
Abstract
Background:
There is little evidence of how metabolic syndrome (MS) affects sympathovagal balance responses to acute physical effort (APE) and autonomic stimulation (AS). This study aimed to evaluate the heart rate variability (HRV) responses to the combined APE and AS challenges.
Methods:
Fourteen subjects (8 men; 49.15 ± 8.67 years) divided into two groups: 7 healthy volunteers [control group (CG)] and 7 patients with MS. Sympathovagal balance [low frequency (LF)/high frequency (HF) ratio] was accessed by HRV through the beat-to-beat heart rate (HR) electrocardiogram. Other variables analyzed were as follows: HR, RR-interval variance (VAR/ms2), LF and HF normalized units (un). The APE consisted of a 30-min walk at 65%–75% of the age-predicted maximal HR. The AS was achieved by changing from the supine to standing position (activity orthostatic position).
Results:
At rest, all HRV variables differ with on MS, but after APE and AS LF (nu) and HF (nu) become similar to the CG. However, the LF/HF ratio responses to the AS were significantly different after APE, but only in the MS (CG rest: 367% ± 59% vs. recovery 495% ± 116%, P > 0.05; MS rest: 316% ± 88% vs. recovery: 665% ± 165%; P = 0.045). Comparing the difference between AS in rest and recovery (ΔAS = rest − recovery), the LF/HF ratio was notably higher in the MS group (CG: 94% ± 29% vs. MS: 415% ± 76%; P < 0.0001).
Conclusions:
The APE and AS induced by body posture changes activated a clear distinction in sympathovagal balance response in MS.
Introduction
Metabolic syndrome (MS) has been associated with increased risk of all causes of morbidity, particularly for cardiovascular diseases. 1 The pathophysiological mechanism underlying MS includes abdominal obesity, dyslipidemia, high blood pressure, and insulin resistance. 2 Each of these components alone can change cardiac autonomic modulation, but together these alterations can lead to a drastic increase in sympathetic nervous system activity (SNSA) that is considered to have a pivotal role in circulatory and metabolic dysfunction. 3,4
SNSA is believed to have an effect on MS development. It was first proposed in a large longitudinal study evaluating 1933 individuals, aged 18–65 years. 5 Two years after a first interview, a blood analysis (fasting state), electrocardiogram, and impedance cardiogram were performed, and a linear relationship was observed between the indirect measure of SNSA, such as “dose–response effect,” and the prediction of new-onset MS. Conversely, high parasympathetic activity emerged as a protective factor against new-onset MS.
Heart rate variability (HRV) is included as an indirect method, usually used to determine SNSA. 6 Changes in HRV have been described early on in individuals with MS, 7 –9 and there are many reports 10 –16 showing the time-domain and frequency-domain of the HRV analysis consistently with an increased SNSA. Autonomic cardiac modulation can be evaluated by sympathovagal balance, achieved through the ratio between the low frequency (LF) and high frequency (HF) of the HRV. Sympathovagal balance (LF/HF ratio) is known to be related to some autonomic stimulation (AS), where the sympathetic activity is classically high, as observed during standing when compared with the supine posture. 6
However, there is no consensus regarding which HRV components can be used as markers of cardiovascular risk factors. Heart rate (HR) remains to be fully explored and some results are indeed hopeful. For example, elevated resting HR was identified as a predictor of MS development in individuals with cardiovascular risk factors for men and women. 17 The HR recovery after acute physical effort (APE) also seems to be another pertinent variable because a 20-year follow-up study involving 2730 volunteers found greater development of hypertension, diabetes, and MS when a slow HR recovery was recorded after a graded exercise test on a treadmill. 18
The aforementioned studies used different approaches to access autonomic cardiovascular control in patients with risk factors for cardiac diseases, but none of these researches evaluated the sympathovagal balance of the HRV analysis, together with APE and AS. Given this scenario, this study aimed to evaluate the possible relationship between cardiovascular overload produced by MS on the sympathovagal balance (LF/HF ratio) responses to the APE and AS challenges, as an alternative way of analyzing autonomic characteristics linked to metabolic disorders.
Methods
Design and subjects
This study was performed at the Rehabilitation Center of the Pontifical Catholic University of Rio Grande do Sul (PUCRS) and included 14 subjects aged between 18 and 65 years (8 men and 6 women; aged 49.15 ± 8.67 years), divided into two groups: a control group (CG) with 7 healthy volunteers and a patient group composed of 7 individuals diagnosed with MS, who attended the Cardiovascular Risk Outpatient unit of the Hospital São Lucas (HSL/PUCRS). The inclusion criteria considered sedentary patients with cardiovascular risk factors well matched to the MS diagnoses. The CG also included sedentary volunteers able to walk/run on a treadmill. Volunteers in a physical rehabilitation program were excluded, and also those with (1) documented autonomic dysfunction, (2) ischemic cardiopathy, (3) heart failure, (4) any cardiac arrhythmia, (5) obstructive pulmonary disorders, (6) peripheral vascular disease, (7) central or peripheral neurologic dysfunction, and (8) muscle or orthopedic limitations limiting their ability to walk/run on a treadmill.
The Research Ethics Committee of the HSL/PUCRS approved the study under protocol number 06/03024 and all procedures were conducted in accordance with the Declaration of Helsinki. All participants were informed about the protocol before initiation of the study and signed an informed consent form.
Sample size
An earlier report showed a 2.5 times increase in indirect sympathovagal balance expressed by the LF/HF ratio of the HRV after exercise. 19 Therefore, the sample size calculation indicated that seven subjects were required in each group to detect the effect for a power of 90% at a 0.05 significance level.
Procedures
The same independent physician performed the diagnosis of MS according to the Adult Treatment Panel (ATP III) criteria. 20 The clinical characteristics of the sample are given in Table 1.
Clinical Characteristics
Data are given as mean ± SD.
P, P value of the statistical analyses (Student's t-test for unpaired samples).
CG, control group (n = 7); MS, metabolic syndrome group (n = 7); BMI, body mass index; WC, waist circumference; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; Tg, triglycerides; AIP, log.(TG/HDL-C); FPG, fast plasma glucose; HOMA [(Glucose/18) × insulin]/22.5, homeostatic model assessment for insulin resistance; hs-CRP, high-sensitivity C-protein reactivity; SBP, systolic blood pressure; DBP, diastolic blood pressure; SD, standard deviation.
Chemicals
All chemicals used in this study were purchased from Sigma Chemical Co. (St. Louis, MO) and were of analytical grade or the highest grade available. Chemical analysis was performed at an independent laboratory.
Biochemical variables
All blood samples were collected between 8:00 and 9:00 a.m. after overnight fasting and before physical effort. Blood samples were collected in heparinized tubes and immediately centrifuged at room temperature for 10 min at 3000 rpm. The supernatant was transferred to cryotubes and aliquots were stored at −70°C until assayed for high-sensitivity C-reactive protein (hs-CRP), glucose, and lipid profiles. Plasma glucose, total serum cholesterol, serum triglycerides, and serum high-density lipoprotein cholesterol levels were measured by standard enzymatic methods using reagents in a fully automated analyzer (Vitros 950 dry chemistry system; Johnson & Johnson, Rochester, NY). Low-density lipoprotein cholesterol (LDL-C) was estimated using the Friedewald equation. 21 The hs-CRP was measured using the ADVIA Centaur® immunoassay system (Siemens Medical Solutions Diagnostics, Frimley, Surrey, United Kingdom). All biochemical analyses were conducted at an independent hospital laboratory.
Clinical and anthropometric variables
Blood pressure was measured using a mercury sphygmomanometer, with participants in a seated position and after a 10-min period of rest. Two separate measurements were recorded, as recommended in the Brazilian Guidelines. 22 Anthropometric measurements included weight, height, and abdominal circumference. 23,24
HRV analysis
One week after clinical evaluation, the volunteers returned to start the HRV and APE procedures. The HRV was assessed through the beat-to-beat HR recorded by an electrocardiogram monitor. The analog signal was transformed into digital using the DATAQ WinDaq® acquisition system (Akron, OH) with a 1000 Hz sample rate. Two variables were evaluated for time-domain: HR (bpm) and RR-interval variance (VAR/ms2). Frequency-domain was performed with an autoregressive algorithm. 6,25 Three main spectral components were considered: very LF from 0 to 0.04 Hz; LF from 0.04 to 0.15 Hz; and HF from 0.15 to 0.40 Hz. Frequency-domain analyses employed three variables: LF normalized units (LF-nu); HF normalized units (HF-nu) and sympathovagal balance expressed by the LF/HF ratio.
All data were recorded between 8:00 and 11:00 a.m. in a quiet room with a temperature of 23°C. The volunteer spent 10-min at rest in the supine position before an electrocardiogram was recorded. Another 10-min resting period was observed after the APE, to achieve a stable electrocardiogram recording for the recovery phase. Two body positions were used for each electrocardiogram recording session (10-min per position), always in the same order: supine position followed by standing [activity orthostatic position (AOP)]. Measurements of HRV were recorded for a continuous period of 250–350 heart cycle segments.
Autonomic stimulation
The orthostatic stress affects the autonomic cardiovascular control and HRV, shifting to a more sympathetic dominance, in which LF increased and HF decreased, indicating a sympathovagal balance response that correlates with autonomic adjustment. 6,25 Therefore, AS was determined by the percentage difference in LF/HF ratio between the AOP and supine position, as described: AS = [(LF/HR ratio in AOP × 100) ÷ LF/HR ratio in supine position] −100. The AS effects on relative changes of the sympathovagal balance in rest conditions were compared with the recovery phases after APE. The delta AS between rest and recovery phases was determined as follows: (ΔAS = AS recovery − AS rest).
Acute physical effort
The exercise session lasted 40 min: 3-min stretching, 3-min warm-up (walking at 3.2 km/hr without incline), 30-min walk at a moderate and constant workload, and 3-min cool-down returning to a low velocity (3.2 km/hr). An HR monitor (POLAR®; Oulu, Finland) was used to measure HR, aimed at indicating 65% and 75% of the age-related maximum HR. 23,24
General considerations
All volunteers were advised to avoid caffeine or alcohol consumption and additional physical exercise for at least 48 hr before testing. All volunteers were nonsmokers. One volunteer with MS was taking beta-blocker medication for hypertension and for this reason a 7-day washout period was requested, before starting the protocol procedures, and this medication was substituted by a diuretic. No volunteers had used alpha-blockers or any drug that promotes inhibition of the cardiovascular central control. An independent blinded investigator conducted all the HRV analyses.
Statistical analysis
Results were expressed as mean (±standard deviation). Groups and rest and recovery situations were compared using Student's t-test. Two-way repeated-measures analysis of variance and Tukey's post hoc test were also used. The correlation between HR and HRV was analyzed by Pearson measures. A P value of ≤0.05 was considered to be statistically significant.
Results
All typical components of MS were significantly different between the two groups, regardless of gender. Moreover, other risk factors for cardiovascular diseases were also significantly higher within the MS volunteer group [AIP, homeostatic model assessment (HOMA), and hs-CRP]. However, age, total cholesterol, and LDL-C were similar between the groups (Table 1). The MS volunteers were also classified as class 1 for obesity (body mass index >30 kg/m2), 26,27 insulin resistance (HOMA >4.38), 28 high atherogenic index of plasma (AIP >0.42) 29 and low-grade inflammation (hs-CRP ≈0.8). 30
HRV during supine position
Besides having these metabolic alterations and higher blood pressure levels, the MS group also presented significant differences in all HRV variables analyzed during rest (Table 2). However, the LF-nu and HF-nu in the recovery phases (after APE) were similar to the CG. Physical exercise affected all HRV variables in the CG, whereas only the HR and LF/HF ratio were modified in the MS group.
Effect of the Acute Physical Exercise on Heart Rate Variability
Data are given as mean ± SD of the sample.
Statistical analyses were performed by two-way repeated-measures analysis of variance and Tukey's post hoc test.
P < 0.05 rest versus recovery.
P < 0.05 CG versus MS.
SP, supine position; AOP, activity orthostatic position; HR, heart rate; VAR, heart rate variability on time-domain; LF-nu, low frequency normalized units; HF-nu, high frequency normalized units; LF/HF, sympathovagal balance.
HRV during AOP
During AOP, LF-nu and HF-nu showed no significant difference when the two groups were compared. In this body position, APE affected HRV variables in both groups, but the difference observed at rest remained during the recovery phase. The VAR/ms2 and LF-nu were significantly reduced in the MS group when compared with the CG (Table 2).
Sympathovagal balance responses to AS
The AS was achieved in this study by changing the body position from supine position to standing that imposed a gravitational challenge to the cardiovascular system. The LF/HF ratio alteration was used to describe the autonomic cardiovascular control responses to AS. Both groups showed an increase in sympathovagal balance after AS in the rest and recovery conditions (Fig. 1A). However, in the MS group, this response was intensified by APE (CG rest: 367% ± 59% vs. CG recovery 495% ± 116%, P > 0.05; MS rest: 316% ± 88% vs. MS recovery: 665% ± 165%; P = 0.045).
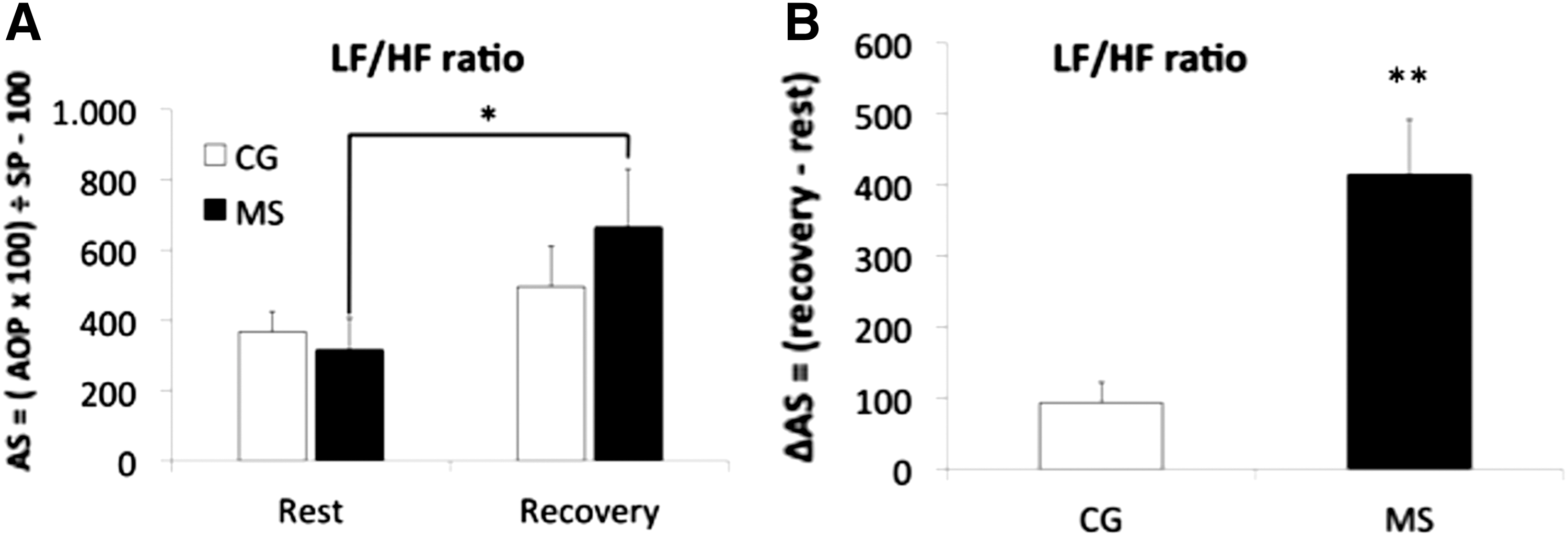
The data express the relative (%) LF/HF ratio responses to AS on rest and recovery phases, where SP is supine position; AOP, activity orthostatic position [*P < 0.05 in
The most important finding emerged when the difference between the rest and recovery AS reaction was calculated. Figure 1B presents the discrepancy in the MS group responses (CG: 94 ± 29 vs. MS: 415 ± 77; P < 0.001). In addition, there was a good correlation between HR and HRV as given in Fig. 2, particularly for RR-VAR (ms2), LF/HF ratio, and LF (nu).

Pearson correlation between HR and HRV. HR, heart rate; HRV, HR variability.
Discussion
Clinical characteristics of MS have been shown to be significantly different in relation to the HRV variables studied, even when a small number of volunteers were analyzed. This alteration in HR control became even more pronounced in our study when AS was evaluated after prolonged moderate walking on a treadmill. This combination induced an important difference between the healthy individuals and patients with MS on sympathovagal balance (expressed by LF/HF ratio) recorded during the recovery phase.
A higher HR was sustained for the MS group in all segments of the study. The same type of response was observed when the sympathovagal balance was evaluated. When these findings are put together, they strongly indicate a higher sympathetic dominance of the autonomic cardiovascular control. However, the unequivocal difference in the LF/HF ratio between the rest and recovery phases to the AS sheds new light on the applications for the use of sympathovagal balance. It is possible that physical exercise and orthostatic stress can help to detect early autonomic dysfunction that can be used for the management and treatment of patients.
Moreover, the RR-VAR (ms2) was consistently lower in the MS group and can also help discriminate between healthy and unhealthy individuals, through this noninvasive autonomic system evaluation. However, no direct measure was used to analyze sympathetic or parasympathetic branch functions, and therefore it is not possible to state the physiological mechanisms that are involved in the observed responses of the autonomic system.
Nonetheless, it is likely that acute physical exercise causes, at least in part, an autonomic heart control adjustment that can be equivalent to that required in MS disorders. During the recovery phase, a better relationship of HRV parameters between the groups was observed; on the contrary, there were fewer pre–post changes in the MS group. These findings suggest that HRV modifications caused by MS could be compared with HRV alterations recorded during the recovery phase in healthy individuals after APE.
The autonomic modulation adjustment, produced by APE, is likely to induce additional effects on AS responses in MS and can explain the high LF/HF reaction noted during recovery. The significantly high LF/HF ratio responses to orthostatic stress reinforce the sympathetic damage associated with MS. Nevertheless, the main implication of this investigation lies in the subsequent determination of differences between the rest and recovery LF/HF ratio responses to AS. This suggests that the combination of two stressors can help investigate early autonomic dysfunction related to SNSA.
Previous studies have shown that cardiovascular risk factors involved in the diagnosis of MS present HRV variables with a more dominant sympathetic activity. 4,5 Licht et al. 5 evaluated 1833 volunteers with MS for the risk factor relationship between the autonomic nervous system and hypothalamic–pituitary–adrenal (HPA) axis: The Netherlands Study of Depression and Anxiety. The HR was positively associated with MS, the number of metabolic abnormalities and all individual components used in MS diagnosis. However, none of the HPA axis measurements were related to MS or its components. These results introduce the concept of the main cardiovascular change in MS being more a result of cardiac autonomic modulation than HPA disruption. The main cardiac autonomic disruption is attributed to an increase in sympathetic activity, 31 where the HRV alterations are associated with glycemic status. 32 The HR responses to metabolic stress stimulated during exercise tests have been used as a mortality predictor. 33 There are many autonomic system interactions in response to physical stress 34 that can be analyzed by HRV and give some indications about cardiovascular autonomic control injury.
Our results corroborate this theory and show an HRV pattern linked to increased sympathetic activity in MS. In this regard, HR (bpm) and VAR (ms2) were significantly higher and lower, respectively, in all recorded conditions. These findings were consistently independent from the body positions and physical conditions.
As described by Goldberger, 35 two important time-domain variables, RR-interval variance of HR and HR, could be used to predict sympathovagal balance. More recently, Goldberger et al. 36 evaluated HR and RR interval in the postexercise recovery period. Using a single and double autonomic blockade and a linear model to analyze the parasympathetic, sympathetic, and magnitude of the parasympathetic–sympathetic interactions, they observed that a decrease in HR is a better reflection of the decline in epinephrine and norepinephrine plasma levels during recovery than of an increase in the magnitude of RR interval. In fact, changes in autonomic tone after the cessation of exercise, namely the withdrawal of sympathoexcitation and parasympathetic reactivation, affect HR because of physiological changes related to sinus node activity, which help to distinguish it from pathological cardiovascular conditions as a prognostic factor. 36
There is a strong correlation between time and frequency through the HRV analyses, as a function of a mathematical and physiological relationship. 37,38 All different methods analyze the same RR-interval variations based on the changes in cardiovascular autonomic control, intra-thorax pressure oscillations created by the respiratory cycle, local and systemic hormonal influences, and oscillations in blood pressure generated by plasmatic volume changes and vasoconstrictor and vasodilation agents. 6 However, even during controlled rest conditions, the redundant mechanisms of blood pressure control change the RR interval in a nonlinear, inverse mathematical relationship with HR form. 38 –41 Therefore, shorter RR intervals are likely to present less variation, having a strong influence on HR in HRV analysis. 37
Nieminen et al. 37 proposed that an increase in HR leads to a consequent decrease in VAR (ms2). Accordingly, the persistent elevated HR could explain the low VAR (ms2) in MS. As previously described, the most common negative effects of MS on HRV variables at rest are a high HR, low VAR (ms2), high LF (nu), low HF (nu), and a high LF/HF ratio. However, after physical exercise, a high HR is a common change observed in MS patients. 3 –5,7 –16
Usually, HR increase depends either on an increase in the sympathetic or decrease in the parasympathetic modulations. None of the volunteers included in this study presented an arrhythmic type of disease. This is an important point to consider as the HRV increase observed in this sample was probably caused by the autonomic heart control reflexes and metabolic aftermath of physical activity. Interestingly, the electrocardiogram during the recovery phase was recorded 20 min after physical activity ceased, in a stable condition. These findings corroborate those from Carnethon et al. 18 and justify the inclusion of HR during recovery, as a marker of cardiovascular risk factor.
The LF/HF ratio response to AS has been less investigated in MS populations, and therefore, knowledge regarding the effects of APE on HRV responses to AS is unclear in MS disorders. Our results support the idea that metabolic and homeostatic stress induced by physical activity could be used in combination with orthostatic stress as a new way to assess premature autonomic heart control abnormalities in patients with cardiovascular risk factors. Experimental and clinical researches 6,25 have demonstrated a very close correlation between HRV and cardiac autonomic modulation, but no HRV component was fully established as an unequivocal predictor of cardiovascular diseases. It is too early to accept the method described here; however, combining postural and acute physical challenges could be a promising way to detect early SNSA intensification through the LF/HF ratio investigation. The difference between the rest–recovery LF/HF ratio responses to AS would appear to be a possible approach for amplifying the autonomic system disturbance.
Limitations
Reyes et al. 40 refute the use of the LF and LF/HF ratio as an index of sympathetic activity. Therefore, our study could have applied measurements of plasma catecholamine or assessed muscle sympathetic nerve activity, to directly evaluate the autonomic nervous system that could be used to give more evidence in relation to sympathetic activity disruption in MS. Baroreflex sensitivity analysis also contributes to the identification of blood pressure control disturbances during physical exercise and orthostatic stress. On the contrary, even with a small sample size, our study data analyses confirmed the presented results and could feasibly be part of a larger study to investigate the effects of APE and orthostatic stress upon cardiovascular autonomic control.
Further contributions
The significance of this study is the possibility of being able to use the acute effects of physical exercise and body posture changes to detect early alterations in cardiovascular control. However, it is advisable to simplify the procedures to test LF/HF ratio responses to the physical challenges in a large and prospective study. Early detection could allow timely treatment for SSNA disruption with the potential aim of preventing the autonomic imbalances widely observed in MS, such as already occurs in renal denervation for high blood pressure 42 and carotid stimulation in heart failure patients. 43
Conclusion
APE affects HRV, which is correlated with increased sympathetic modulation, and therefore, enhances the difference between rest and recovery LF/HF ratio responses to AS when MS is present. This suggests that physical stressors can be used to identify early alterations in autonomic control impairment related to cardiac risk factors.
Footnotes
Acknowledgments
The authors thank Dr. Luis Carlos Bodanese, Dra. Karine Rabello Casali, Dra. Maria Claudia Irigoyen, and Dr. Rodrigo Della Méa Plentz for all their support.
Authors' Contributions
F.E.M. and A.M.P.F. contributed with data collection, interpretation and the writing of the article. T.R. contributed with critical reviewing and writing.
Author Disclosure Statement
No conflicting financial interests exist.