
Abstract
Aim:
To understand age- and gender-related differences and secular trends in coronary artery disease (CAD) lipid profiles and the characteristic of dyslipidemia in western China.
Methods:
An age-matched case–control study, including 2400 patients and 1200 controls was performed. All blood lipid tests evaluated from January 2012 to January 2015 at First Affiliated Hospital of Xinjiang Medical University were analyzed. Details of the gender and age of the patients were available. Trends were calculated using linear regression and Mantel–Haenszel X2 analyses.
Results:
We determined the associations among total cholesterol (TC), triglycerides (TGs), low-density lipoprotein cholesterol (LDL-C), apolipoprotein A-1 (apoA-1), apolipoprotein B (apoB), nonhigh-density lipoprotein cholesterol (non-HDL-C), and high-density lipoprotein cholesterol (HDL-C) with CAD for different ages and gender. Except for patients who were <40 years old, the plasma levels of TC, TG, LDL-C, non-HDL-C, apoB, and apoB/apoA-1 were higher in the cases than in controls, and the average levels of these markers decreased significantly as age increased. In contrast, the levels of apoA-1 and HDL-C were significantly higher in the controls than in the patients, and the levels of these markers significantly increased as age increased. Women had higher levels of TC, LDL-C, non-HDL-C, and apoB and a higher value of the apoB/apoA-1 ratio compared to men. The decrease in the average levels of these markers with age was significantly lower in women compared to men. Logistic regression was used to compute the odds ratio of CAD for a one standard deviation change in each lipid marker. Most notably, the apoB/apoA-1 ratio could be a strong risk factor for CAD, and increasing values of the ratio showed a curved line for the graph of the relationship between the ratio and risk.
Conclusions:
Our results confirmed that serum lipid levels in patients with CAD varied by age and gender. The apoB/apoA-1 ratio remains a strong risk factor for CAD.
Introduction
As dyslipidemia is a principal risk factor for cardiovascular disease (CVD), optimization of its treatment remains a health care priority. 1,2 However, the extent to which the lipid profile directly induces CVD or represents a biomarker for risk has been debated for years. A scientific statement from the American Heart Association claimed that a long-standing association exists between elevated triglyceride (TG) levels and CVD. 3 A meta-analysis that included 302,430 people without initial vascular disease from 68 long-term prospective studies concluded that, in contrast with previous findings, TG concentration was not independently related to CHD risk after controlling for high-density lipoprotein cholesterol (HDL-C), nonhigh-density lipoprotein cholesterol (non-HDL-C), and other standard risk factors. In contrast, with the null TG findings after performing adjustment, HDL-C and non-HDL-C were both strongly associated, in opposite directions, with CHD risk in an approximately log-linear manner. 4 A large body of evidence supports the reduction of low-density lipoprotein cholesterol (LDL-C) as the primary objective of dyslipidemia management, 5 –7 and the administration of statins is considered the most effective regimen for achieving this. The results of previous randomized clinical trials have shown that interventions for lowering LDL-C concentrations can significantly reduce the incidence of coronary artery disease (CAD) and other major vascular events. A prospective meta-analysis of data from 90,056 individuals from 14 randomized trials of statins was conducted, over a mean of follow-up of 5 years, and it showed that there was a 12% proportional reduction in all-cause mortality and a 19% reduction in coronary mortality per millimolar reduction in LDL-C. 8 However, several epidemiological and clinical studies demonstrated that patients even with LDL-C values below 70 mg/dL had the so-called residual risk for atherothrombotic events. 9 –11 During the last several years, interest in this field has focused on the importance of lipid-transporting apolipoproteins. Apolipoprotein B (apoB) transports all potentially atherogenic very LDL, intermediate-density lipoprotein and LDL particles, and apolipoprotein A-1 (apoA-1) transports and acts as the major antiatherogenic protein in the HDL particles. The serum apoB level and the apoB/apoA ratio can be used as risk factors for cardiovascular diseases and as new targets for lipid reduction treatment strategies, which has been confirmed in relevant studies. 12,13 Expert opinion is divided in whether the assessment of apoA-1 and apoB levels should replace the assessment of HDL-C and total cholesterol (TC) levels in the assessment of vascular risk. 14,15 Thus, the relationship between different lipid components of blood and CVD remains controversial. On the other hand, age and gender are strong determinants of CAD risk; however, until now, attention has been focused on whether markers of the atherogenic lipoproteins remain predictive in older individuals, and whether these particles create greater risk for younger individuals has not been specifically addressed. Thus, we performed a case–control study to compare the associations of the TG, TC, LDL-C, non-HDL-C, apoB, and apoA-1 levels and the apoB/apoA-1 ratio with coronary events for different ages and genders.
Methods
This retrospective case–control study was conducted at the First Affiliated Hospital of Xinjiang Medical University. Ethical approval for the study was obtained. The case records of all patients presenting with acute CAD and who were hospitalized in the coronary care unit of our hospital between January 2012 and January 2015 were analyzed retrospectively. Subjects (3767 subjects) were consecutively enrolled in this study. The diagnosis of CAD was defined in accordance with the 1979 WHO diagnostic criteria. 16 Subjects were diagnosed with CAD (2463 patients) by the presence of at least one significant coronary artery stenosis of ≥50% luminal diameter on coronary angiography. Healthy controls (1304 controls) were defined as having no presence of coronary artery stenosis of ≥50% luminal diameter. Following the exclusion of individuals with noncardiac complaints or cerebrovascular disease, cancer, severe mental disorders, or chronic kidney disease, as well as individuals with acute and chronic liver disease, infectious diseases, and acute and chronic fevers of unknown origin, 2400 CAD patients and 1243 healthy controls were enrolled in the study. After age matching was performed between the cases and controls, a total of 2400 cases and 1200 controls were included in the final analysis. A flowchart of our study selection protocol is shown (Fig. 1). Smoking and drinking status were defined as current tobacco or alcohol use. The guidelines used for the diagnosis of dyslipidemia, essential hypertension (EH), and diabetes mellitus (DM) in this study have been described elsewhere. The definition of drug treatment for patients used in this study is as follows: patients receive drug treatment for more than 1 month and take medicine for treatment regularly. Fasting lipid profiles, including the levels of TG, TC, HDL-C, LDL-C, apoA-1, and apoB, and the measurement of body mass index, were also noted.
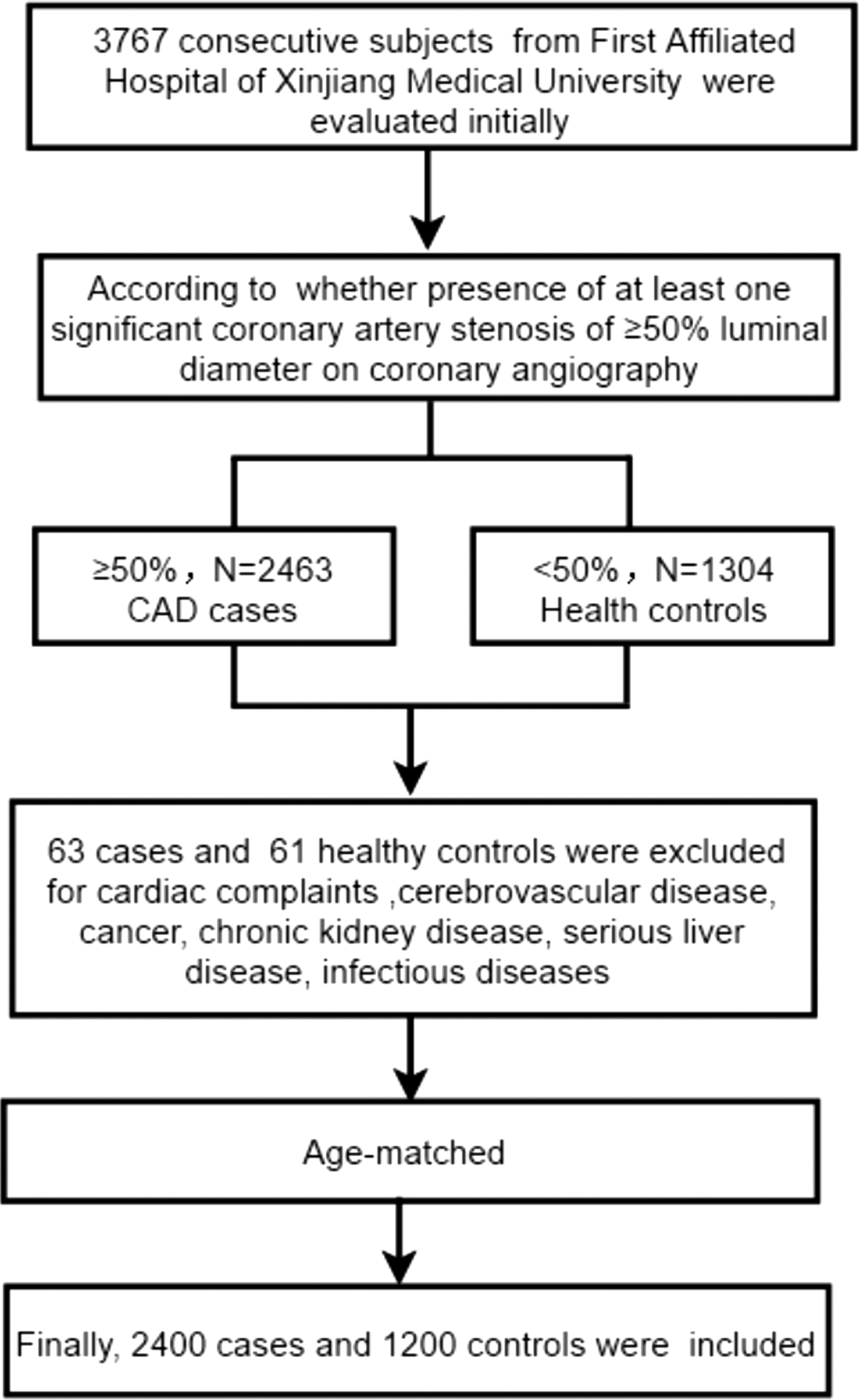
A flow chart of the study.
Statistical analysis
Data from continuous variables are presented as the mean ± standard deviation (SD) and were compared using an independent samples t-test. Data from categorical variables are expressed as frequencies and percentages and were compared using the chi-square test. Subjects were then categorized by age in decades. The mean and SD of selected lipid parameters across different age groups overall and by case or control status of the participants were computed. These included the TG, TC, apoA-1, apoB, LDL-C, and HDL-C levels and apoB/apoA-1 ratio, as well as the non-HDL-C level, which was computed by subtracting the HDL-C level from the TC level. Tests of linear trends were also performed using orthogonal contrasts across age and sex categories. Multivariate logistic regression was used to compute the odds ratio (OR) of CAD for 1 SD change in each lipid marker. All statistical analyses were performed with Statistical Package for the Social Sciences (SPSS, Inc., Chicago, IL), version 22.0. A two-sided value of P < 0.05 was considered significant.
Results
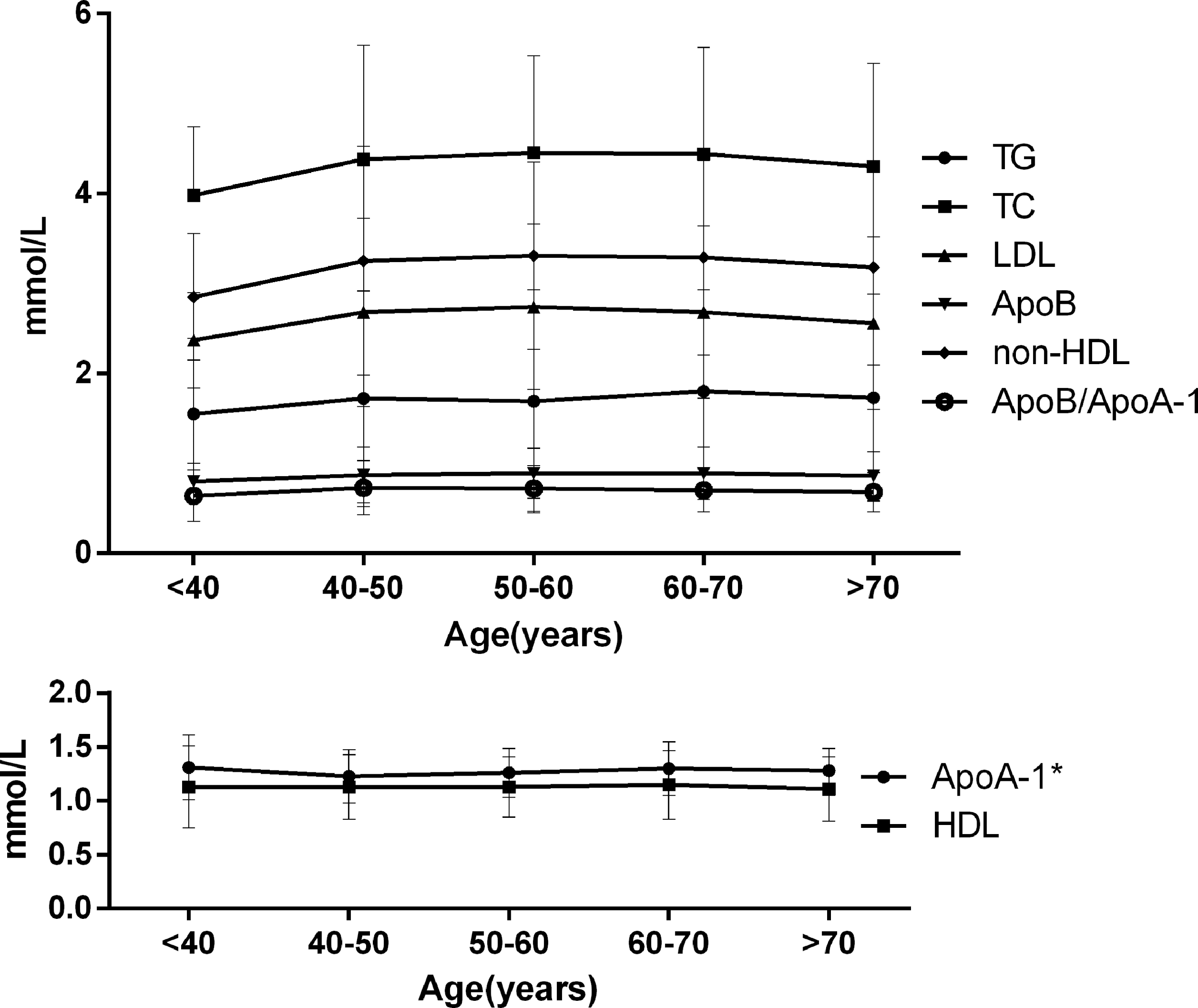
A total of 3600 subjects, including 2400 (66.67%) patients and 1200 (33.33%) healthy controls, were included in this study. The mean age of those in the case group was 57.7 ± 10.6 years; 68.67% (1648) of these subjects were male. The male patients in the case group were younger than those in the control group; however, for females, those in the case group were older than those in the control group. Table 1 lists the baseline characteristics of the study population. The rates of smoking and statin treatment, as well as the histories of EH and DM, were significantly higher in the CAD patients than in the controls. Compared with the controls, the CAD patients had higher levels of TC, TG, aopB, non-HDL-C, and LDL-C and had a higher aopB/apoA-1 ratio. In contrast, the level of HDL-C was lower in the CAD patients than in the controls. In subgroup analyses that were stratified by gender, we found that all of the lipid profiles were associated with CAD risk in both males and females. We also found that all of the lipid profiles varied for the different genders. All were higher in female patients than in male patients, except for the TG level and the apoB/apoA-1 ratio (Fig. 2). The number of participants and the average lipid levels grouped by age are described in Table 2. Most lipid levels increase at <40 years of age, peak at 40–50 years of age, and then decline with age thereafter. This trend is presented in Fig. 3. Tables 3 and 4 describe the average levels of the lipid markers by age category separately for the CAD patients and health controls, respectively. At the same age, comparing patients to controls of the same age, except for the youngest subjects (<40 years of age) that contained the smallest numbers of cases, the levels of TG, TC, LDL-C, apoB, and non-HDL-C and the apoB/apoA-1 ratio (P < 0.001) were significantly higher in the patients than in the controls, and the HDL-C level was significantly higher in the controls. The variation in the trends of average lipid and apolipoprotein levels by different gender is described in Figs. 4 and 5. After adjusting for multiple clinical factors, including age, diabetes, hypertension, and smoking, we found that all of the lipid parameters could be powerful risk factors for CAD. A high apoB/apoA-1 ratio was strongly related to an increased CAD risk. This ratio was superior to any of the cholesterol parameters in predicting risk (Table 5). In fact, the OR adjusted by age, gender, hypertension, and diabetes presented a linear increase in CAD risk after the eighth decile, as shown in Fig. 6.
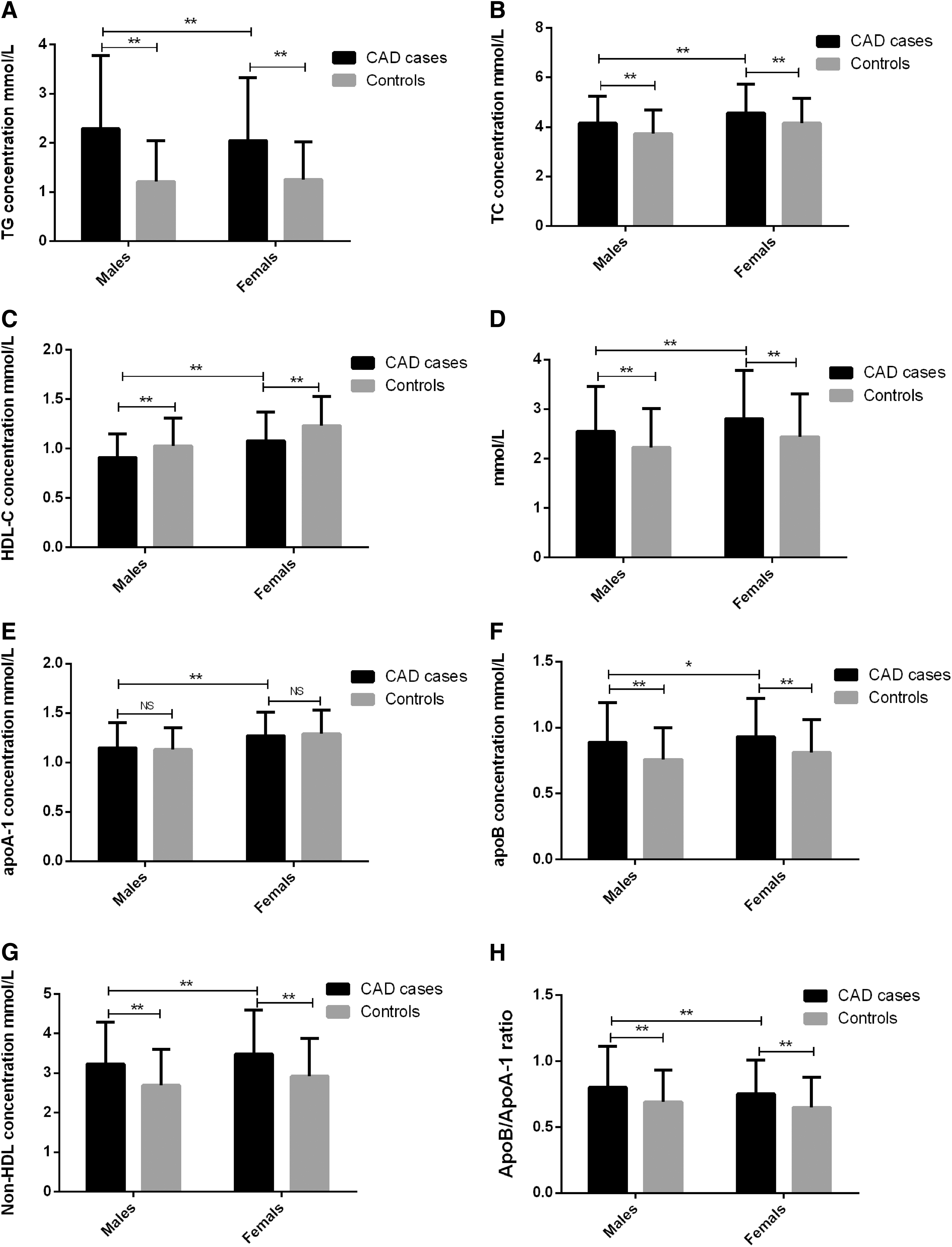
Associations between lipid parameters and CAD risk by gender
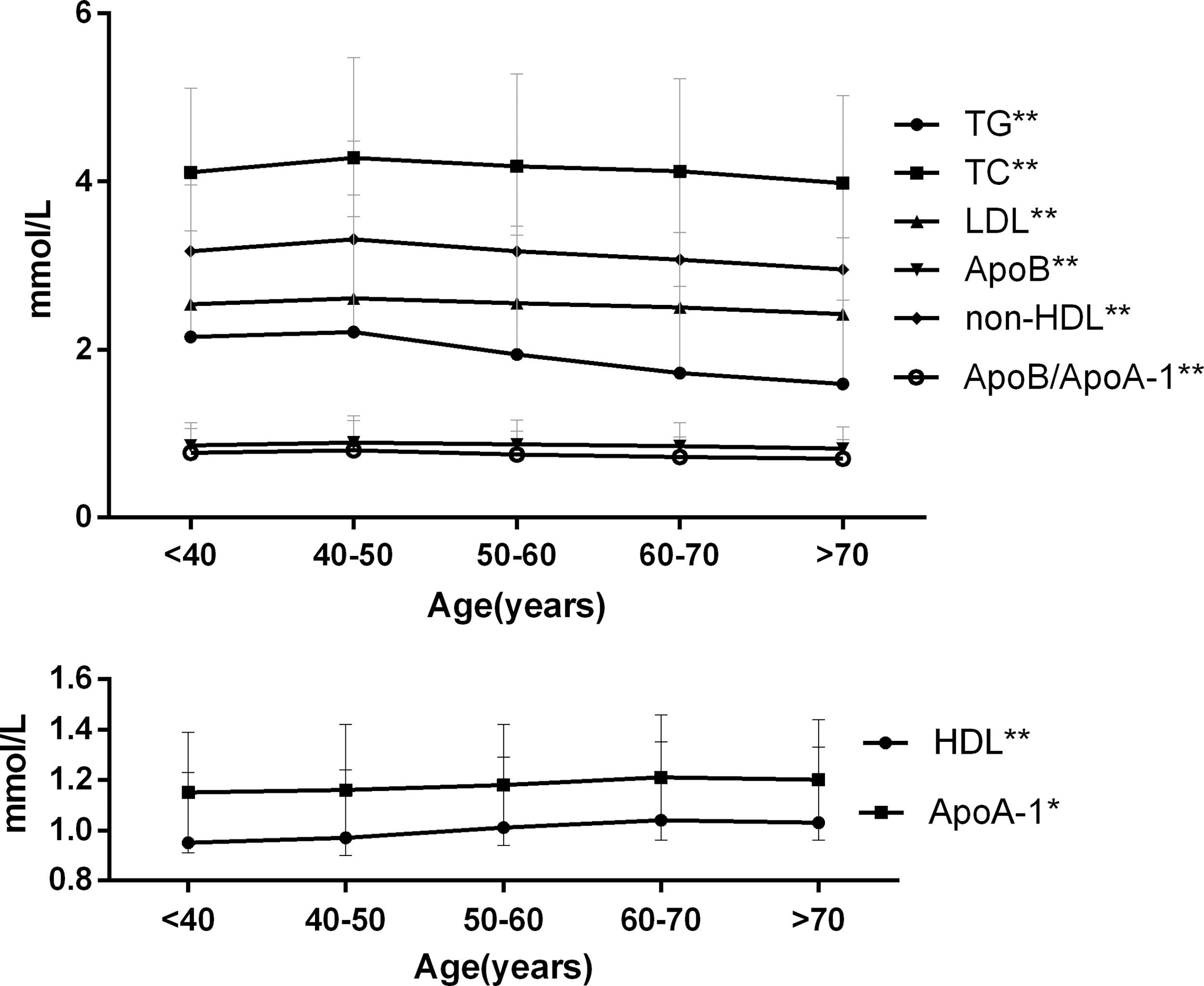
Relationship between serum lipid concentration (mM) and age (years) in all subjects.
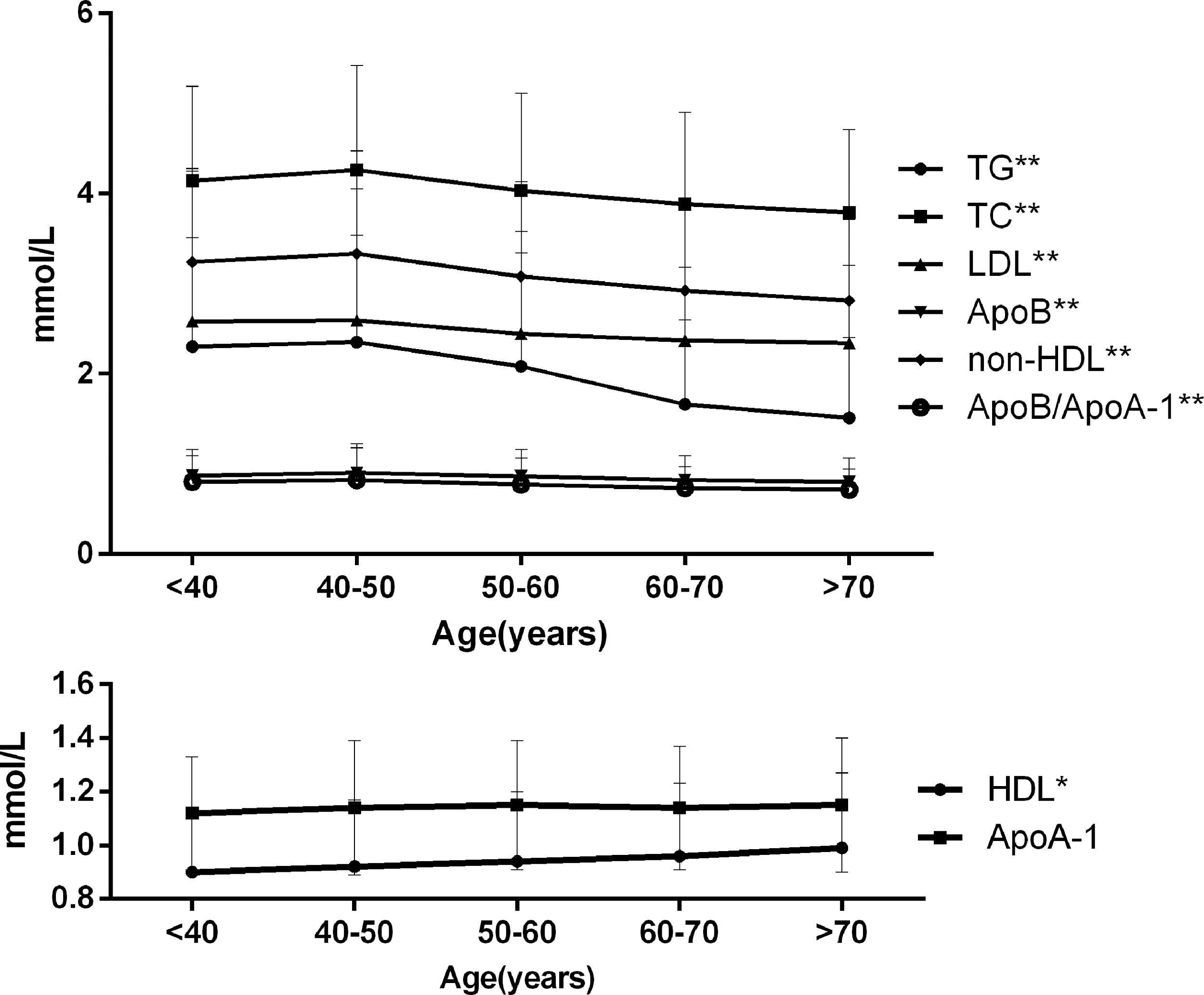
Relationship between serum lipid concentration (mM) and age (years) in males.
Relationship between serum lipid concentration (mM) and age (years) in females.
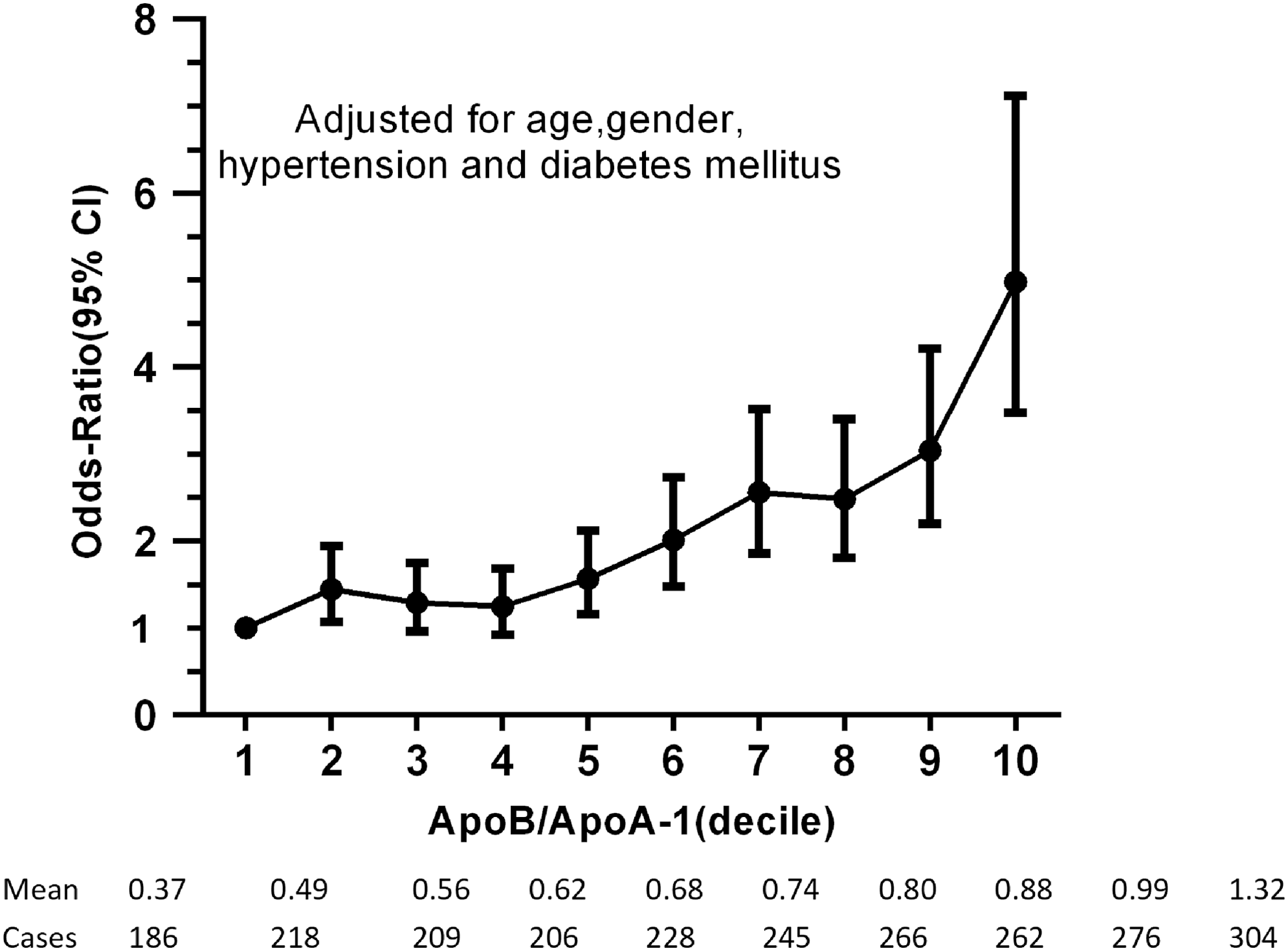
Odds ratio for CAD in men and women pooled together in relation to the apoB/apoA-1 ratio expressed in deciles (log plot).
Clinical Characteristics in Participant in Both Genders
All CAD cases versus all controls; males CAD cases versus male controls; females CAD cases versus female controls. ** P < 0.0001.
apoB, apolipoprotein B; apoA-1, apolipoprotein A-1; BMI, body mass index; CAD, coronary artery disease; DM, diabetes mellitus; EH, essential hypertension; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; NS, not significant; TC, total cholesterol; TG, triglyceride.
Lipid and Apolipoprotein Concentrations by Age
Cholesterol and Apolipoprotein Concentrations by Age for Coronary Artery Disease Cases
Cases versus controls ** P < 0.001,* P < 0.05.
Cholesterol and Apolipoprotein Concentrations by Age for Controls
Multivariate Logistics Regression Analysis
Adjustment risk factors, including age, smoking, hypertension, and diabetes.
CI, confidence interval; OR, odds ratio.
Discussion
In this study, we evaluated the effects of the TC, TG, LDL-C, HDL-C, non-HDL-C, apoA-1, and apoB levels and apoB/apoA-1 ratio on the risk of CAD at different ages and by gender. We found that all of the lipid parameters were significantly associated with CAD risk and blood lipids showed different peaks between male and female subjects, as most lipid profiles were higher in women than in men, and some of the lipid profiles decreased gradually with age. After adjusting for common cardiovascular risk factors, the apoB/apoA-1 ratio was still shown to be a strong, new risk factor for CAD, which is expected since the risk of CAD significantly increased with increasing apoB/apoA-1 ratio.
The variation in cholesterol lipoprotein lipids in this study is contrary to some previous studies. A significant, direct correlation between age and cholesterol levels was identified in a meta-analysis. 17 Five cross-sectional studies performed in middle-socioeconomic status urban locations in India showed that the age- and sex-adjusted trends showed significant increases in TC, TC, and HDL-C. 18 A study based on the same population insisted that there was a significant increase in TC, LDL-C, non-HDL-C, and TG with age, but that HDL-C decreased slightly with age. 19 However, declining trends in lipid levels observed in this analysis were similar to data from the INTERHEART study, which contained more than 25,000 myocardial infarction individuals at different ages. 20 Zhong et al. analyzed 1382 patients with a first acute myocardial infarction and indicated that dyslipidemia was more prevalent in the nonelderly than the elderly. 21 Because cardiovascular risk, and therefore the incidence of cardiovascular events, increases so profoundly after 60 years of age, cardiovascular disease is thought to be a disease of older age groups. However, a previous study suggested that half of all cardiovascular events in men and one-third in women occur before 65 years of age. 22 Forty- and 50-year olds quantitatively account for an important fraction of the total number of events. Given that the population at risk in these age groups is large and that the 10-year risk is low for the majority of individuals, a higher emphasis on the causes of vascular disease must be placed on those individuals who are younger. Until now, despite age being the principal determinant of risk, except for those with markedly elevated levels of LDL-C or diabetes, lipid-lowering interventions have become common only after reaching 60 years of age. 23 Therefore, it is necessary for the nonelderly to accept lipid-lowering therapy and choose more effective lipid-lowering drugs. These findings add to this argument by demonstrating that the lipid risk factors were greater in the younger subjects than the older individuals.
There were also significant differences in CAD risk between males and females. In previously published studies, differences in atherogenic profile, in terms of both gender and menopausal status, were suggested. 24 –27 Gupta et al. developed a hospital database, which included 67,395 subjects, and observed greater hypercholesterolemia and lower HDL-C in women. A lower decline was observed in women. 28 Similar to previous results, we found that the peak serum lipid levels in female and male subjects were different for different age ranges. In our study, the peak serum lipid level in male patients was observed mainly in those between 40 and 50 years of age, while in females, it was observed mainly in those between 50 and 60 years of age. The average age of the females we enrolled was greater compared with the males, at which point the male lipid level had begun to decline. In addition, in the health records, we found that some patients did not take medicine regularly despite having a clear diagnosis of hypertension or hyperlipidemia. Therefore, we classified these subjects as being unmedicated. Most subjects used statins as lipid-lowering drugs, and fish oil was not used by any of them. In both the CAD patients and controls, we found that the rate of previous drug lipid-lowering treatment use was lower. We also found that the lipid-lowering treatment rate of males was higher compared with females. Therefore, there may be some other reasons why the women in this study showed elevated lipid profiles compared to men. One possible explanation for this observation may be that the women were less likely to undergo drug treatment. Lower rates of treatment utilization have been reported in women compared to men. Another possible explanation is that therapeutic targets are harder to attain for women because they have a worse cardiovascular risk profile than the risk profile of men. The effects of androgens and estrogens on lipoprotein concentrations have dominated the evaluation of the hypothesis that differences in sex hormones underlie the sex difference in lipoprotein concentrations and CHD incidence. Sex steroids play a pivotal role in regulating body composition in both men and women, and some of their precursors have been shown to have several biological effects, such as dehydroepiandrosterone sulfate, a precursor of androgens, which is gender related and varies during the life. DHEAS has been shown to affect lipid metabolism and is closely related to the occurrence of cardiovascular diseases. However, the relevance in assessing the roles of sex hormones in CHD is doubtful, and it was not performed with sufficient rigor to provide definitive conclusions. These reasons described above may affect the lipid levels that were produced in our results.
At present, according to the newest guidelines of management of CVD risk, the primary criterion was to initiate lipid-lowering therapy to reduce subsequent risk for CVD. 29 In our study, we found apoB/apoA-1 to be a strong risk factor for CAD. At present, it has been demonstrated that apoB and/or apoA-1 are risk factors for CVD. 30 –32 Some of these trials are briefly commented upon, and several advantages for measuring apoB and apoA-1 were found. By using internationally standardized and validated techniques, they can be measured directly, 33 and they reflect the two sides of the risk equation. The ratio of apoB to apoA-1 is a simple way to reflect the balance of cholesterol transportation. The higher the value of the apoB/apoA-1 ratio and the more cholesterol circulating in the plasma are likely to lead to cholesterol becoming deposited in arterial walls, provoking atherogenesis and inducing a higher risk for CV events. 13,34 –36 On the other hand, the effect of lipid-lowering therapy targeting the apoB/apoA-1 ratio also has been verified. 12,34 This verification affirmed that the apoB/apoA-1 ratio could be a simple, robust, and precise indicator of risk with great value for health screening and lipid-lowering therapy. In addition, Fig. 1 seems to show that all of the other lipid parameters, except for potentially the TG level, with overlapping error bars for the CAD patients and controls. indicate high risk as well. In clinical practice, it is commonly recommended that patients reduce TG by diet control, but when necessary, better drugs and ezeomab can be administered appropriately to regulate high TG levels. However, when we reviewed these patient records, we found that patients rarely took these drugs. In addition, people in Xinjiang prefer a high-fat diet, which may be the reason why the error bars of TG did not overlap. Through multifactor Cox regression analysis, we found that the apoB/apoA-1 ratio had the largest OR value, and TG had an OR value just less than it. We also believe that the TG level is a powerful risk factor for CAD, as previous studies have clarified that an elevated TG level is a strong marker of cardiovascular disease risk. Increased TG levels lead to increased levels of small-density lipoproteins, which ultimately lead to increased cardiovascular risk. 37,38
In conclusion, our findings may show differences in outcomes. This study has some limitations. We used a hospital-based case–control study population with individuals who were undergoing CAG examination; thus, this population does not represent the general population, and the results cannot be extrapolated and generalized to all populations. Some other factors, such as differences in culture, race, diet, lifestyle, demographic characteristics, laboratory tests, different diet, lifestyle factors, and metabolic status, could also have affected the lipid values. Because of the retrospective nature of this article, data from some factors like diet and lifestyle factors were not recorded. The limited number of female participants included in this study was a limitation as well since the mean age of women in the case group was higher compared with women in the control group. As the proportion of postmenopausal women in the study was very small, we did not consider menopausal status. No female subjects received hormone replacement therapy. However, the duration of menopause and sex hormone levels were not further recorded. Larger community-based and well-designed studies on this topic should be carried out in the future. However, despite the limitations of this study, our results highlight significant age- and sex-related differences in secular trends in cholesterol-related lipoproteins.
Footnotes
Acknowledgment
This work was supported by the National Natural Science Foundation of China (U1603381).
Author Disclosure Statement
No conflicting financial interests exist.