
Abstract
Background:
Glycated hemoglobin (HbA1c) is an index of the average blood glucose level over the preceding 2–3 months. In experimental studies, the lens responded to changes in osmolarity by forming vacuoles. By observing the vacuoles of the lens during eye examination, can we detect changes in osmolarity and glycemia over the last 6 months through HbA1c levels?
Methods:
In total, 400 patients (mean age, 67.7 ± 9.8 years), including those with diabetes mellitus, hypertension, and heart failure, were included in the study. The control group contained 70 patients matched in terms of age and sex and who had no prior disease (mean age, 67.8 ± 9.4 years). Monthly Na, glucose, and blood urea nitrogen values were used to calculate changes in osmolarity over 6 months. HbA1c values were also recorded. Biomicroscopy was used to evaluate lens vacuolation; all vacuoles were digitally photographed and converted to ImageJ format.
Results:
The sensitivity and specificity of using large vacuoles to detect HbA1c ≥10% were 88.0% (95% confidence interval [CI]: 68.8–97.4) and 82.6% (95% CI: 74.1–89.2), respectively. The sensitivity and specificity of detecting a 10 mOsm/kg change in osmolarity were 61% (95% CI: 48.9–72.4) and 94.5% (95% CI: 91.5–96.7), respectively.
Conclusions:
Lens vacuoles, which can be observed with a simple and quick examination, can be used to detect HbA1c levels and osmolarity changes over the last 6 months. Because of their relationship to the severity of retinopathy, vacuoles can also be used as a weak control indicator.
Introduction
T
The lens of the eye surrounded by aquoeus humor is a perfect environment for examining osmolarity change because it is transparent and easily observable. Glucose, salts, water, oxygen, carbon dioxide, and metabolic wastes readily pass through the lens capsule to the cortex and nucleus. 4 Minimal lens swelling triggers hydropic changes in lens epithelial cells and fibers, but excessive swelling causes fluid accumulation in the interfibrillar field. In experimental studies, the lens responded to changes in osmolarity by forming vacuoles and has been described as a “perfect osmometer”. 5 Vacuoles are open, spherical fluid-filled spaces, usually located in the lens cortex. Their diameters range from ∼10 μm to 1.3 mm. 6
Systemic hyperosmolality often induces thirst and vasopressin release from osmosensing neurons in the lamina terminalis and hypothalamus of the forebrain. In response, water reabsorption from the collecting ducts of the kidney is controlled by aquaporins 2. Central osmoregulatory processes are associated with the sympathetic nervous system. 7 As intracellular space constitutes about two-thirds of the bodily volume, changes in water homeostasis significantly affect cells. 8 Peripheral osmoreceptors sense local osmolarities in various tissues. 9,10 Vacuoles, water clefts, and spokes are often the precursors of cortical cataracts; most are of osmotic origin. 11 “Osmotic nephrosis,” a reaction to ingestion of hyperosmolar materials, features vacuolization and swelling of renal proximal tubular cells. 12
Approximately 30% of DM patients have heart failure (HF). 13 Type 2 diabetes was detected in 40% of patients hospitalized with low ejection fraction. 14 In patients with HF, the prolonged activation of various neurohumoral mechanisms can increase sodium levels and fluid retention. 15 In patients with HF, acute stroke, acute coronary syndrome, and other critical illnesses, changes in osmolarity are associated with mortality. 16,17 Therefore, from a prognostic viewpoint, it is important to explore whether patients are experiencing changes in osmolarity.
In this study, we investigated for the first time whether lens vacuoles can be used to detect changes in glycemia and osmolarity over a 6-month period in patients with DM, hypertension (HT), and HF, who are frequently exposed to osmolarity changes.
Methods
Data source and study population
A total of 2550 patients diagnosed with HT, DM, and HF (with low or normal ejection fractions) were screened. Four hundred patients aged 40–90 years who underwent 6-month laboratory tests for the following reasons were admitted to the study.
Diabetic patients for the purpose of monthly sugar control for oral antidiabetic or/and insulin dose adjustment. HT patients, due to blood pressure control charts follow-up, due to the side effect of blood pressure drugs, and due to coexistent latent diabetes follow-up. In patients with HF, in addition to these, monthly laboratory test had requested to follow the metabolic and renal side effects of diuretics. In addition, there were patients who had monthly laboratory tests on their own request.
Glucose, Na +, and blood urea nitrogen (BUN) levels were recorded monthly. We enrolled 70 similarly aged healthy individuals without HT, diabetes, or HF as controls. Demographic data were recorded. HbA1c levels, which were measured twice in the last 6 months; the use of insulin and diuretics was recorded.
Lens examination
After application of a mydriatic agent, all subjects underwent biomicroscopic (İnami L-0240, Japan) examinations. Pupil diameter was measured using the light-width function of the biomicroscope. Under retroillumination, all lenses were digitally photographed using a smartphone. With reference to biomicroscopic pupil measurement, vacuole and pupil diameters were measured with the aid of ImageJ software (NIH, Bethesda, MD). Individuals with the presence of an apparent vacuole (ø ≥ 80 μm) that could easily be seen by eye were considered “vacuole positive”. A cutoff of 300 μm was used to separate small and big vacuoles; cases with both types of vacuoles were considered to have big vacuoles.
Osmolarity was calculated as (2[Na+] + [glucose]/18 + [BUN]/2.8). 18 Osmolarity change was taken as absolute change, positive or negative. Retinopathy was investigated using ophthalmoscopy.
The study followed all relevant tenets of the Declaration of Helsinki. The study protocol was approved by our ethics committee. Written informed consent was obtained from each subject.
Statistical analysis
Data analysis was performed using IBM SPSS Statistics version 17.0 software (IBM Corporation, Armonk, NY). The assumptions of the distribution of normality and homogeneity of variances were evaluated by Kolmogorov–Smirnov and Levene tests, respectively. Descriptive statistics for continuous variables was expressed as mean ± SD or median (minimum–maximum), where applicable. Number of cases and (%) were used for categorical data. While the mean differences between groups were compared by Student's t-test, otherwise, Mann–Whitney U test was used for the comparisons of not normally distributed data. When the number of independent groups was more than two, either one-way ANOVA or Kruskal–Wallis test was performed. Since the P values from one-way ANOVA or Kruskal–Wallis test statistics were statistically significant, post hoc Tukey HSD or Conover's multiple comparison test was used to know which group differs from which others. Categorical data were analyzed by Pearson's chi-squared, Likelihood ratio, or Fisher's exact test, where appropriate. Determining the best predictor(s) which effect on vacuole existence was evaluated by multiple logistic regression analysis Backward LR method. Any variable whose univariable test had a P value <0.25 was accepted as a candidate for the multivariable model along with all variables of known clinical importance. Whether the differences between case and control groups in terms of the mean of osmolarity levels were carrying on or not was evaluated by multiple linear regression analysis after adjustment for age. Sensitivity, specificity, positive, and negative predicted values of clinical characteristics (e.g., existence of vacuole and size of vacuole) for determining the severity of HbA1c, osmolarity levels, and differences in osmolarity levels were also calculated. A P value less than 0.05 was considered as statistically significant.
Results
Baseline characteristics
The mean age of the patients was 67.7 ± 9.8 years and that of the controls was 67.8 ± 9.4 years. The sex ratio was 50% in both groups. Patients were divided into three subgroups: those with DM, HT, and HF.
In the patient group, of the patients with small vacuoles (n = 110), 8 (7.2%) had only DM, 48 (43.6%) had only HT, and 53 (48.1%) had both DM and HT. Among patients with large vacuoles (n = 62), 41 (66.1%) had only DM, 13 (20.9%) had only HT, and 38 (61.2%) had both DM and HT.
Of all vacuoles, 78% were in the posterior capsule, 12% in the anterior cortex, 8% at the equator, and 2% in the nucleus. Vacuole diameters ranged from 80 to 600 μm. Intraobserver, interobserver intraclass correlation coefficient was 0.92 (confidence interval [CI]: 0.90–0.94) and 0.90 (CI: 0.88–0.92), respectively. Vacuole samples are shown in Fig. 1.
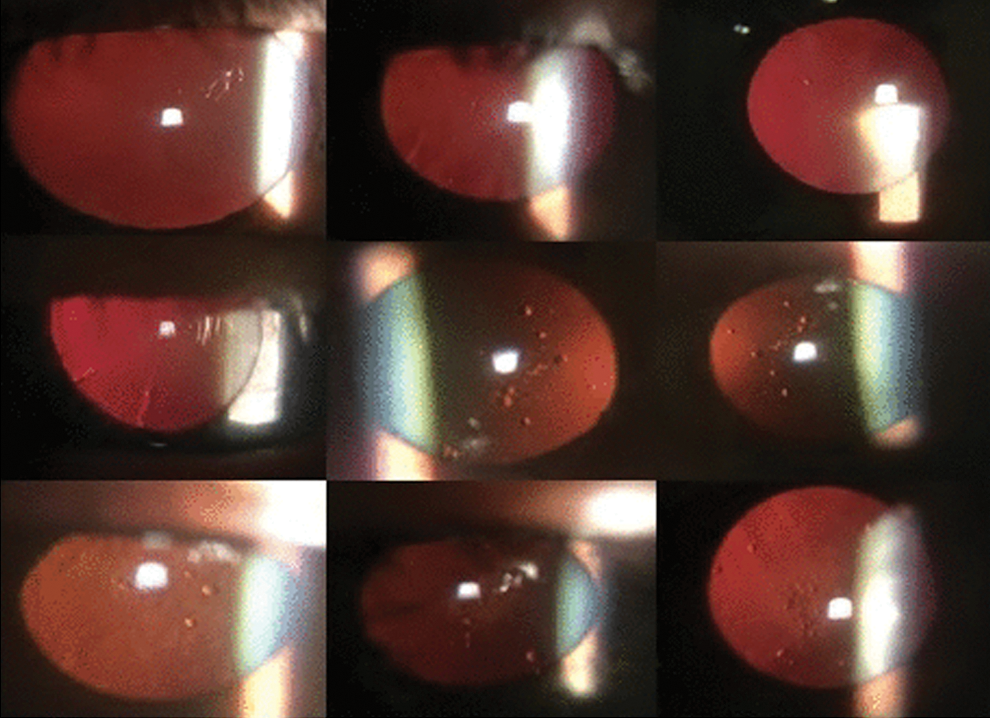
Examples of small and large vacuoles—Top row: small vacuoles middle row: small and large vacuoles bottom row: vacuoles may be associated with retrodots, cortical+ subcapsular cataract, and subcapsular cataract. Color images available online at
Of the entire patient group, 350 (87.5%) patients exhibited no diabetic retinopathy, 44 (11.0%) patients exhibited background retinopathy, and 6 (1.5%) patients exhibited proliferative retinopathy. There were no cases of hypertensive retinopathy in 302 (75.5%) patients. Grade 1 retinopathy was present in 43 (10.8%) patients, grade 2 retinopathy in 51 (12.8%) patients, and grade 3 retinopathy in 4(1.0%) patients. Retrodots were present in 20 patients (5.0%) and one-eye pseudophakia in 70 patients (17.5%). The demographic and clinical characteristics of all subjects are shown in Table 1.
Demographic and Clinical Characteristics of Patient and Control Groups
Student's t-test.
Pearson's chi-squared test.
BUN, blood urea nitrogen; DM, diabetes mellitus; HbA1c, glycated hemoglobin; HF, heart failure; PTE, pretibial edema.
In the patient group, the osmolarity change over 6 months ranged from 1 to 30 mOsm/kg.
When patients with small and large vacuoles were compared to those without vacuoles, and when those with large and small vacuoles were compared, the changes in osmolarity differed significantly (P < 0.001 and P < 0.001, respectively). The average osmolarity of those with DM was significantly higher than that in other patients (P < 0.001). Patients with DM exhibited greater osmolarity changes than the other patients over the 6-month period (P < 0.001). The findings are summarized in Table 2.
Osmolarity Levels According to the Clinical Features of Patients and the Changes in Osmolarity Over 6 Months
One-way ANOVA.
Student's t-test.
The difference between no vacuole and small vacuole groups was found to be statistically significant (P < 0.001).
The difference between no vacuole and big vacuole groups was found to be statistically significant (P < 0.001).
The difference between small vacuole and big vacuole groups was found to be statistically significant (P < 0.001).
The median fasting blood sugar levels of patients with small and large vacuoles were higher than those of patients with no vacuoles (P = 0.015 and P < 0.001, respectively). The median BUN level of patients with big vacuoles was higher compared with those with small and no vacuoles (P < 0.001 and P < 0.001, respectively). The demographic and clinical features of the patients with and without vacuoles are shown in Table 3.
Demographic and Clinical Characteristics of Patients With and Without Vacuoles
Student's t-test.
Pearson's chi-squared test.
Mann–Whitney U test.
Likelihood ratio test.
Regression analysis of factors that may affect lens vacuole formation
In the patients, the frequencies of both small and large vacuoles, and the average osmolarity, were significantly higher than in controls (P = 0.004, P < 0.001, and P < 0.001, respectively). On multivariate logistic regression, the probability of vacuolation in the patient group was 5.615-fold higher (95% CI: 2.603–12.111 fold) than that in the control group after adjustment for age (P < 0.001).
We performed univariate statistical analysis and entered all variables with P values <0.25 into a multivariate logistic regression model. The most significant contributors to the formation of vacuoles were body mass index, HbA1c, and HT. The multivariate logistic regression analysis of all possible factors that might affect vacuolation in patients is shown in Table 4.
The Co-Effects of All Possible Risk Factors Predictive of the Presence of Vacuoles in Patients Using Multivariate Logistic Regression Analysis with Backward Elimination
CI, confidence interval; OR, odds ratio.
HbA1c level and lens vacuoles
The HbA1c level was significantly higher in patients with small or large vacuoles compared to those with no vacuoles (P < 0.001 and P < 0.001, respectively). In the patient group, both small and large vacuoles significantly detected HbA1c levels above 7% and 10% (P < 0.001 and P < 0.001, respectively). In addition, the HbA1c level of those with large vacuoles was significantly higher (P < 0.001) compared with those with small vacuoles (Table 1).
When DM and non-DM patients were compared, the median sodium level was lower (P = 0.006) in DM patients. In patients with similar sodium levels, the glucose level was not significantly associated with the presence of small vacuoles (odds ratio [OR] = 1.004, 95% CI: 1.000–1.008, P = 0.062).
However, in patients with similar sodium levels, each 50-U increase in the glucose level significantly increased the probability of large vacuoles, by 1.481 fold (95% CI: 1.179–1.862 fold, P < 0.001).
The diagnostic performance of vacuoles in terms of HbA1c levels ≥7%, ≥7% and ≤9%, and ≥10% is summarized in Tables 5 and 6.
The Diagnostic Performance of All, Small, and Large Vacuoles in Terms of HbA1c Levels ≥7%, 7%–9%, and ≥10%
Data in bold indicate the sensitivity of detecting vacuoles due to HbA1c levels among age groups.
NPV, negative predictive value; PPV, positive predictive value; LV, large vacuole; SV, small vacuole; V+, vacuole +.
Within Each Age Group, the Vacuole Diagnostic Performance Indicators Were Used to Distinguish Among HbA1c Levels Below 7%, Those Between 7% and 9%, and Those Above 10%, Respectively
Data in bold indicate the sensitivity of detecting vacuoles due to HbA1c levels among age groups.
PPV, NPV, the statistics within parenthesis indicates lower and upper limits of 95% confidence intervals.
According to Bonferroni corrections, the effects of vacuole presence were considered statistically significant at P < 0.0056, and the effects of small and large vacuoles were considered statistically significant at P < 0.0028.
NPV, negative predictive value; PPV, positive predictive value; LV, large vacuole; SV, small vacuole; V+, vacuole +.
Performance diagnostics of lens vacuoles for determining changes in osmolarity
To determine the osmolarity changes ≥5 mOsm/kg over the preceding 6 months, the vacuole sensitivity was 72.1% (95% CI: 65.3–78.2) and the specificity was 85.2% (95% CI: 79.6–89.8). Large vacuole sensitivity was 93.1% (95% CI: 84.5–97.7), and specificity was 68.0% (95% CI: 62.6–73.0).
For osmolarity changes greater than 10 mOsm/kg, the vacuole sensitivity was 31.5% (95% CI: 25.1–38.5), and the specificity was 100% (95% CI: 98.2–100.0). Large vacuole sensitivity was 61.1% (95% CI: 48.9–72.4), and specificity was 94.5% (95% CI: 91.5–96.7).
The positive detection of osmolarity greater than 295 mOsm/kg was 55.8% sensitivity (95% CI: 46.5–64.9) and 62.5% specificity (95% CI: 56.5–68.2) for vacuoles, and it was 27.5% sensitivity (95% CI: 19.7–36.4) and 89.6% specificity (95% CI: 85.5–91.9) for large vacuoles.
Discussion
In diabetics, hyperglycemia activates the lens pentose phosphate pathway and sorbitol formation and triggers ion influx by creating osmotic and oxidative stress. Activation of the KCC and chloride channel triggers uncontrolled cell swelling.
19
In an experiment in diabetic rabbits, in cases of hyperglycemia, with glucose levels above 300 mg/dL, serum and aqueous glucose levels increased together, hyperosmolarity developed, small vacuoles and opacities formed, and both sodium and calcium levels increased in the lens.
20
Significant vacuole formation was observed in canine lenses incubated for up to 96 hr in growth medium supplemented with 30 mM
DM can be associated with both hypo- and hypernatremia. Hypernatremia and hyperosmolarity can occur in both insulin-mediated glucose metabolism and in glucagon-dependent glucose release weakness. 23 In our study, 51% of patients had DM, and the mean osmolarity and osmolarity change were greater in diabetes patients than in those without diabetes (Table 2). In a survey, thirst and vasopressin release osmolarity thresholds were found to be elevated in patients with poorly controlled DM (HbA1c >9%) compared with those in patients with well-controlled DM (HbA1c <7%) and patients without diabetes. 3
Most studies have established that the aqueous humor Na+ level is similar to its plasma level, and glucose and urea levels are ∼80% of their plasma levels. 24 The osmolarities of the lens and aqueous humor are controlled to ensure normal metabolism and transparency. 4 In the rabbit lens, an osmolarity of 185 mOsm is associated with 45% of the theoretical maximum swelling; at 375 mOsm, the shrinkage is 47%. 25 As is true of all animal cells, the lens initially swells in a hypoosmotic environment followed by a regulatory volume decrease. In hyperosmotic medium, initial shrinkage is followed by a regulatory volume increase. 26 A similar situation exists in brain cells, but the brain responds within minutes. 27
Water movement in AQPs (aquaporins, water channel proteins) is driven by osmotic gradients. 28 AQP0 (a major intrinsic protein) is active only in the lens posterior pole and nuclear fibers. 29 AQP1 is present in anterior lens epithelial cells, vascular endothelia, and fibroblasts; it is released by hyperosmotic agents, such as glucose, sucrose, sorbitol, urea, and sodium chloride. 30 Vanilloid 4 (TRPV4) channels are involved in the hypoosmotic response, 31 and the absence of AQP5 has been shown to cause osmotic swelling under hyperglycemic conditions. 32
In one study of human lenses, the positive relationship between aqueous glucose and lens sodium was weaker in diabetics than nondiabetics. The osmotic stressors that occur in the lenses of diabetic patients differ from those that occur in nondiabetics. 33
In our study, there was no significant effect of DM duration on the presence of vacuoles. Insulin usage was statistically higher in the group in which vacuoles were detected. The sodium-retention effects of insulin during hyperglycemia may be due to the preservation of the sodium balance in uncontrolled type II diabeties. 34 Age-related changes in glucose, Na+, and Ca+ permeability occur on the lens membrane. 35,36 The protective mechanisms of the lens vacuole formation deteriorated above HbA1c >10; as HbA1c changed, the sensitivity of vacuole detection increased and the effect of aging decreased (Tables 5 and 6).
In those with primary HT, increased NKCC1 activity in vascular smooth muscle cells and osmoregulatory neurons of the paraventricular nucleus increases the peripheral resistance of the systemic circulation and activates the central nervous system. 37 In the obese, total water intake, urine osmolality, and hypohydration were more prevalent. 38 Mediators of obesity (tumor necrosis factor-α, interleukin-1β, insulin, and, to a lesser degree, leptin) attenuated the TRPV4-mediated effects. 39
In our study, 38% of patients with HF had DM. Serum sodium levels, and by extension plasma osmolarity, are affected principally by water and not sodium homeostasis. On postdischarge follow-up of HF with reduced ejection fraction patients, low osmolarity (≤284 mOsm/kg) was associated with more mortality than normal (285–300 mOsm/kg) and high (≥300 mOsm/kg) osmolarity. 40 In these patients, large vacuoles may reflect unbalanced fluid intake.
Evaluation of dehydration by reference to osmolarity remains controversial. However, a value of 300 mOsm/kg is indicative of dehydration. A figure in the range 295–300 mOsm/kg indicates incipient dehydration. 41 –43 In those with acute coronary syndrome, a median osmolarity of 291 mOsm/kg was associated with more mortality than a median level of 281 mOsm/kg. 44 In 16,598 intensive care patients, osmolarity >300 mmol/L was found to be significantly associated with mortality, 45 as was a value >296 mOsm/kg in patients with acute stroke (OR 2.4, 95% CI: 1.0–5.9). 46 In our study, the large vacuoles detected an osmolarity of 295 mOsm/kg over the 6-month period with a specificity of 89.6% (95% CI: 85.5–91.9).
A few studies with an insufficient number of patients reported that the vacuoles may disappear, change, or increase over a few months of follow-up. 47 –49 According to our clinical observations, in cases in which hyperglycemia and hyponatremia coexist in diabetes patients (e.g., diabetic ketoacidosis), and in cases in which hyponatremia is attributable to diuretic use in HF, if these two situations are corrected, the osmolarity may change markedly with the development of vacuoles.
In the control group without DM or HT, 11.4% of subjects had small vacuoles, and no big vacuoles were found. While 66.1% of the patients with large vacuoles had DM, only 7.2% of the patients with small vacuoles had DM, suggesting that glucose may be more effective in the formation of large vacuoles.
Because of its relation to the severity of retinopathy, vacuole can be used as a weak control indicator. Large vacuoles may be particularly useful for people who are not aware of their diabetes.
Study limitations
It is difficult to measure the precise extent and duration of daily or weekly osmolarity changes. Due to easy visual selectability, a diameter limit of 80 μm was preferred. No similar cutoff was found in the literature. Because the number of patients with HbA1c between 6.5% and 7% was not significant, members of this group were not enrolled in the study.
Conclusions
The sensitivity and specificity of using large vacuoles to detect HbA1c ≥10% were 88.0% (95% CI: 68.8–97.4) and 82.6% (95% CI: 74.1–89.2), respectively. The sensitivity and specificity of detecting a 10 mOsm/kg change in osmolarity were 61% (95% CI: 48.9–72.4) and 94.5% (95% CI: 91.5–96.7), respectively. For more precise results, studies with larger sample sizes are needed.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.