
Abstract
Background:
Hypertension and obesity are very common and complex cardiovascular (CV) risk factors. Our aim was to provide a comprehensive assessment of associations between visceral fat depots and vascular or cardiac complications of hypertension.
Methods:
All the consecutive patients (age: 45–80 years old) scheduled for elective coronary angiography in the Department of Cardiology were screened, and 400 patients were included into the study group. All the patients had a comprehensive clinical assessment focused on hypertension and obesity, risk factors, fat depots, and several hypertension-related vascular or cardiac complications.
Results:
The study group (n = 400; F/M: 140/260; age: 61 ± 7 years) included patients with hypertension (n = 354; 88.5%) and normal blood pressure (n = 46; 11.5%) and individuals with obesity (n = 192; 48%), diabetes (n = 139; 35%), metabolic syndrome (n = 240; 60%), and coronary artery disease (n = 286; 71%). Patients with higher degrees of hypertension (grade 3 vs. 2 vs. 1) showed increased body mass index (BMI) and waist circumference and ultrasound indexes of perivascular, epicardial, and abdominal visceral fat with no differences in age, waist–hip ratio, and subcutaneous fat. Both visceral fat depots: perivascular fat (carotid extra-media thickness) and abdominal visceral fat (intra-abdominal thickness) assessed as single measures and ratios were significantly increased in hypertensive patients with high versus low global CV risk in a hypertension-focused risk model (differences more pronounced in patients ≤60 years old). Visceral fat parameters were not independent, but rather additive to general obesity (BMI), except for visceral abdominal fat depot.
Conclusions:
Visceral abdominal and perivascular fat depots assessed as ultrasound indexes are associated with complications of hypertension and CV risk indicators, especially in patients with a mild-to-moderate hypertension and in younger patients.
Obesity may be a cause of hypertension.
The severity of hypertension is associated with the degree of obesity.
The quantity of visceral fat (mainly abdominal and perivascular) is associated with hypertension-related complications in patients with a mild-to-moderate (but not severe) hypertension, especially among all hypertensive patients with obesity [body mass index (BMI) ≥30 kg/m2].
Visceral fat parameters were not independent, but rather additive to general obesity (BMI), except for visceral abdominal fat depot.
Perivascular adipose tissue was associated with vascular stiffness and diastolic dysfunction, but not endothelial function. In contrast, abdominal visceral fat was increased in patients with concentric hypertrophy and diastolic dysfunction and showed trend toward association with increased vascular stiffness.
Introduction
H
The relationship between hypertension and obesity has been established prospectively since the Framingham Heart Study. 4 The assessment of adiposity and CV risk is complex, and in the group of patients with similar degrees of obesity [body mass index (BMI)], individual risk may be different. 5 A growing body of recent evidence suggests that obesity is a very heterogeneous condition, in which fat quantity, distribution, metabolic function, and specific visceral fat depots are closely associated with CV risk. 6
Our aim was to provide a comprehensive assessment of associations between visceral fat depots and vascular or cardiac complications of hypertension.
We are not aware of other studies showing a comprehensive analysis of visceral adipose tissue (VAT) in relation to complications of hypertension. Therefore no particular hypothesis was tested, and the study was explanatory in purpose.
Materials and Methods
The study group
All the consecutive individuals (45–80 years old) scheduled for elective coronary angiography in our Department of Cardiology (stable angina pectoris and/or positive noninvasive tests) were screened, and 400 patients (n = 400) were finally included into the study group (flow chart—Supplementary Fig. S1; Supplementary Data are available online at
The main exclusion criteria were as follows: acute coronary syndrome, left ventricular dysfunction and/or heart failure, severe primary heart valve disease, secondary causes of arterial hypertension, uncontrolled or untreated arterial hypertension, secondary causes of obesity or medical interventions aimed at weight loss (prior 12 months), at least 10% unintentional weight loss (prior 3 months) or risk of malnutrition, neck or abdomen surgery, radiotherapy, a very poor carotid artery image quality, and confirmed diagnosis of genetic predisposition for CVD.
All the patients were recruited in the Department of Cardiology at the Medical University of Silesia, and all of them gave their written informed consent for the study. The study was a cross-sectional analysis with the study protocol approved by the local Medical University of Silesia Ethics Committee.
Risk factors and CVD
All the patients had a comprehensive clinical assessment focused on arterial hypertension, CV risk factors, and hypertension-related vascular or heart complications. Coronary artery disease (CAD) was diagnosed in coronary angiography performed during the hospitalization and defined as stenosis ≥50% in any major coronary artery.
The CV risk estimation was based on the European Society of Cardiology (ESC) guidelines. 7 The following obesity measures were used: BMI, waist circumference (WC), waist–hip ratio (WHR), and body fat percentage (BF%; bioimpedance method). The bioelectric impedance analysis (Bodystat 1500) was used to obtain patients' BF% according to the manufacturer's manual. Hypertension was diagnosed and classified according to the current European Society of Hypertension and ESC guidelines for the management of arterial hypertension. 2 The severity of hypertension was determined based on any evidenced (ambulatory medical records) prior history of hypertension, past and current treatment. 2 Moreover, for each participant, mean BP was calculated as the average of the three office BP measurements taken during the index hospitalization. The following classifications of hypertension were used [systolic blood pressure (SBP) and diastolic blood pressure (DBP)]: grade I (SBP = 140–159 mmHg and/or DBP = 90–99 mmHg), grade II (SBP = 160–179 mmHg and/or DBP = 100–109 mmHg), and grade III (SBP ≥180 mmHg and/or DBP ≥110 mmHg). 2 The diagnosis of dyslipidemia, diabetes, and obesity (classified according to BMI) was defined as previously described. 7 –9 Finally, metabolic syndrome (MS) was diagnosed according to the International Diabetes Federation consensus. 10 Renal function was assessed based on actual serum creatinine level, estimated glomerular filtration rate (eGFR CKD-EPI creatinine equation), and clinical history. Chronic kidney disease (CKD) as a risk factor was defined for the purpose of our study as eGFR <60 mL/min/1.73 m2 with or without kidney damage.
CV risk and hypertension-related complications in hypertensive patients
CV risk factors, asymptomatic organ damage, and established CV and/or renal diseases were determined and defined as in the Table 4 presented in the guidelines. 2
CV risk estimation was based on the severity of arterial hypertension (HA) (1, 2, or 3 points as grade 1, 2, or 3) and hypertension-related complications according to the ESC guidelines (n1): pulse pressure (PP), pulse wave velocity (PWV), carotid intima-media thickness (IMT), chronic kidney disease, left ventricle hypertrophy, left ventricle concentric remodeling, diastolic dysfunction, and the number of coronary arteries with ≥50% narrowing. Afterward, all the patients with HA (n = 354) were defined as low (<8 points) or high (≥8 points) CV risk.
All the hypertension-related complications were determined as described below.
Echocardiography
Transthoracic echocardiography was performed according to the current guidelines 11,12 and included a quantification of the left atrial volume index, left ventricle volume, geometry, hypertrophy, and systolic and diastolic function.
Peripheral artery atherosclerosis, stiffness, and endothelial dysfunction
Carotid femoral PWV was used as a measure of systemic arterial stiffness with the method used according to the expert consensus. 13 PP was defined as the difference between the systolic and diastolic office BP. The ankle–brachial index was defined as the ratio of the SBP measured at the ankle to that measured at the brachial artery. 14 Endothelium-dependent flow-mediated dilatation (FMD) was assessed on the brachial artery according to the standard methods described in our previous study. 15
Carotid IMT and particular fat depots
All the images were obtained by one experienced researcher using constant settings. Afterwards, single images of the particular region of interest were randomly analyzed offline by one observer blinded to patient's data and characteristics. All the measurements were identical in all patients and were obtained with a high-resolution ultrasound (GE Vivid 9; Milwaukee) with a linear or convex transducer.
Carotid IMT was used as a well-evidenced vascular index of arterial atherosclerosis and organ damage. The following ultrasound indexes of adipose tissue were obtained in all our patients: perivascular visceral fat measured as extra media thickness (EMT), epicardial visceral fat measured as epicardial fat thickness, abdominal visceral fat measured as intra-abdominal thickness (IAT), and abdominal subcutaneous adipose tissue (SAT). All the ultrasound indexes were used in our recent studies, and the detailed method of measurements and offline analysis was described in our previous articles. 16 –19
All the individuals were divided into quantiles based on the amount of visceral perivascular (EMT) and abdominal (IAT) fat, and the obesity phenotype score was determined (2.0–4.0 points with increased amount of VAT). Finally, further analysis included the amount of visceral fat indexed to: subcutaneous fat depot (visceral/subcutaneous), general obesity (visceral/BMI), or added to general obesity (visceral × BMI).
Statistical analysis
All the results presented in the text, tables, and figures are expressed as means ± standard deviations or number and percentage. The data normal distribution was analyzed with the Kolmogorov–Smirnov test. Baseline clinical parameters or the ultrasound measures were compared between the subgroups using the t-tests for normally distributed continuous variable (Student's t-test); in case of abnormal distribution, the Mann–Whitney U test was used. Multiple comparison analysis was performed using the analysis of variance (ANOVA) with Bonferroni correction. Before the ANOVA test, Levene's test for equality of variances was performed. The differences between the subgroups were analyzed using one-way ANOVA. Associations between parameters were assessed using Pearson or Spearman correlation analysis, respectively, for the parametric or nonparametric variables. A value P < 0.05 was considered statistically significant. Statistical analysis was undertaken using Statistica software (version 10.0; Stat Soft, PL).
Results
Study group clinical characteristics
The study group (n = 400; females = 35%; age: 61.2 ± 7 years) included patients with hypertension (n = 354; 88.5%) and normal BP (n = 46; 11.5%). Half of the study group had obesity (n = 192; 48%) or central obesity (n = 208; 52%), one third had diabetes (n = 139; 35%), and most had MS (n = 240; 60%). CAD was found in 286 patients (71%), and 89 patients (22%) had a history of peripheral artery disease. The detailed clinical characteristics of our study group with main indexes of hypertension-related organ damage, CVD, and echocardiography parameters are presented in the Table 1.
Clinical Characteristics and Cardiovascular Risk of the Study Group
Body fat percentage assessed in bioelectrical impedance method.
Metabolic syndrome according to the International Diabetes Federation criteria 10 ; current smoking or smoking in the past for at least 1 year.
Risk factors: male sex, age >55 years old, hypertension, hyperlipidemia, obesity, type 2 diabetes, chronic kidney disease, smoking.
High or very high cardiovascular risk according to European Society of Cardiology guidelines. 2
At least 1 major coronary artery with 50% stenosis in coronary angiography.
ACS, acute coronary syndrome; ACE-I, angiotensin converting enzyme inhibitors; ARB, angiotensin receptor blockers; BB, beta blockers; CCB, calcium channel blockers; CV, cardiovascular; PTCA, percutaneous transluminal coronary angioplasty; SD, standard deviation.
Hypertension, obesity, and fat depots
The study group included individuals with different grades of hypertension (mild: n = 126; moderate: n = 152; and severe: n = 76) and the mean number of antihypertensive drugs (2.2 ± 1.1 vs. 2.6 ± 1.1 vs. 3.1 ± 1 drugs; P < 0.05). Patients with higher degrees of hypertension showed increased clinical measures of obesity (BMI and WC) and ultrasound indexes of perivascular, epicardial, and abdominal visceral with no differences in age or SAT (Supplementary Table S1).
Visceral fat depots in hypertensive patients and CV risk
Both visceral fat depots: perivascular fat (carotid EMT) and abdominal visceral fat (IAT) were significantly increased in hypertensive patients with high versus low CV risk. Moreover, both visceral indexes (ratio to subcutaneous fat and multiplied by BMI) were also increased in hypertensive individuals with high versus low CV risk. However, neither abdominal visceral fat nor perivascular fat differentiated CV risk in a group of severe hypertension (Figs. 1 and 2).
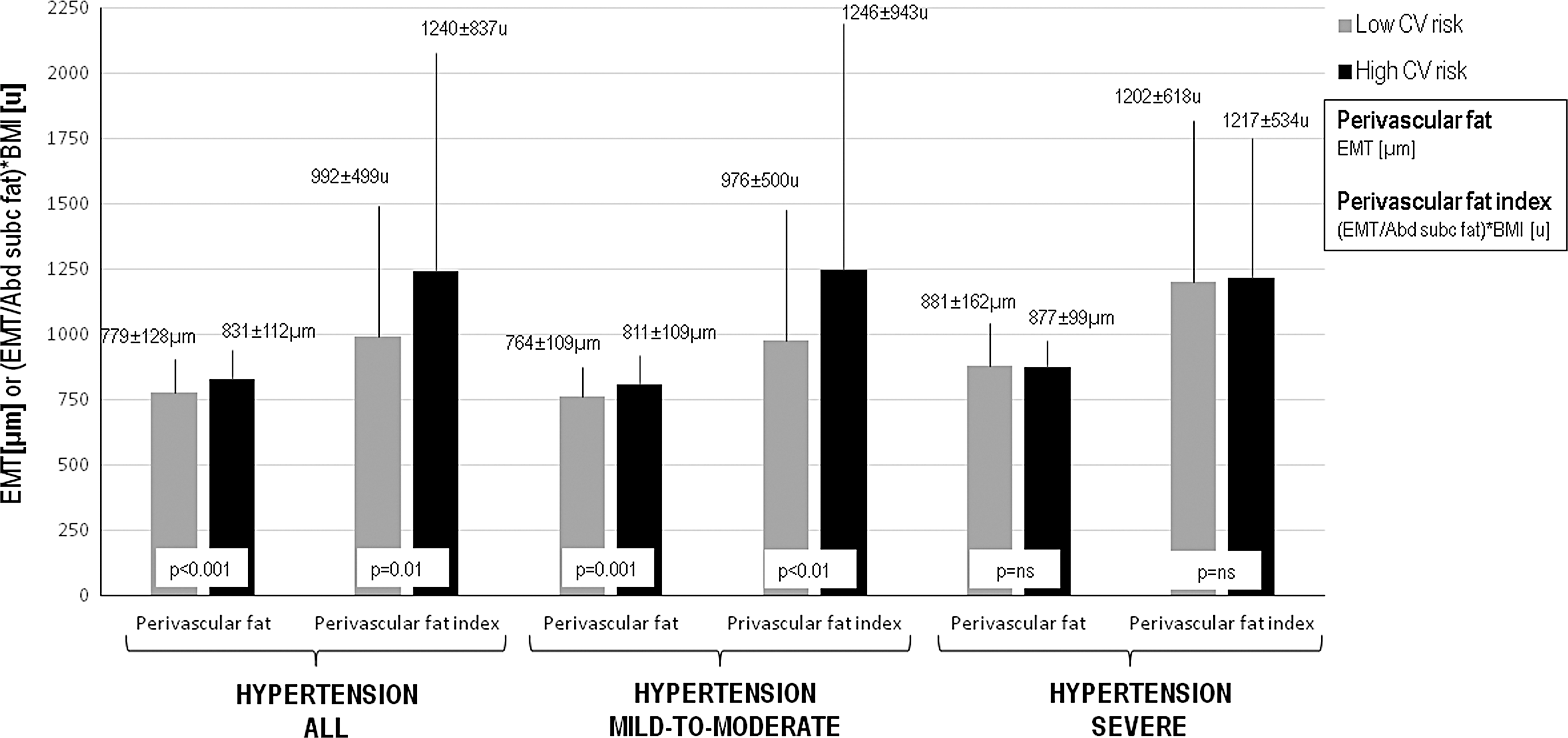
Perivascular fat in hypertensive patients with low and high cardiovascular risk. Results are expressed as mean values and standard deviations in comparison between patients with high and low cardiovascular risk (independent samples t-test). BMI, body mass index; EMT, extra media thickness.
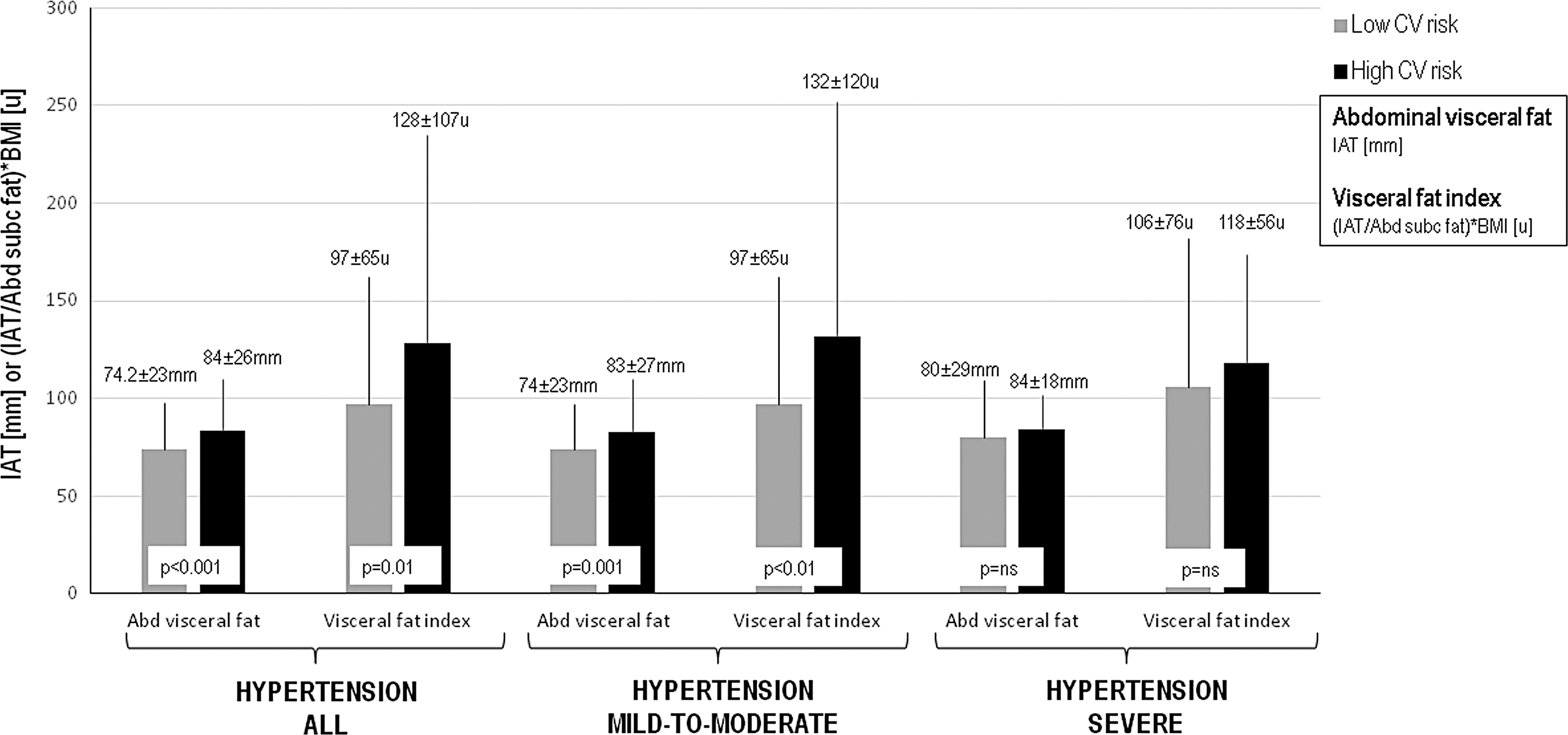
Abdominal visceral fat in hypertensive patients with low and high cardiovascular risk. Results are expressed as mean values and standard deviations in comparison between patients with high and low cardiovascular risk (independent samples t-test). IAT, intra-abdominal thickness.
Obesity and hypertension-related complications
The Table 2 presents correlations between hypertension-related vascular complications and measures of adiposity. Visceral fat indexes revealed moderate associations with ultrasound indexes of vascular stiffness. Endothelial function (FMD) was not associated with any clinical measures of obesity or the type of obesity.
Clinical Measures of Obesity, Fat Depots, and Vascular Complications
Results are expressed as mean values and standard deviations in comparisons between the subgroups (independent samples t-test).
ns, not significant.
The Table 3 provides results on left ventricle geometry, diastolic dysfunction, and adiposity. Patients with diastolic dysfunction revealed significantly increased measures of general obesity, abdominal accumulation of visceral fat, and perivascular fat compared to patients with normal diastolic function. Similar differences, except for perivascular fat, were found between individuals with concentric hypertrophy and normal left ventricle geometry.
Clinical Measures of Obesity, Fat Distribution, and Heart Complications of Hypertension
Results are expressed as mean values and standard deviations in comparisons between the subgroups (independent samples t-test).
Visceral fat depots in obese patients with hypertension and CV risk
All the patients with hypertension (n = 354) were assessed in a more precise risk score focused on the severity of hypertension and its complications (described in the “Materials and Methods” section). Patients with obesity suffering from hypertension (n = 150) were defined as low (<8 points) or high (≥8 points) CV risk, and indexes of adiposity of both groups are provided in the Table 4. Obese patients with hypertension and a high CV risk revealed increased WC and visceral fat indexes, especially the ratio of perivascular-to-subcutaneous fat. Moreover, individuals with high CV risk showed increased values of visceral obesity phenotype (increased rate of visceral abdominal and perivascular fat) compared to low CV risk patients.
Cardiovascular Risk and Obesity Phenotype
CV RISK is based on the severity of hypertension (1, 2, or 3 points as class I, II, or III) and related complications according to the European Society of Cardiology guidelines 2 : pulse pressure, pulse wave velocity, carotid intima-media thickness, chronic kidney disease, left ventricle hypertrophy, left ventricle concentric remodeling, diastolic dysfunction, and number of coronary arteries with ≥50% narrowing. All the hypertensive patients were defined as low (<8 points) or high (≥8 points) cardiovascular risk. Obese patients aged 60 years or younger (n = 146 points) with BMI ≥30.0 kg/m2: low (n = 86 points) versus high (n = 60 points) CV risk. Results are expressed as mean values and standard deviations in comparisons between the subgroups (independent samples t-test).
Abd, abdominal; BMI, body mass index; EMT, extra media thickness; IAT, intra-abdominal thickness; ns, not significant.
The Table 4 presents also data regarding hypertensive patients below 60 years of age. Individuals with high or low CV risk showed significant differences in most parameters of adiposity, especially visceral fat indexes.
Discussion
The principal finding of our study was that the quantity of visceral fat (mainly abdominal and perivascular) was associated with complications of hypertension and increased CV risk in patients with a mild-to-moderate (but not severe) hypertension and even among all hypertensive patients with obesity (BMI ≥30 kg/m2). The differences in visceral fat depots were more pronounced in hypertensive individuals aged 60 years or less. Visceral fat parameters were not independent, but rather additive to general obesity (BMI), except for visceral abdominal fat depot. Perivascular adipose tissue was associated with vascular stiffness and diastolic dysfunction, but not endothelial function. In contrast, abdominal visceral fat was increased in patients with concentric hypertrophy, diastolic dysfunction, and showed trend toward association with increased vascular stiffness. Finally, the severity of hypertension was associated with increased measures of central obesity and indexes of both perivascular and abdominal fat.
To the best of our knowledge, this is the first study providing a comprehensive and complete analysis of obesity, visceral fat depots, and total CV risk in patients with hypertension. Our study group was representative of a real life population of hypertensive patients with a mean number of six risk factors and more than two antihypertensive drugs (almost all with beta blockers and angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers). Most patients (71%) had CAD, every fifth had peripheral artery disease, and even 40% of them had acute coronary syndrome or percutaneous coronary intervention in the history. Although patients with heart failure with reduced ejection fraction were not included in the study, 41% revealed diastolic dysfunction, and half of the patients fulfilled the criteria of echocardiographic left ventricle hypertrophy. Moreover, nearly every second patient showed increased carotid IMT or vascular stiffness.
Carotid EMT is an ultrasound index of common carotid artery, which corresponds mainly to perivascular visceral fat. 20,21 Our previous research showed that carotid EMT is associated with MS, CV risk, the severity or complexity of CAD, and even with the effectiveness of statin therapy in subjects with obesity. 22 –24 Abdominal visceral fat (IAT) was also associated with CV risk factors and cardiometabolic complications, 25 but it was not sensitive enough to predict the severity of CAD. 24 Thus, both indexes—carotid EMT and abdominal IAT—represent different visceral compartments corresponding to more general (cardiac) or metabolic complications (IAT) and local atherosclerosis or vascular complications (EMT).
Obesity measures in hypertension
The clinical measures of general obesity were associated with HA severity and cardiac complications with no association with vascular complications. While there was a clear association between the BMI and the severity of HA, abdominal obesity measure (WC) showed better association with CV risk, especially among younger patients. We found that the waist–hip ratio does not have any role in hypertensive patients.
Ultrasound index of abdominal visceral fat revealed a strong and complete association with the severity of HA, complications and CV risk, which was independent from BMI. Perivascular fat showed mildly weaker associations with HA and added to BMI value as an indicator of high CV risk. Epicardial fat was the weakest visceral fat depot associated with HA, and SAT had no role in hypertensive patients.
Hypertension, obesity, and fat depots
There are several studies on obesity in hypertension focused on obesity as a cause of HA or resistant HA. 26 Both cross-sectional and prospective studies showed that visceral abdominal fat is associated with higher prevalence or incidence of HA independently from general obesity (BMI) or SAT. 27 –31 In our study, individuals with higher degrees of HA showed increased measures of adiposity except for SAT depot. However, the strength of relationship varied among measures and depots with perivascular fat as the strongest associate (significant differences among all the grades of HA). Visceral abdominal fat and clinical measures (BMI, WC) revealed a moderate relationship with no differences between moderate and severe HA.
Obesity and complications of hypertension
Our study showed that patients with vascular stiffness (PWV) revealed increased quantity of all three visceral fat depots compared to individuals with elastic vessels, which is in line with previous studies. 32 –35 However, fat measures were not associated with FMD except for visceral abdominal depot. Large body of evidence suggests that arterial stiffness in obesity is an independent predictor of adverse CVD. It is a risk factor for systolic HA, diastolic dysfunction, and atherosclerosis. 33 Although obesity is a well-evidenced condition with impaired FMD, it is associated with dysfunctional adipose tissue, insulin resistance, and chronic inflammatory state (e.g., diabetes and MS) rather than obesity and the fat quantity itself. 36 –38 Moreover, the ultrasound method of endothelial dysfunction is very sensitive, but susceptible to several risk factors, especially when FMD is used in a cross-sectional study. 39 Therefore, some previous studies also failed to show impaired endothelial dysfunction in patients with obesity. 40 –42
Patients with either concentric hypertrophy or diastolic dysfunction showed increased BMI, WC, and visceral abdominal fat. Increased perivascular fat was found only in patients with diastolic dysfunction. Obesity and visceral fat (abdominal and epicardial) were shown to be associated with left ventricle mass and diastolic dysfunction using different imaging modalities, including echocardiography and the reference method of cardiac magnetic resonance. 43 –47
Adipose tissue depots and hypertension-related CV risk
Our study group was representative for patients diagnosed and treated in cardiological clinical practice. Due to a number of risk factors and co-morbidities, CV risk models recommended in the ESC guidelines 7 are insufficient and would not discriminate a risk. Therefore we used a CV risk model related to HA complications and based on ESC guidelines. 2
Both visceral fat depots (perivascular and abdominal) were significantly increased in hypertensive patients with high compared to low CV risk, except for a group of severe HA. Grade III HA is considered a very high risk state in itself, CV risk estimation in this group seems inappropriate, and it would not change clinical decisions. We found that VAT is a principal component of adiposity affecting HA related risk and complications. However, our results suggest that while abdominal VAT is an independent risk indicator, perivascular VAT provides additive data and modifies the BMI-related risk. Moreover, adiposity phenotype and all obesity measures, including VAT depots, showed a major role in the discrimination of HA-related risk in younger hypertensive patients (≤60 years old). Available evidence suggests that younger the patient stronger the influence of obesity and adiposity on clinical prognosis and life expectancy. 48 Therefore, CV risk discrimination based on visceral fat depot quantification may have the greatest application in young patients with a mild-to-moderate HA. Finally, we focused on a subgroup of hypertensive patients with obesity and showed that central obesity and perivascular fat amount were able to differentiate high and low CV risk.
The precise mechanisms explaining several associations between specific fat depots, VAT, and CV risk in HA are not fully known. A considerable interest in this field resulted in few major linking hypotheses. The primary theory is based on the accumulation of adipose tissue in VAT depots in case of inability of SAT to further store triglycerides. 49 Moreover, lipolytic activity of VAT results in increased passage of free fatty acids through portal circulation to liver leading to hyperinsulinemia and insulin resistance, which seems to be the key metabolic trigger increasing CV risk. 50 Finally, recent years provided several studies, which confirmed that specific adipose tissue depots are involved in synthesis and release of a number of cytokines affecting both metabolic pathways and CV system. 51 The quality of fat and its dysfunction is currently the main hypothesis linking VAT and CVD. Given the anatomical proximity, perivascular fat depot may affect vascular structure (atherosclerosis) and function through the release of cytokines. 51
Limitations and clinical perspectives
There are several articles reporting association between obesity and HA. We present the first article providing a detailed and comprehensive assessment of obesity, fat depots, and CV risk in HA. We are not aware of other studies involving a hypertension-oriented CV risk stratification based on the ESC guidelines. 2 A growing body of evidence indicates that most of vascular clinical events among hypertensive patients occur in a mild-to-moderate HA. 26 However, this subgroup of hypertensive patients reveals a very heterogenous global CV risk profile. Therefore, our results suggest that ultrasound index of VAT depots (abdominal or perivascular) may be used to distinguish CV risk in patients with a mild-to-moderate HA and identify individuals requiring earlier or more intensive pharmacotherapy or more frequent follow-up. Abdominal IAT is an ultrasound measure, which is easier to obtain, and it does not require high ultrasound skills. However, carotid EMT requires more experience in carotid ultrasound, but it is a more precise and sensitive risk marker. Both indexes reflect different aspects of CV risk as various VAT depots are evidenced to increase total CV risk through local or systemic mechanisms.
Our conclusions are based on a cross-sectional study, and further prospective study is needed to confirm the causality among fat measures, global CV risk, and clinical events related to hypertension. Ultrasound indexes provide clinical value if obtained by experienced observers. Our results refer mainly to hypertensive patients with increased CV risk.
Conclusions
Visceral abdominal and perivascular fat depots assessed as ultrasound indexes are associated with complications of hypertension and CV risk indicators, especially in patients with a mild-to-moderate hypertension and among younger patients.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist. All the authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.