
Abstract
Background:
The plasma concentration ratio of triglyceride (TG)/high-density lipoprotein cholesterol (HDL-C) is a simple way to estimate insulin resistance. We aimed to evaluate the TG/HDL-C ratio as a simple clinical way to identify apparently healthy individuals with insulin resistance and enhanced risk of future cardiovascular disease (CVD).
Methods:
One thousand seven hundred twenty men, aged 50 years, free from diabetes and CVD when evaluated at baseline in 1970–1974 were followed for 40 years regarding incident CVD (myocardial infarction and/or ischemic stroke, n = 576).
Results:
Participants with a high TG/HDL-C ratio (highest quartile >1.8) at baseline were more insulin resistant, with a significantly more adverse cardiometabolic risk profile (P < 0.001) at baseline, compared with those with a lower ratio. This group also showed an increased risk of CVD [hazard ratio, HR 1.47 (95% confidence interval 1.26–1.93) P < 0.001]. Fourteen percent of subjects with metabolic syndrome, in whom insulin resistance is increased, were also at enhanced CVD risk [HR 1.75 (1.42–2.16) P < 0.001].
Conclusions:
Twenty-five percent of apparently healthy 50-year-old men with the highest TG/HDL-C plasma concentration ratio had a significantly more adverse cardiometabolic profile at baseline, and developed more CVD over the next 40 years, compared with those not meeting this cut point. Determining the TG/HDL-C ratio in middle-aged men provided a simple and potentially clinically useful way to identify increased risk of developing CVD in persons free of diabetes or manifest CVD.
Introduction
P
An alternative way to identify individuals within an apparently healthy population who are sufficiently insulin resistant and at increased risk of CVD is to use commonly measured metabolic abnormalities associated with insulin resistance. The metabolic syndrome (MetS) diagnostic criteria are an example of this approach. 9 The independent relationship between insulin resistance and both plasma triglyceride (TG) and high-density lipoprotein cholesterol (HDL-C) concentrations led to the suggestion that the plasma concentration ratio of TG/HDL-C might accomplish the same goal 10 –12 while being simpler to calculate than the MetS. Sex-specific TG/HDL-C cut points have been shown to identify individuals at high risk of incident CVD. 13,14 To further evaluate if the ratio of TG/HDL-C, being easy to obtain in both primary and specialized care, is a useful tool to identify high-risk individuals, the current study was initiated to analyze data obtained as part of the Uppsala Longitudinal Study of Adult Men (ULSAM) 15 with several goals in mind: (1) evaluation of the ability of the TG/HDL-C ratio to identify increased cardiometabolic and overall CVD risk in an apparently healthy middle-aged population; (2) comparison of the ability of the TG/HDL-C ratio cut point that defined high risk and incident CVD in this population with that used for the same purpose in previous studies; (3) determination of the ability of a high-risk TG/HDL-C ratio to predict risk of incident myocardial infarction (MI) vs. stroke; and (4) use a diagnosis of MetS to identify a high-risk population to serve as a benchmark with which to compare estimates of cardiometabolic risk and incident CVD with those generated using the TG/HDL-C ratio. MetS has been shown to add prognostic value above and beyond established risk factors in this cohort. 15
Methods
Study sample
In 1970–1974, all men born during the period 1920–1924 and residing in the county of Uppsala were invited at random to a health survey (at age 50) aimed at identifying risk factors for CVD; 82% of the invited men participated (n = 2322). The design and selection criteria for the cohort have been described previously. 15 Informed written consent was obtained and the Uppsala University Ethics Committee approved the study.
Baseline examinations
The general procedures followed have been described in detail previously. 15 Supine systolic and diastolic blood pressure levels were measured twice in the right arm after a 10-min rest, and means were calculated. Blood samples for fasting concentrations were drawn in the morning after an overnight fast. Cholesterol and TG concentrations in serum and HDL-C were assayed by enzymatic techniques. Low-density lipoprotein cholesterol concentration was calculated by Friedewald's formula. 16 Fasting blood glucose was determined by an oxidase method, and serum insulin was measured with the Phadebas Insulin test (Pharmacia AB, Sweden), based upon a radioimmuno-absorbent technique. Homeostasis model assessment of insulin resistance (HOMA-IR) was calculated 17 using the formula ([insulin (μU/mL) × glucose (mg/100 mL)/18]/22.5). Insulin was only measured in a random sample of 1425 subjects due to lack of serum. The concentrations of intact and 32–33 split proinsulin were analyzed using the two-site immunometric assay technique 18 in plasma samples that had been stored frozen (−70°C) since baseline.
Diabetes at baseline was defined according to the WHO 2006 definition (fasting blood glucose ≥6.1 mM or the use of antidiabetic medication). Volunteers meeting these criteria were excluded from further analysis, as were individuals who had TG concentrations >5.6 mM or HDL-C concentrations >2.6 mmol or prevalent CVD at baseline. Thus, the sample at risk (with determinations of TG and HDL-C) at baseline was 1720.
NCEP/ATP-III criteria with a slight modification were used to determine the presence of MetS, in which three of the following five diagnostic criteria must be met: blood pressure >130/85 mmHg or antihypertensive treatment, fasting blood glucose >5.6 mM, serum TGs >1.7 mM, HDL-C <1.0 mM, 9 and increased waist circumference. As waist circumference was only measured in a minority of men at age 50 (n = 480), we performed a regression analysis showing that a waist circumference of 102 cm corresponds to a body mass index (BMI) of 29.4 kg/m2 in middle-aged men, a value then used in the present study as the cutoff for obesity criteria in the MetS definition. A previous analysis has shown this substitution to only induce <1% misclassification in men. 15
End point definitions
Date and cause of death were obtained from the Swedish Cause of Death Registry. Date and cause of hospitalization were obtained from the Swedish Hospital Discharge Registry. We evaluated acute myocardial infarction (ICD-8 code 410, ICD-9 code 310, or ICD-10 code I20, not including unstable angina pectoris) and ischemic stroke (ICD-8 codes 431, 433–436, ICD-9 codes 431, 433–436, and ICD-10 codes I63–I66, not including TIA). Both fatal and nonfatal events were included in those end points. The combined end point used in this study (CVD) consisted of myocardial infarction and/or stroke.
Combining data from the Swedish Cause of Death Registry and the Swedish Hospital Discharge Registry is an efficient validated alternative to revised hospital discharge notes and death certificates for both coronary heart disease and stroke. 19,20 Censor date for the registers was December 31, 2013.
At age 70, the cohort was reinvestigated, and in 1099 of nondiabetics without CVD, we have measurements on both the TG/HDL-C ratio and the euglycemic clamp method. The euglycemic clamp method was performed according to DeFronzo et al., 21 with a slight modification: the rate of infused insulin was 56 mU/min/BSA instead of 40 mU/min/BSA. The M-value was calculated as the amount of glucose taken up during the last 60 min of the 120-min-long clamp procedure.
Statistical analyses
For cross-sectional analyses at baseline relating a high TG/HDL-C ratio (or MetS) to cardiometabolic risk factors, one-way ANOVA or chi-square tests were used. In those analyses, fasting blood glucose, serum TG, plasma insulin, and HOMA-IR were log-transformed to achieve a normal distribution.
Cox proportional hazard models were used to assess the risk of a high TG/HDL-C ratio (or MetS) on CVD (primary analysis) or myocardial infarction or stroke (secondary analyses). We used the upper quartile of the TG/HDL-C ratio (1.8) as the cutoff value as well as a previously suggested cutoff of 1.5. 14 The proportional hazard assumption was evaluated by visual inspection of graphs. No adjustments were performed in the models since age and sex are the same in all individuals, and the aim was to evaluate the clinical usefulness of a high TG/HDL-C ratio (not the added value compared with other risk factors).
The risk of future CVD from age 70 was also investigated in those with a TG/HDL-C ratio >1.8 (or 1.5) using Cox proportional hazard models.
The relationship between the TG/HDL-C ratio and M-value at clamp at the 70-year investigation was evaluated by a regression model using cubic restricted splines with three knots (10th, 50th, and 90th percentiles) for the TG/HDL-C ratio. We also fitted a model examining the effect of interaction of the TG/HDL-C ratio and BMI on the M-value at clamp.
STATA 14 (Stata, Inc., College Station, TX) was used for calculations, and P < 0.05 was regarded as significant.
Results
Table 1 compares degree of insulin resistance (HOMA-IR) and cardiometabolic risk factor profiles of the high-risk group, as identified by each of the three criteria. First, it can be seen that the magnitude of insulin resistance was significantly increased in all three high-risk groups. Second, every cardiometabolic risk factor measured was significantly more adverse in those identified as high risk, irrespective of the criteria used to classify them. However, the number of persons identified as at high risk varied dramatically as a function of the criteria used to identify them, ranging from a low of 14% (MetS) and 25% (TG/HDL-C ≥1.8) to fairly high of 37% (TG/HDL-C ≥1.5). Third, although the number of apparently healthy persons identified as high risk varied with the TG/HDL-C cut point used, inspection of actual values of individual cardiometabolic variables seems surprisingly comparable whether a TG/HDL-C ratio of ≥1.5 or ≥1.8 was used for purposes of classification. Finally, although the fewest number of apparently healthy persons identified as being at high risk met MetS criteria, their individual cardiometabolic risk factors appeared somewhat accentuated compared with high-risk groups identified with the two TG/HDL-C ratio cutoff levels.
BMI, body mass index; CVD, cardiovascular disease; ,DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; HOMA-IR, homeostasis model assessment of insulin resistance; LDL-C, low-density lipoprotein cholesterol; MetS, metabolic syndrome; SBP, systolic blood pressure; TG, triglyceride.
Table 2 compares hazard ratios (HRs) for total CVD (MI and/or stroke), as well as for MI and stroke separately, in the high-risk groups as a function of the criteria used for classification. The HRs for total CVD were all significantly increased (P < 0.001) in the high-risk groups, irrespective of how they were identified. HRs for MI were significantly increased (P < 0.001) in apparently healthy persons classified as at high risk with all three criteria, while HRs for ischemic stroke were reduced in all three high-risk groups and only remained statistically significant in persons with MetS (P = 0.008). Cumulative hazard estimates comparing incident CVD in high-risk groups with the remainder of the population are illustrated in Fig. 1 and essentially convey the same message.
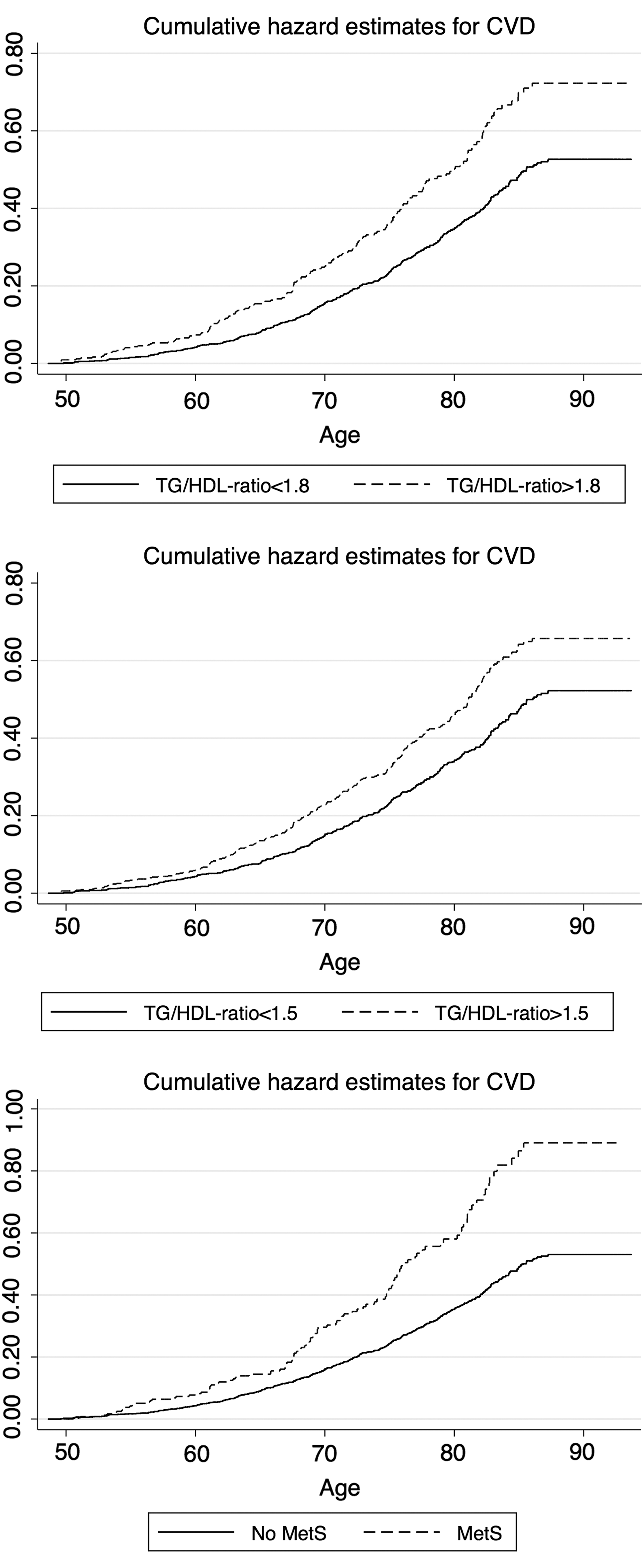
Cumulative hazard estimates for incident CVD (myocardial infarction or ischemic stroke) in subjects with elevated TG/HDL ratio (cutoff 1.8 shown in upper panel, cutoff 1.5 shown in middle panel) or in those with MetS (lower panel). CVD, cardiovascular disease; HDL, high-density lipoprotein; MetS, metabolic syndrome; TG, triglyceride.
Total sample n = 1728.
CI, confidence interval; HR, hazard ratio.
At age 70, the mean TG/HDL-C ratio was 1.26 (SD 0.94) and the mean M-value at clamp was 5.17 mg/kg/min (SD 2.04). The relationship between the TG/HDL-C ratio and M-value at clamp was highly significant (P < 0.0001) and nonlinear (P < 0.0001) with the steepest slope for TG/HDL-C ratio values lower than 1.5 (Fig. 2). The relationship between the M-value at clamp and TG/HDL-C ratio was still significant (P < 0.0001) after adding BMI to the model. The interaction between the TG/HDL-C ratio and BMI in this respect is shown in the contour plot in Fig. 3.
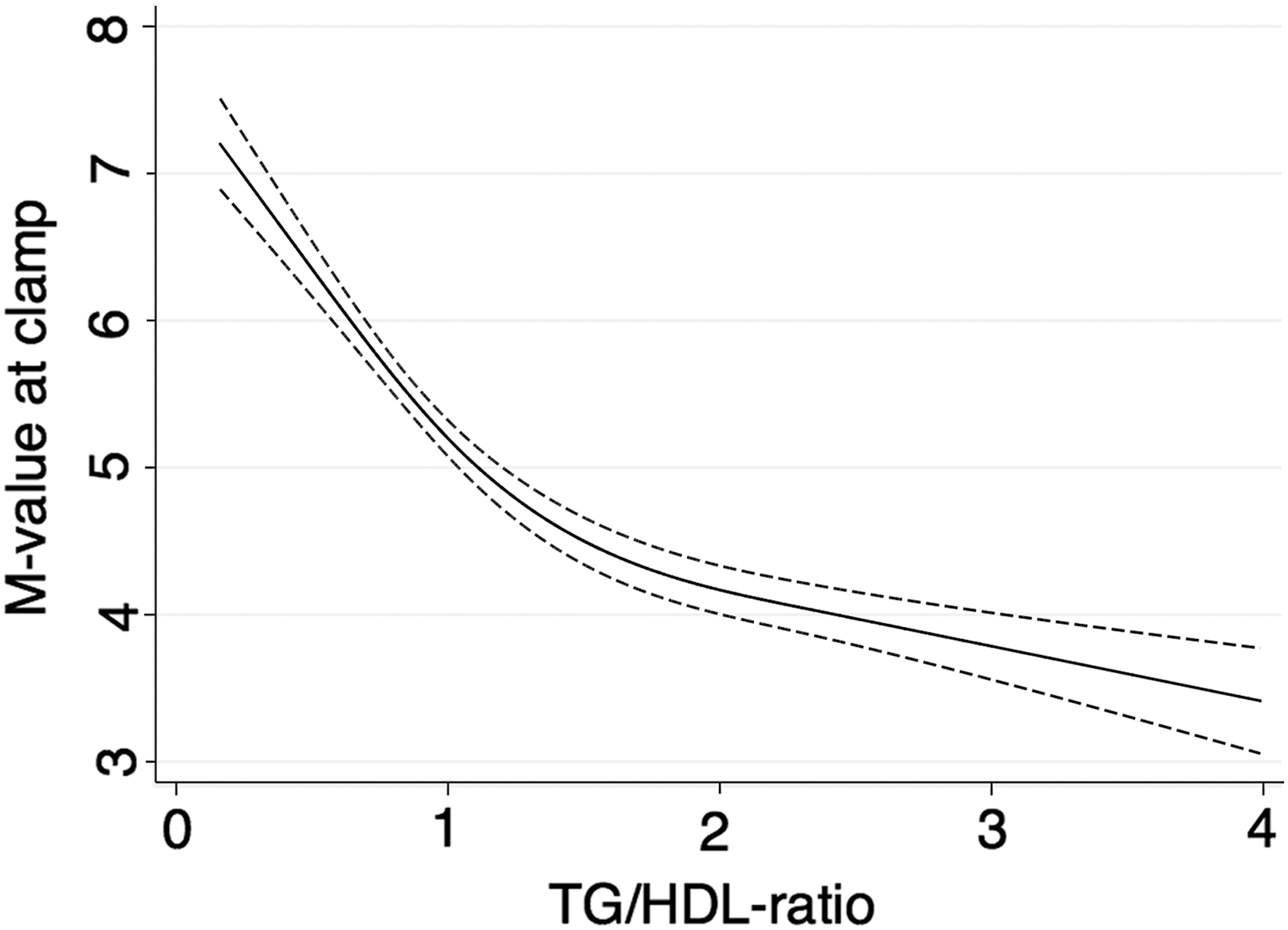
Relationship between the TG/HDL-C ratio and the M-value at clamp based on data from reinvestigation at age 70. A cubit restricted spline function with three knots was used for the TG/HDL-C ratio. Regression line and 95% CI are given. CI, confidence interval; HDL-C, HDL cholesterol.

Relationship between the M-value at clamp and the interaction between the TG/HDL-C ratio and BMI based on data from reinvestigation at age 70. BMI, body mass index.
Twenty-seven percent of participants showed a TG/HDL-C ratio >1.5 and 18% showed a TG/HDL-C ratio >1.8 at age 70. During a median follow-up period of 13.0 years (maximum 22.0 years), 333 subjects suffered from a CVD. Having a TG/HDL-C ratio >1.5 at age 70 was associated with an increased risk of CVD [HR 1.41, 95% confidence interval (CI) 1.12–1.77, P = 0.003] as well as having a TG/HDL-C ratio >1.8 (HR 1.38, 95% CI 1.07–1.80, P = 0.014).
Discussion
The presence of insulin resistance in apparently healthy individuals is associated with a cluster of cardiometabolic risk factors related to the pathogenesis of a number of significant clinical syndromes. 1,2,22,23 At the simplest level, results of this study indicate that 25% of apparently healthy 50-year-old men with the highest TG/HDL-C plasma concentration ratio were significantly more insulin resistant, with a more adverse cardiometabolic risk profile, compared with the remainder of the population. Using essentially the same classification approach, comparable findings were also observed 14 in another population (mean age ∼50 years) as well as in college students. 24 Thus, it seems that the TG/HDL-C ratio can identify insulin resistance and increased cardiometabolic risk in apparently healthy persons over a wide range of ages. Furthermore, results of the current analysis support prior studies showing that incident CVD is also increased in 25% of an apparently healthy population with the highest TG/HDL-C plasma concentration ratio. 12,14,25
An analysis of the TG/HDL-C ratio versus M-value at euglycemic clamp performed at age 70 in the same cohort showed an inverse relationship at TG/HDL-C ratio values below 1.5. This analysis thus showed that the TG/HDL-C ratio is a valid, although not perfect, proxy for insulin resistance.
The rationale for performing the analysis described and summarized in this article is that it would be useful to have a simple test that could be used in primary care as well as in specialized care to identify insulin resistance and a high CV risk in apparently healthy individuals. It could be argued that establishment of the MetS criteria provides such an approach, 9 and indeed, insulin resistance, cardiometabolic risk profile, and incident CVD were somewhat accentuated in those meeting diagnostic criteria qualifying for the diagnosis of MetS than high-risk groups as identified by the TG/HDL-C ratio.
However, some previous studies found that both the CVD risk profile and CVD outcome were reasonably comparable in apparently healthy persons defined to be at high risk by either MetS or the TG/HDL-C ratio. 14,25 Furthermore, in the current study, only ∼45% of those with a TG/HDL-C ratio >1.8 (Table 1) had MetS. The finding that a greater number of high-risk persons were identified with a high TG/HDL-C ratio than with a diagnosis of MetS is consistent with a previous report. 25 An obvious advantage of using the TG/HDL-C ratio over the MetS criteria to identify high CVD risk in apparently healthy individuals is its simplicity, requiring fewer measurements and avoiding the need to quantify waist circumference, which is a less standardized routine procedure. Furthermore, the present study showed that the TG/HDL-C ratio adds important information to BMI regarding insulin resistance (Fig. 3). Thus, taken together, the TG/HDL-C ratio is simpler to perform in comparison with applying the MetS criteria and should be used in combination with information on obesity.
The present study used a follow-up period of 40 years from age 50, as well as a follow-up from age 70, when a new measurement of the TG/HDL-C ratio was performed. It could then be seen that the HRs from these two time points, although 20 years apart, were almost the same, further validating that the TG/HDL-C ratio could be a useful clinical tool in the middle-aged as well as in the elderly.
However, clinical utility of the TG/HDL-C ratio at present suffers from the absence of a universally accepted cut point with which to separate high- and low-risk persons. This dilemma may be more apparent than real since cardiometabolic risk and incident CVD did not vary substantially when using the TG/HDL-C ratio of 1.8 derived from the ULSAM population or the ratio of 1.5 used in studies of Argentinean and North American men. 13,14,25 It is likely that the previously used cutoff of 1.5 is more accurate than 1.8 (representing the highest quartile of the ratio) used in the present study since lipid levels generally were higher in the early 70s when the baseline investigation in ULSAM was performed than usually seen today.
During the last years, Mendelian randomization studies have shown serum TGs to be causally related to coronary heart disease, while there is a question mark regarding the causality of HDL. 26,27 The present study did not investigate the issue of causality, and the TG/HDL-C ratio was merely used as a marker of insulin resistance.
Among the strengths of the present study is the large follow-up period. A major limitation is that the study only includes men, which limits the generalizability of the findings. In the calculation of MetS, BMI was used instead of waist circumference. This might lead to misclassification of MetS, but we have previously shown that in the same cohort at age 70, this misclassification is <1%. 15
In conclusion, results of this study provide additional evidence that 25% of an apparent healthy male population with the highest TG/HDL-C ratio are more likely to be insulin resistant, with a more adverse cardiometabolic risk profile, and with an increased risk of incident coronary heart disease. 12 –14,25 What remains to be seen is whether or not these biological findings can be translated to a clinical approach that can be used to obtain significant clinical information. The first step is the need to develop sex-specific and racial/ethnic cut points that can be universally applied. 13,28 We hope that the current findings are sufficiently interesting to stimulate other investigators (with relevant experimental populations) to undertake analyses that might move us closer to accomplishing the goal of finding a clinically easily obtainable marker of insulin resistance and high CV risk.
Footnotes
Author Disclosure Statement
E.I. is a scientific advisor for Precision Wellness and Olink Proteomics for work unrelated to the present project. J.S. serves on the advisory board for the fitness company Itrim. No competing financial interests exist for L.L., J.Ä., B.Z., and G.M.R.