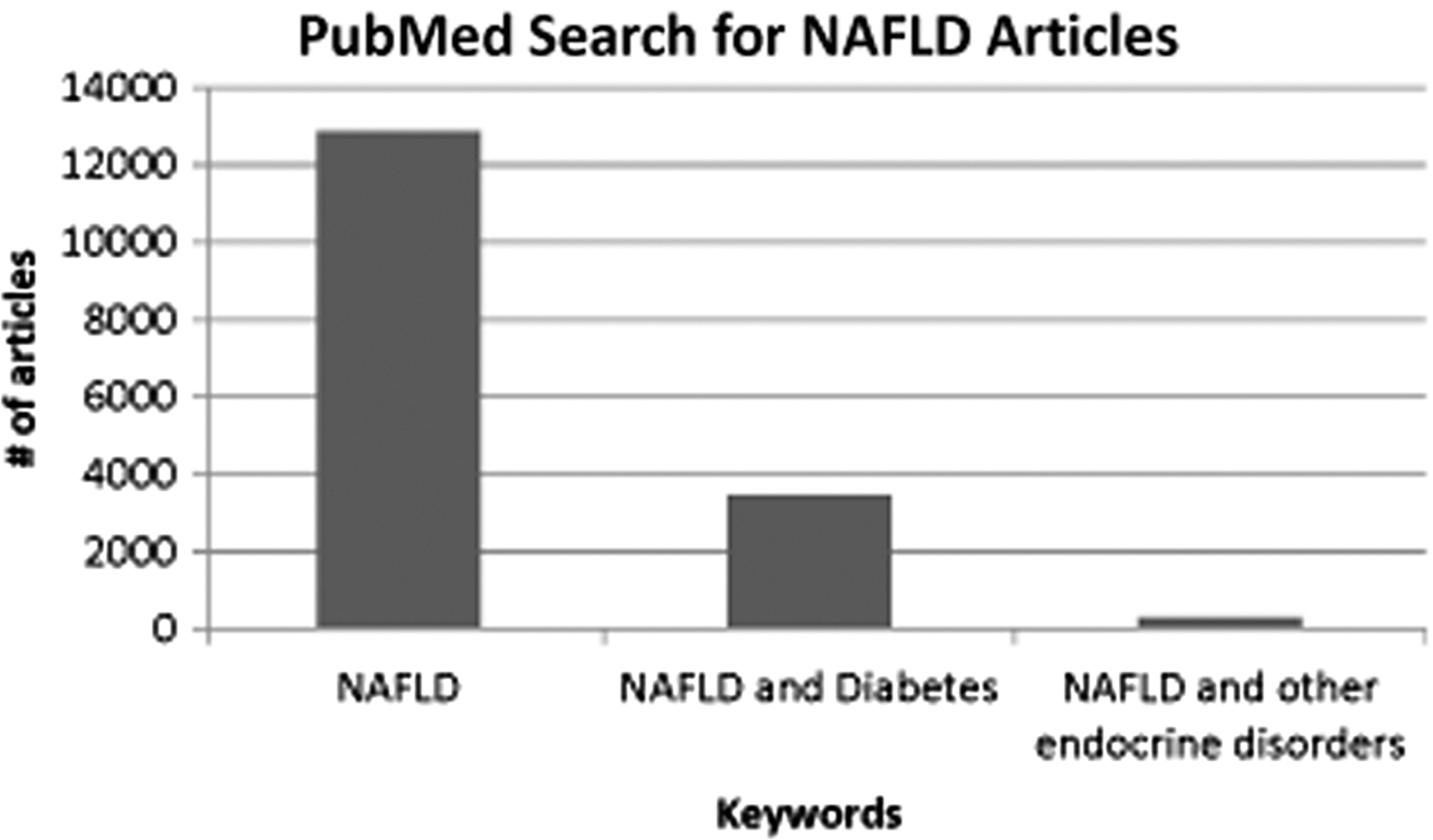
PubMed Search for NAFLD Articles. A PubMed search was conducted with the keywords “NAFLD,” “diabetes,” and “endocrine” with the corresponding number of search results. While the relationship between NAFLD and diabetes has been well researched, there have been much fewer articles examining NAFLD and other endocrine disorders. NAFLD, nonalcoholic fatty liver disease.
Pathogenesis of NAFLD
The pathogenesis of NAFLD is intimately related to fatty acid metabolism in the liver through a proposed “three-hit hypothesis”. 4
The first hit involves the accumulation of free fatty acids (FFAs) in the liver either through an increase in synthesis or delivery or a decrease in export or oxidation. While increased dietary intake of lipids can contribute to increased FFA accumulation in the liver, insulin can suppress lipolysis in adipose tissue, which decreases the amount of efflux of FFA to the liver. Thus, IR can impair this suppressive effect and lead to increased deposition of FFA in the liver. The second hit postulates that the increased accumulation of FFAs in the liver causes oxidative stress and upregulation of inflammatory cytokines that leads to inflammation and fibrosis and eventually, cell death. The final hit involves how ongoing oxidative stress and inflammation decreases hepatocyte proliferation and maturation, which leads to further development of fibrosis. There is also evidence that endoplasmic reticulum stress and other related signaling networks, in addition to gut endotoxins, may play a central role in the pathogenesis of NAFLD. 5
Diagnosis of NAFLD
While central obesity or other diagnostic criteria for metabolic syndrome may help identify patients at risk for development of NAFLD, there are no physical exam findings specific for NAFLD. Unfortunately, signs of cirrhosis such as scleral icterus, jaundice, spider angiomata, palmar erythema, caput medusa, or ascites likely indicate an already advanced stage of disease. Furthermore, the majority of patients with NAFLD are asymptomatic or have nonspecific symptoms. Thus, the initial diagnosis is often an incidental finding on imaging or an abnormal Alanine Aminotransferase (ALT) level when the patient is being evaluated for an unrelated condition. This is further complicated by studies that have shown that up to 30%–60% of patients with biopsy-confirmed NASH have a normal ALT level. 2
Ultrasound has emerged as an inexpensive and low-risk diagnostic tool in identifying hepatic steatosis. Some studies have reported 100% sensitivity when there is greater than 33% steatosis. 6,7 However, some characteristics of more severe NASH, such as fibrosis, may be indistinguishable from simple steatosis on ultrasound.
Given the overwhelming prevalence of NAFLD, liver biopsy is likely not a cost-effective way to diagnosis the disease in most patients. But it remains the gold standard for diagnosis and staging of NAFLD. Data from the NASH Clinical Research Network helped refine a staging system for biopsy grading and staging of NAFLD-related steatosis, inflammation, and fibrosis. 8 The development of the NAFLD fibrosis score may help further identify patients who should receive a liver biopsy for confirmation of diagnosis. The score considers a patient's age, body mass index (BMI), ALT, aspartate aminotransferase, platelets, albumin, and whether they have impaired fasting glucose or diabetes. Values less than −1.455 can predict the absence of significant fibrosis (stage 0–2) with an 88% certainty, while values >0.676 are able to predict the presence of significant fibrosis (stage 3–4) with an 82% certainty. 9 Patients that fall between these two values are indeterminate and may need liver biopsy to confirm the degree of fibrosis.
Endocrinopathies associated with NAFLD
NAFLD is commonly encountered in clinical settings in patients with
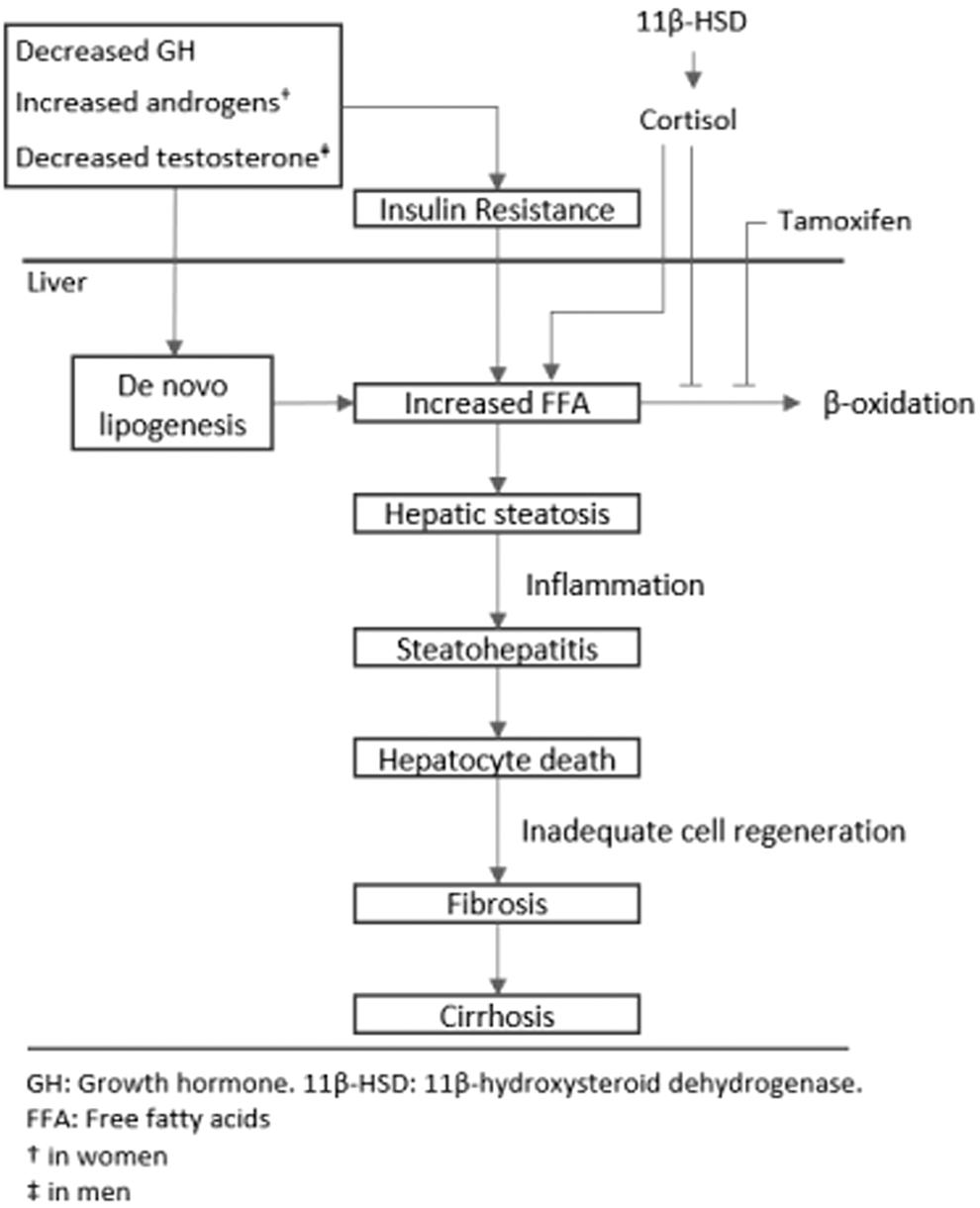
Endocrine Mechanisms of NAFLD. IR leads to increased FFA uptake into the liver, which is the major mechanism by which diabetes is associated with NAFLD. Other endocrine abnormalities such as decreased GH, increased androgens (in women), and decreased testosterone (in men) also can lead to hepatic steatosis via a mechanism that is independent of the effects of IR alone. Medications such as cortisol and tamoxifen contribute to hepatic steatosis by inhibiting the metabolism of fatty acids via β-oxidation. FFA, free fatty acids; GH, growth hormone; IR, insulin resistance.
Polycystic ovarian syndrome
PCOS is a syndrome that is classically characterized by hyperandrogenism and IR. Given the intimate relationship between IR and NAFLD, it is natural to assume a correlation between NAFLD and PCOS. This has been reviewed by many studies that have documented the increased prevalence of NAFLD in patients with PCOS. 10
One Brazilian case–control study of 90 obese women showed that the prevalence of NAFLD is higher in obese patients with PCOS compared with their age-matched, obese controls, 11 which suggests that obesity and IR are not the sole risk factors for NAFLD in PCOS patients. Elevated free and total testosterone levels were also positively associated with elevated ALT and presence of NAFLD, suggesting a role of androgens in the pathogenesis of the disease. 12 Notably, PCOS patients with hyperandrogenism have a higher prevalence of NAFLD compared to those without. 13 Another study that looked at the effect of metformin in NAFLD patients with PCOS found that PCOS patients with ultrasound-confirmed diagnosis of NAFLD had significantly higher free-androgen index values compared to PCOS patients without evidence of NAFLD. 14 These data suggest that there is a distinct mechanism (aside from just IR) by which hyperandrogenism contributes to NAFLD.
Diagnosis of NAFLD in these patients is essential to enable linkage to care. Plasma ALT and noninvasive liver imaging such as ultrasound should be considered in PCOS patients with hyperandrogenism.
Several diabetes drugs, such as thiazolidinediones and metformin, have been used to improve insulin sensitivity and decrease androgen levels in patients with PCOS. 15 Some trials have shown that thiazolidinediones can help normalize ALT levels and improve histological inflammation and fibrosis. 16 These data remain less convincing for metformin as several studies have shown that, despite an improvement in insulin sensitivity, there is no histological improvement of disease after treatment. 17
The PIVENs trial demonstrated the effectiveness of vitamin E in reducing ALT levels, hepatic steatosis, and lobular inflammation in patients with NASH although this was not focused specifically on patients with PCOS. 18 Interestingly, a combination of omega-3 fatty acids and vitamin E has been shown to improve insulin sensitivity and decrease free and total testosterone levels in patients with PCOS. 19 Overall, these findings may suggest an important role of vitamin E in the overall treatment of NAFLD in patients with PCOS and should be a consideration for therapy.
Male hypogonadism
In contrast to women with PCOS, androgen deficiency in men is associated with metabolic syndrome and fatty liver. Male hypogonadism, defined as a low testosterone level along with clinical symptoms of decreased libido, erectile dysfunction, and decreased lean body mass, has also been associated with NAFLD in the literature. This correlation was demonstrated in a preclinical study in which mice with liver-specific knockout of the androgen receptor developed a greater degree of hepatic steatosis in comparison with obese controls. 20
A retrospective study of 1912 men from Central Europe showed that hepatic steatosis correlates independently with low serum testosterone levels after adjusting for age, BMI, smoking, DM, and visceral adipose tissue. 21 In another retrospective cross-sectional study of 495 Korean men, those with the lowest quintile of testosterone concentrations had an odds ratio of 4.52 for presence of NAFLD, after accounting for confounding variables including age, smoking, DM, exercise, cholesterol, and BMI. 22 This then begs the question of whether testosterone replacement could improve hepatic steatosis.
An in vivo study in castrated rats who were fed a high fat diet showed that testosterone replacement decreased body fat percentage and led to less severe microvesicular hepatic steatosis compared to those not receiving testosterone. 23 In this study, the serum glucose and insulin levels were not increased in either group, suggesting an insulin independent effect. The use of testosterone treatment to decrease hepatic steatosis has also been evaluated in humans. In a randomized control trial of 67 patients with obstructive sleep apnea, testosterone replacement therapy improved insulin sensitivity and reduced hepatic steatosis, without a reduction in BMI or weight. 24 Finally, testosterone has been shown in various studies to play a critical role in insulin sensitivity, 25 a mechanism that independently correlates with NAFLD. In a recent single center double blind trial, testosterone replacement treatment in men with T2DM and hypogonadotrophic hypogonadism was shown to increase insulin sensitivity, lean mass, and decrease subcutaneous fat. 26
Testosterone therapy is not without risks, which include increased prostate volume and prostate-specific antigen level, worsening sleep apnea, erythrocytosis and venous thromboembolism. Patients on testosterone therapy are routinely monitored, and therapy is discontinued if they experience adverse effects.
GH deficiency
Hypopituitarism is a disease that is accompanied by a host of metabolic changes that can include central obesity, hyperglycemia, IR, and NAFLD. Most of these changes are thought to be mediated by GH deficiency. While the exact mechanism remains unknown, adults with GH deficiency have increased visceral adiposity and abnormal lipid profiles. 27 It has been shown that adult patients with anterior hypopituitary insufficiency and associated GH deficiency have a higher incidence of fatty infiltration of the liver when compared to patients with anterior hypopituitary insufficiency without GH deficiency. 28
Furthermore, a Korean study found that the severity of NAFLD on ultrasound was negatively correlated with GH levels after adjusting for BMI. 29 One case series followed 21 patients who developed NAFLD after being diagnosed with pituitary/hypothalamic disease. The diagnosis of NAFLD was made either by liver biopsy or by evidence of fatty infiltration of the liver on imaging in conjunction with elevated liver enzymes. On average, the diagnosis of NAFLD was made 6.4 years after the diagnosis of pituitary/hypothalamic disease, showing a rather rapid development. 30 Of those 21 patients, 3 died from complications related directly to their liver disease.
Given the proposed role of GH deficiency in mediating NAFLD, there have been a few studies that observed the effect of GH replacement therapy (GHRT) on liver function. One Japanese study of 69 patients analyzed the presence of NAFLD by ultrasound and liver biopsy. They showed that GHRT not only improved liver enzyme levels, but also improved histologic markers of steatosis and fibrosis in those with biopsy-confirmed NASH. 31 The one caveat observed by another Japanese retrospective observational study was that body weight gain while on GHRT can attenuate some of these beneficial effects. 32
Another British study of 28 patients with GH deficiency and 24 controls found a reduction in abdominal and visceral fat but no difference in hepatic fat or transaminase levels. 33 Notably, this study did not perform liver biopsies, so they were not able to differentiate between simple steatosis and more advanced disease such as NASH. Thus, there may be a role for GHRT in those with GH deficiency to help ameliorate the progression of NAFLD, if patients are able to avoid gaining weight.
Hypothyroidism
Thyroid hormones are important regulators of the body's metabolic function. Hypothyroidism is proposed to lead to NAFLD through a combination of intra and extrahepatic mechanisms. In mouse models, reduced thyroid hormone levels decrease suppression of adipose tissue lipolysis due to decreased insulin secretion and increased IR in the tissue. 34 This leads to increased hepatic uptake of fatty acids, which induces hepatic IR and, subsequently de novo lipogenesis. Notably, this effect was only seen in mice with mild hypothyroidism. Severe hypothyroid mice had such profound inhibition of adipose tissue lipolysis, which led to decreased delivery of fatty acids to the liver.
There have been multiple cohort, cross-sectional, and case–control studies that have investigated the relationship between hypothyroidism and NAFLD. Unfortunately, the results are conflicting.
One recent meta-analysis involving a total of 14 observational studies (9 cross-sectional, 4 case–control, and 1 cohort study), which included around 7000 NAFLD patients and 30,000 controls showed that NAFLD was not associated with subclinical, overt, or overall hypothyroidism. 35 The same authors also conducted separate meta-analyses for assessing the association between NAFLD and FT3, FT4, and thyroid stimulating hormone (TSH) levels and found no significant difference in NAFLD patients compared to non-NAFLD controls.
On the other hand, another recent meta-analysis that analyzed 13 studies, which included around 42,000 participants, found high correlation between hypothyroidism and NAFLD. 36 Further subgroup analysis found that both overt and subclinical hypothyroidism were significantly correlated with NAFLD. Both meta-analyses used pooled odds ratios with 95% confidence intervals to evaluate the association.
Despite the unclear association between NAFLD and hypothyroidism, one Chinese study conducted a retrospective post hoc analysis of a randomized control trial looking at the effects of levothyroxine replacement therapy on NAFLD in patients with subclinical hypothyroidism. 37 They found that treatment with levothyroxine reduced the prevalence of NAFLD in significant subclinical hypothyroidism patients (TSH ≥10 mIU/L) from 48.5% to 24.2%. However, in mild subclinical hypothyroidism patients (TSH of 4.2–10 mIU/L) there was no difference after treatment with levothyroxine. This study was limited by the fact that NAFLD was diagnosed via ultrasound as opposed to liver biopsy so it is unclear whether levothyroxine can provide any significant histological changes in the disease progression. Additionally, the ALT levels in a majority of patients were already normal, so the further decrease upon treatment with levothyroxine may not be clinically significant.
At this time it is difficult to say if there is any utility in TSH testing in NAFLD patients with no clinical signs of thyroid dysfunction.
Endocrine-related medications
Adrenal steroids
Excess glucocorticoids can lead to IR and many manifestations of metabolic syndrome. It appears that local production of glucocorticoids in the visceral adipose tissue, as well as overall glucocorticoid excess, can lead to fatty liver. Glucocorticoids are produced by adrenal glands in response to adrenocorticotropic hormone stimulation. They are metabolized by 11 beta-hydroxysteroid dehydrogenases (11β-HSD) and A-ring reductases, including 5-alpha and 5-beta reductase in the extra-adrenal tissues. 11β-HSD type 1 regenerates the active cortisol from the inactive cortisone in the brain, liver, and adipose tissue. 11β-HSD type 2 converts the active glucocorticoid cortisol to its inactive form, cortisone, at sites of aldosterone action such as the kidneys.
A murine study showed that deletion of 5-alpha reductase type 1 inhibits conversion of corticosteroids to androgens, causing hepatic accumulation of glucocorticoids and increases the risk of hepatic steatosis. This persisted following gonadectomy, suggesting an androgen-independent role for glucocorticoids. 38 Another study showed that transgenic mice overexpressing 11β-HSD1 in adipose tissue develop hepatic steatosis and metabolic syndrome. 39
In contrast, 11β-HSD1 knock out mice were protected from hepatic steatosis. 40 Another in vivo study confirmed that genetic knockout of 11B-HSD type 1 in mice consuming a western type diet had decreased hepatic steatosis due to decreased synthesis and secretion of triglycerides and increased fatty acid oxidation. 41 Liver-specific disruption of the glucocorticoid receptor also improved hepatic steatosis by specifically triggering the hydrolysis of triglyceride stores through fatty acid oxidation pathway. 42
Studies in humans also support the role of local or general excess of cortisol in the etiology of fatty liver.
A study that determined the expression of 11β-HSD 1 in 49 morbidly obese patients undergoing bariatric surgery demonstrated that overexpression of this enzyme in the visceral adipose tissue was associated with the presence of NAFLD. 43 The enzymes metabolizing glucocorticoids are abundant in the liver and their expression and activity may vary depending on the stage of the fatty liver process.
Ahmed et al. demonstrated that during the hepatic steatosis phase, metabolism and urinary clearance of cortisol increased while hepatic regeneration decreased, possibly pointing to a protective mechanism to limit hepatic cortisol exposure. In the early phases of NAFLD, 5-alpha reductase activity is increased, leading to increased cortisol clearance, while 11β-HSD type 1 is decreased, which is thought to be part of a physiologic protective response. 44 Interestingly, only 20% of patients with Cushing's disease (or nonfunctioning pituitary adenoma) who are on daily hydrocortisone have hepatic steatosis. This has been theorized to be due to inhibition of low grade chronic inflammation by cortisol, mediated by interleukin 6. 45 In the later stages of NAFLD, 5-alpha reductase activity is decreased, leading to decreased cortisol clearance, while 11β-HSD type 1 is increased.
Clinical trials have shown selective 11β-HSD type 1 is inhibitors improved glycemic control, lipid profile, and led to weight loss in patients with type 2 diabetes. 46,47 Their therapeutic utility is currently being investigated in the context of hepatic steatosis.
Tamoxifen
Tamoxifen has long been used as an adjuvant hormonal therapy in treatment of patients with estrogen receptor (ER)-positive breast cancer. While generally well-tolerated, one of the most common side effects of tamoxifen is development of NAFLD. The exact pathogenesis of tamoxifen induced NAFLD is unclear, but estrogen is known to help modulate fatty acid oxidation. Thus, tamoxifen, which binds to the ER, may inhibit fatty acid oxidation and lead to hepatic steatosis. 48
The possibility of tamoxifen-induced NAFLD may have been reported as early as 1995 when a woman with breast cancer being treated with tamoxifen subsequently developed elevated liver enzymes and had evidence of hepatic fatty infiltration on US. 49 Liver biopsy confirmed macrovesicular fat and portal inflammation with fibrosis and a diagnosis of NASH was made in the absence of alcohol use. Once tamoxifen was discontinued in this patient, liver enzyme levels normalized in 4 months.
Since that case report, studies have shown as high as 40% of patients treated with tamoxifen may develop evidence of NAFLD. When compared to controls, patients treated with tamoxifen show higher rates of development of NAFLD as well as worsening of the degree of severity of NAFLD. 48 One large prospective, randomized, double-blind, placebo-controlled trial that analyzed the effect of tamoxifen in 5408 women with breast cancer suggested that the risk of tamoxifen-induced NAFLD was only seen in overweight women. 50
Several studies have looked at therapies that may help attenuate some of these effects. One study showed that Uridine, a pyrimide nucleoside, helped prevent tamoxifen-induced liver lipid droplet accumulation in mice when co-administered. 51 UPAse1TG mice, which have decreased liver and circulating uridine concentrations, showed evidence of microvesicular steatosis even before being treated with tamoxifen. Upon treatment, the liver lipid content was even further increased. Another study looked at anordrin, which is marketed as an antifertility medicine in China. Anordrin was shown to reduce baseline hepatic triglyceride levels when compared to controls and help reverse some of the tamoxifen-induced NAFLD. 52
Conclusion
NAFLD is one of the most common causes of liver disease in the world, and its prevalence is likely to continue to increase. It is important that physicians recognize its effects not only in regard to the liver, but also its association with specific endocrinopathies that can create diagnostic and management challenges unique to its disease state. Understanding the pathophysiology of NAFLD in these distinct endocrinopathies is essential in not only managing these patient cohorts but also in developing novel therapies for the general NAFLD population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.