
Abstract
Background:
Overweight and obesity are more common in men than in women. This explains the higher prevalence of risk factors for metabolic syndrome (MetS) found in men. We aimed to assess whether gender, per se, might be an independent risk factor for the components of MetS in a large cohort of subjects within the normal range of body mass index (BMI).
Materials and Methods:
Cross-sectional analysis was carried out on 9976 men and women, aged 18 to 70 years, with a BMI between 18.5 and 25.0 kg/m2 attending a screening center in Israel between the years 2000 and 2014.
Results:
Mean (SD) age of the study sample was 43.3 (9.6) years, 54.5% were men. Prevalence of MetS components in men and women was hypertension 5.3% and 3.0%, impaired fasting glucose (IFG) 18.1% and 7.9%, diabetes mellitus (DM) 2.4% and 1.3%, high triglyceride levels 17.7% and 9.4%, and low high-density lipoprotein (HDL) cholesterol levels 13.6% and 17.0%, respectively, P < 0.001 for all. Increased waist circumference was <1% in both genders. Multivariate analysis showed male gender to be an independent risk factor for IFG [odds ratio (OR) 2.43, 95% confidence interval (CI) 2.12–2.79], hypertriglyceridemia (OR 1.86, 95% CI 1.63–2.12), DM (OR 1.80, 95% CI 1.29–2.50), and hypertension (OR 1.46, 95% CI 1.16–1.83) but not for low HDL levels (OR 0.59, 95% CI 0.52–0.67).
Conclusion:
This study, on a cross-sectional sample of subjects with a normal BMI, showed male gender to be an independent risk factor for all components of the MetS, apart from the low HDL risk factor that was found to be higher in women.
Introduction
A
To see whether gender, per se, might be an independent risk factor for the components of MetS, we decided to assess the prevalence all components of MetS, in a large cohort of subjects with a body mass index (BMI) within the normal range, thus neutralizing the effect of overweight and obesity.
Materials and Methods
Study population
The study population consisted of a cross-sectional sample of all men and nonpregnant women aged 18–70 years, who were referred by their employers for a routine medical screen, at a tertiary medical center in Israel between the years 2000 and 2014. None of the subjects was hospitalized at the time of screening. The screen in each case consisted of a thorough medical history evaluation and complete physical examination. This was accompanied by a broad series of blood and urine tests, chest X-ray, electrocardiogram, exercise stress test, respiratory function test, and full ophthalmology examination. As subjects may return once a year for a repeat investigation, data from each subject's most recent visit were used in this study.
Blood tests
After an overnight 12-hour fast, serum glucose levels, triglyceride, and HDL cholesterol were measured. Normal serum glucose level was defined as serum levels <100 mg/dL; impaired fasting glucose (IFG) as 100–125 mg/dL; and DM as serum levels ≥126 mg/dL and/or a known diagnosis of DM treated with medication. 5 Subjects with glucose serum levels of 100–125 mg/dL who had been treated for DM were included in the DM group. Hypertriglyceridemia was defined by either triglyceride levels ≥150 mg/dL or by a personal history of hypertriglyceridemia treated with medication. Low level of HDL was defined as HDL <40 mg/dL in men and <50 mg/dL in women. 6
Blood pressure measurements
Blood pressure measurements were performed with the subject in the sitting position. The width of the sphygmomanometer cuff was in accordance to the subject's arm dimension.
Hypertension was defined as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg or self-reported hypertension treated with medication.
BMI and WC
BMI between ≥18.5 and ≤25.0 kg/m2 was defined as normal. Increased waist circumference (WC) was defined as ≥102 cm in men and ≥88 cm in women.
Smoking habits
Data on participants' smoking habits were collected by direct questioning on the day of examination in the screening center. The questionnaire included the following questions: Do you smoke? Yes/no. If so, how many cigarettes do you smoke per day, and for how many years? (To calculate the number of pack years). Have you smoked in the past? Since when have you stopped smoking?
A computer program was created to transfer data from each visit into a spreadsheet Excel file.
The study was approved by the Helsinki Ethics Committee of Rabin Medical Center, Israel.
Statistical methods
Descriptive statistics were used to describe the distribution of the components of the MetS within the genders. Analytic statistical methods were then implemented. A t-test was used for continuous variables that followed the normal distribution, whereas the Mann–Whitney U test was implemented if the variable's distribution could not be considered normal. Chi-square test was used for dichotomous variables. Bivariate analysis was carried out to yield the unadjusted odds ratio (OR) for gender within each category of the MetS. Thereafter, a multivariate analysis was implemented using logistic regression models adjusting for gender (with women as the reference group) and for other possible interfering factors; this included the possible confounding effect of the components of the MetS on each tested component. The increased WC definition used was the common one defined by the National Cholesterol Education Program Adult Treatment Panel III, 6 that is, WC ≥102 cm in men and ≥88 cm in women. A supplemental analysis was performed to assess the increased WC prevalence data using the European criteria, that is, WC ≥94 cm for men and ≥80 cm for women.
A sensitivity analysis was carried out by the exclusion of individuals younger than 55 years, evaluating the effect of gender among the older population, where women are postmenopausal.
For all analyses, a P value of <5% was considered significant. Analyses were carried out using IBM SPSS version 19.
Results
The total number of subjects who attended the screening center between 2000 and 2014 was 26,722. The number of subjects with a normal range BMI was 9976, of which 54.5% were men. This group was defined as the study cohort. The clinical and laboratory characteristics of these participants are presented in Table 1. No significant differences between men and women were found as to age and smoking habits. Increased WC was found to be <1% in both genders (3 men and 26 women). Compared with women, men had a higher prevalence of hypertension (5.3% vs. 3.0%), IFG (18.1% vs. 7.9%), DM (2.4% vs. 1.3%), hypertriglyceridemia (17.7% vs. 9.4%); however, the prevalence of low HDL was lower in men (13.6% vs. 17.0%) (P < 0.001 for all) (Fig. 1).
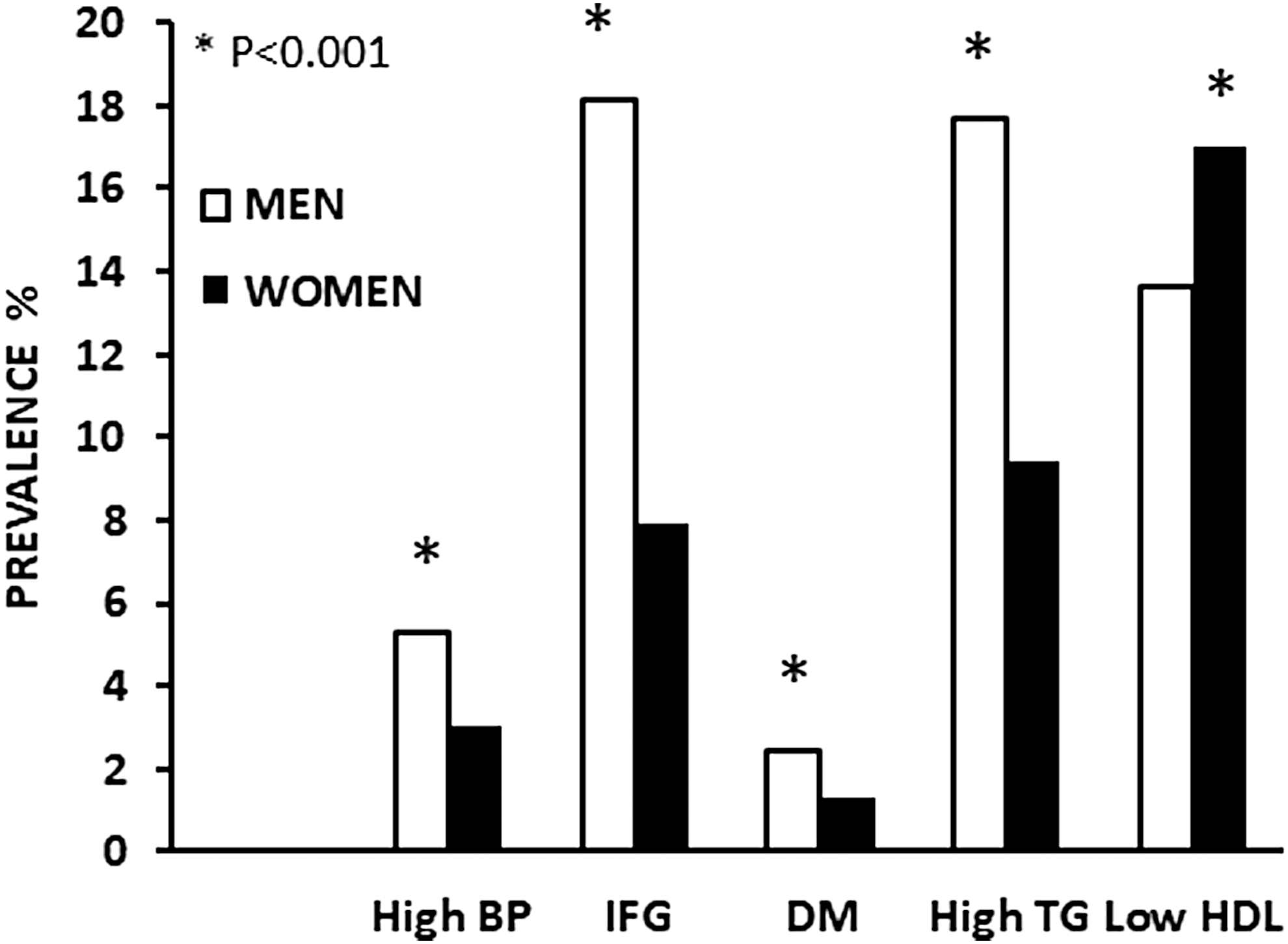
Prevalence (%) of metabolic syndrome components in subjects with a normal body mass index. BP, blood pressure; DM, diabetes mellitus; HDL, high-density lipoprotein; IFG, impaired fasting glucose; TG, triglycerides.
Patients Characteristics by Gender
Calculated using t-test for continuous variables and chi square test for categorical variables.
Total 9627 cases, due to missing data.
Lower than 40 mg/dL for men; lower than 50 mg/dL for women.
BMI, body mass index; BP, blood pressure; LDL, low-density lipoprotein; HDL, high-density lipoprotein.
Multivariate analysis revealed male gender to be an independent risk factor for IFG [OR 2.43, 95% confidence interval (CI) 2.12–2.79), hypertriglyceridemia (OR 1.86, 95% CI 1.63–2.12), DM (OR 1.80, 95% CI 1.29–2.50), and hypertension (OR 1.46, 95% CI 1.16–1.83) but not for low HDL levels (OR 0.59, 95% CI 0.52–0.67) (Table 2).
Male Gender as a Determining Factor for the Components of the Metabolic Syndrome, Among Individuals Within the Normal Range of Body Mass Index
Odds ratios with adjustments using logistic regression models.
Sensitivity analysis: men and women aged 55 years or older were included, N = 1436.
Adjusted for age, BMI, smoking status, DM, IFG, hypertriglyceridemia, and low HDL.
Adjusted for age, BMI, smoking status, hypertension, hypertriglyceridemia, and low HDL.
Adjusted for age, BMI, smoking status, hypertension, DM, IFG, and low HDL.
Adjusted for age, BMI, smoking status, hypertension, DM, IFG, and hypertriglyceridemia.
CI, confidence interval; DM, diabetes mellitus; IFG, impaired fasting glucose; OR, odds ratio.
To adjust for a potential protective effect of estrogen on the cardiovascular system, we reanalyzed our data in a subgroup of subjects, age range 55 to 70, assuming all women in this group to be in menopause. The multivariate analysis on this age group revealed a lower OR of the male gender as a determinant risk factor for components of MetS than the OR results of the whole cohort. This was found to be apparent for IFG (OR 1.93, 95% CI 1.49–2.49), hypertriglyceridemia (OR 1.48, 95% CI 1.10–1.99), and hypertension (OR 1.31, 95% CI 0.95–1.81). However, the OR of the male gender as a determinant risk factor for DM was found to be higher in this age group (OR 3.20, 95% CI 1.89–5.41). As for low HDL levels, in this subgroup, the OR was similar to that of women (OR 0.78, 95% CI 0.55–1.08) (Table 2).
The supplemental analysis using the European criteria revealed 105 (2.7%) men and 347 (11.0%) women with increased WC (P < 0.001). The unadjusted OR (95% CI) of the male gender as a determining factor for increased WC was 0.22 (0.18–0.28). When adjusted for age, BMI, smoking status, hypertension, DM, IFG, hypertriglyceridemia, and low HDL, the OR (95% CI) was 0.10 (0.08–0.13).
Discussion
MetS is defined as a group of cardiovascular risk factors that result from insulin resistance. These include hyperglycemia, dyslipidemia, hypertension, and central adiposity. 7 Currently there are three definitions of MetS 6,8,9 (Table 3). MetS may precede overt DM and can also be related to the development and prognosis of cardiovascular disease. 10,11 Gender differences exist as to the prevalence of MetS. In regard to the non-Hispanic white population, a recent survey found the prevalence of MetS to be 23.7% and 21.8% in men and women, respectively. 1 It should be noted that obesity and overweight are more common in men 1 and this may affect the prevalence of MetS components. Indeed, obesity has been associated with an increased risk for hypertension, 2 type 2 DM, 3 and dyslipidemia. 4 The question that arises is whether, after adjusting for the effect of obesity, these gender differences persist. This was the goal of our study and indeed we found significant differences between men and women with normal BMI levels. Apart from low levels of HDL, which were more common in women, all other components of MetS were found to be to the advantage of women. With regard to HDL levels, there are two different aspects. The first is the average HDL levels, which are indeed higher in women. The second aspect is the percentage of low HDL levels that is lower in women. It should be noted that the definition of low HDL between men and women differs, that is, in men the definition is a level <40 mg/dL, and in women a level <50 mg/dL. This stricter definition in women accounts for the higher average of low HDL levels found in women.
The Current Three Definitions of the Metabolic Syndrome
Increased WC in Mediterranean populations is defined as ≥94 cm for men and ≥80 cm for women.
IDF, International Diabetes Federation; NCEP ATP III, National Cholesterol Education Program Adult Treatment Panel III; WC, waist circumference.
Multivariate analysis revealed male gender to be an independent risk factor for hypertriglyceridemia, DM, and hypertension.
The definition of increased WC used in our study was WC ≥102 cm for men and ≥88 cm for women. This is the common clinical practice definition used in the National Cholesterol Education Program Adult Treatment Panel III. 6 So, as the cohort was based on subjects with a normal BMI, it was not surprising to find that the prevalence of increased WC in our study was <1% for both genders. Other MetS definitions 8,9 define increased WC as ethnicity specific. That is, different ethnic groups have a specific WC definition. For Middle East population, it is suggested that European data are used until more specific data are available. The European definition of increased WC is ≥94 cm for men and ≥80 cm for women. Using the European definition, we reanalyzed the WC data and found the prevalence of increased WC in men and women to be 2.7% and 11.0%, respectively (P < 0.001). The unadjusted OR (95% CI) of the male gender as a determining factor for increased WC was 0.22 (0.18–0.28). When adjusted for age, BMI, smoking status, hypertension, DM, IFG, hypertriglyceridemia, and low HDL, the OR became 0.10 (0.08–0.13). Indeed, if this is the case, men in our cohort with a normal BMI had a lower prevalence of increased levels of WC than women of the same cohort. Despite that, men still showed a higher prevalence of hypertriglyceridemia, DM, and hypertension. This endorses the possibility of gender per se as a risk factor for those MetS components. As increased WC is correlated with a high prevalence of low HDL, 4 this may explain why women in our cohort had a higher prevalence of low HDL than men.
There are a few possible explanations as to gender differences in MetS, as well as their role in cardiovascular disease. 12 The pattern of lipid accumulation in women and men differs. In general, women have more peripheral adipose tissue, with gluteal fat accumulation, whereas men have more central or android obesity. 13 It is possible that this reduced tendency to accumulate fat within the intra-abdominal sites might be one of the primary metabolic differences underlying the reduced risk in women of cardiovascular disease, MetS, and DM. 13
In men, visceral fat is also associated with hypertension and insulin resistance. 14 In addition, women exhibit low salt sensitivity in their blood pressure regulation before menopause and become increasingly salt sensitive after menopause. 15 Moreover, it is possible that the renin angiotensin system (RAS) may be regulated differently in men and women, with endogenous estrogen suppressing angiotensin receptor type 1 expression and angiotensinogen synthesis. 16 Gender-specific activation of the RAS may play a role in the postmenopausal increase in hypertension in women. Estrogen has a protective effect on the cardiovascular system. In a review by Mendelsohn et al., some possible protective mechanisms were suggested. 17 Estrogens exert both a direct and an indirect effect on the vascular system. The direct effect acts rapidly and causes vasodilatation by activating nitric oxide synthase in endothelial cells. This also has a long-term effect by influencing gene expression. These genomic effects cause an increase in the expression of genes with important vasodilatory enzymes, such as prostacyclin synthase and endothelial nitric oxide synthase. Estrogen may also accelerate endothelial cell growth and replacement after vascular injury. Indirectly, estrogen has an influence on serum lipid concentrations. Most of these effects involve receptor-mediated effects on hepatic genes such as Apo- protein genes. The result is an increase in serum HDL cholesterol, a decrease in low-density lipoprotein (LDL), and an increase in triglyceride serum levels.
Since estrogen plays an important role in cardiovascular protection, we decided to reanalyze our data in a subgroup of subjects, aged 55 to 70 years, assuming women to already be in menopause (Table 2). Indeed, the OR for all components of MetS apart from DM moved toward the null compared with the OR of the entire study cohort. The existing OR, although smaller, suggests that the estrogen element may not be the only reason for the female advantage as to the prevalence of the MetS components.
The main strength of the study is the inclusion of a large cohort—∼10,000 men and women with complete data sets of clinical and laboratory findings. Nevertheless, our study has its limitations. The study group was not drawn from a population sample but from those attending an examination center. This limits the generalizability of the findings. In addition, the cross-sectional design precludes conclusions regarding causality. Moreover, sedentarity is an important component associated with MetS components. We did not have these data in regard to our cohort. Lastly, the use of BMI for assessing obesity is limited, but this was the best way that we could eliminate the effect of obesity on the risk factors of MetS.
Assessment of gender as a risk factor for the components of MetS in men and women without obesity has not been performed directly. Such data were presented indirectly in a study by St-Onge et al. 18 In their study of a cohort of normal weight Americans, they divided the normal range of BMI into four subgroups: 18.5–20.9, 21.0–22.9, 23.0–24.9, and 25.0–26.9 kg/m2 and showed that as BMI increased within the normal range, the prevalence of the risk factors for MetS also increased. It could be seen indirectly from their results that compared with women, men had a higher prevalence of all risk factors for MetS, apart from low HDL levels that were higher in women. These finding are exactly in accordance with our results.
During the past decades, the burden of the MetS gained attention as its prevalence increased dramatically. It is well established that men are prone to the MetS and their excessive morbidity and mortality are related to it. However, this study provides evidence that even among individuals within the normal BMI, men are at increased risk for most health conditions comprising the MetS. This implies a mechanism inherent to gender itself. The fact that the advantage of women diminishes as they go into menopause suggests the role of hormonal signaling networks.
In summary, in this large cohort of subjects with normal BMI, we show male gender to be an independent risk factor for all components of MetS, apart from low levels of HDL. This advantage appears to be partially attenuated when women go into menopause.
Authors' Contributions
All authors contributed to the study design. E.C. interpreted the results of analyses, prepared figures and tables, and drafted the article. I.M. performed the statistical analysis. E.C. and I.K edited and revised the article. E.C., I.M., E.G., and I.K., approved the final version of the article.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.