
Abstract
Background:
Compared to studies evaluating the effect of environmental factors on weight and health, relationships between housing types and health conditions are understudied. This study aimed to assess the relationship between housing types and metabolic and weight phenotypes using data from the 2014 to 2015 Korea National Health and Nutrition Examination Survey.
Methods:
A total of 9586 Korean adults (4128 men and 5458 women; mean age, 50.7 ± 16.5 years) were considered for this study. Four metabolic and weight phenotypes were created using presence/absence of metabolic syndrome and body mass index (<25 kg/m2 for normal weight vs. ≥25 kg/m2 for overweight).
Results:
Nonapartment residents were 1.23-fold (95% confidence interval: 1.07–1.42) more likely to have metabolically unhealthy and overweight phenotype compared to apartment residents, after adjusting for sociodemographic characteristics, residence area, health behaviors, and nutritional information awareness. In a subgroup analysis, nonapartment living was associated with higher odds for the metabolically unhealthy and overweight phenotype than living in an apartment in individuals with the following characteristics: age <60 years, education ≥ college, second–third quartile income level, married, living in urban area, alcohol <16 drinks/week, noncurrent smokers, and aware of nutritional information.
Conclusions:
Housing types may be an indicator for increased risk of metabolic and weight phenotypes in Korean adults and used to select high risk individuals. Uncontrolled confounding factors related to housing types, including property assets and environmental attributes, may contribute to the findings.
Introduction
Different combinations of presence or absence of metabolic syndrome and weight status have different effects on the risk of cardiovascular disease and mortality. Compared to metabolic healthy with normal-weight individuals, metabolic healthy with overweight, metabolic unhealthy with normal-weight, or metabolic unhealthy with overweight individuals had an increased risk for incident cardiovascular disease, cardiovascular disease-related mortality, or all-cause mortality. 1,2 Particularly, metabolic unhealthy with overweight individuals were at the highest risk for those outcomes. 1 Although genetic factors may contribute to the dysregulation of metabolic components and weight, 3 an increase in the prevalence of unhealthy metabolic and weight phenotypes suggests that personal behavior and neighborhood factors may significantly affect these conditions. 4
The relationship between the level of neighborhood deprivation and increased risk of cardiovascular diseases has been well established. 5,6 Evidence for the relationship of the risk of cardiovascular disease and characteristics of living environment suggests that this relationship is caused by factors such as residential density, recreational facilities, walkability of environment, traffic density, road proximity, and fast food environment. 7 Likewise, other studies suggest associations of metabolic syndrome and obesity with residents' perceptions of the local residential environment and neighborhood walkability; metabolic syndrome was inversely associated with greater infrastructure for walking 8 and obesity was inversely associated with desirable neighborhood walkability. 9
Besides neighborhood environment, home environment, such as housing type, may also be an important determinant of metabolic and weight phenotypes. Suboptimal housing type may be a measure of the underlying low socioeconomic status and linked to an undesirable home environment, household crowding, and exposure to adverse environmental conditions. 10,11 A small number of studies reported that suboptimal housing condition and type were related to incident diabetes 11 and short sleep duration. 10
More than half of the population in Korea lives in apartments. Given the evidence for higher risk for mental illness in individuals living in high-rises than those in low-rises and houses, 12 and higher risk for cardiovascular disease in residents living at higher floor levels of residential tall buildings compared with residents living at lower floor levels, 13 apartment-living in Korea may be the optimal or suboptimal home environment for high/low cardiovascular risk. Nevertheless, there have been no studies on the association between housing types (apartment vs. nonapartment) and metabolic and weight phenotypes.
Therefore, the purpose of this study was to assess the relationship between housing types (apartment vs. nonapartment) and the metabolic and weight phenotypes using data from the 2014 to 2015 Korea National Health and Nutrition Examination Survey (KNHANES).
Materials and Methods
Study population
The KNHANES 2014–2015 was a cross-sectional, nationally representative survey of individuals from the noninstitutionalized civilian population of Korea. A rolling sampling design was applied to involve a complex, stratified multistage probability cluster survey. 14 This survey was performed at mobile examination centers by trained medical staff and interviewers. Among 11,921 adults, 19–80 years of age, this study included 9586 participants (4128 men and 5458 women; mean age, 50.7 ± 16.5 years) with data for housing type, residential area, sociodemographic characteristics (age, sex, educational levels, marital status, and income), anthropometric measurements (weight, height, and waist circumference), and components of metabolic syndrome.
Written informed consent was obtained from all the participants. The KNHANES met the guidelines laid down in the Declaration of Helsinki, and the Institutional Review Board (IRB) of the Korean Center for Disease Control and Prevention approved all procedures involving human subjects (The IRB number was 2013-12EXP-03-5C). The IRB at Busan Paik Hospital Inje University provided a waiver from IRB review for the use of publicly available data.
Metabolic and weight phenotypes, housing types, and confounding factors
Measurements of components of metabolic syndrome were done in each participant after >8 hr of fasting. Blood samples were analyzed in a central laboratory certified by the Korean Ministry of Health and Welfare. Fasting plasma glucose (FPG), triglyceride (TG), and high-density lipoprotein (HDL) cholesterol concentrations were measured using an automatic analyzer (Automatic Chemistry Analyzer 7600; Hitachi, Tokyo, Japan). Blood pressure (BP) was assessed manually, using a standard mercury sphygmomanometer.
Waist circumference (WC) was measured at the narrowest point between the lower rib margin and the iliac crest. The definition of metabolic syndrome was adapted from the harmonized definition, which requires that three of the following five components should be present.: WC >90 cm in men or >80 cm in women; BP ≥130/85 mmHg or a history of hypertension; FPG concentration ≥5.6 mmol/L or a history of diabetes; HDL concentration <1.03 mmol/L for men or <1.29 mmol/L for women; and TG concentration ≥1.63 mmol/L. 15
Body mass index was calculated as measured weight (kg)/measured height (m) 2 , and the weight status was dichotomized as a body mass index <25 kg/m 2 for normal weight versus ≥25 kg/m 2 for overweight. 16 Using combination of metabolic and weight status categories, four metabolic and weight phenotypes were created: without metabolic syndrome and normal weight (phenotype I), without metabolic syndrome and overweight (phenotype II), with metabolic syndrome and normal weight (phenotype III), and with metabolic syndrome and overweight (phenotype IV).
The assessment of housing types and potential confounding factors was based on self-reported questionnaires. Housing types were dichotomized into apartment versus nonapartment (townhouse, multiplex house, and independent house). The potential confounding factors were age (19–39 years, 40–59 years, or ≥60 years), sex, educational attainment (graduated elementary school, graduated middle school, graduated high school, or graduated college or higher level), income level (quartiles of individual income), residential area (urban vs. rural), smoking status (nonsmoker, ex-smoker, or current smoker), alcohol consumption (nondrinker, <4 drinks/week, 4–16 drinks/week, and >16 drinks/week), regular aerobic physical activity (no vs. yes), walk frequency (0–2 times/week, 3–5 times/week, or >5 times/week), and awareness of nutritional information (yes vs. no). Regular physical activity was defined as engaged in regular, high-intensity exercise for >20 min per session at least thrice per week, as regular, moderate-intensity exercise for >30 min per session at least five times per week, or regular walking for >30 min per session at least five times per week.
Statistical analysis
As the KNHANES is a complex, stratified, multistage, probability-cluster survey and provides specific guidelines for analysis and reporting of sample weights, the stratification and clustering of the design must be incorporated into analyses to ensure appropriate estimates and standard errors to avoid biased estimates and overestimated significance levels. 17 Then, the analyses were conducted as complex sample analyses, except for multinomial logistic regression. Complex sample cross-tabs analysis was used to assess the relationships of metabolic and weight phenotypes with housing types and confounding factors.
Complex sample cross-tabs analysis was used to assess the relationships of housing types with confounding factors. Multinomial logistic regression analysis was performed to test the association of metabolic and weight phenotypes with housing types and confounding factors. Complex sample frequency analysis was conducted to calculate the prevalence of phenotype IV in individuals according to housing types and categories of confounding factors. Subgroup analysis was performed to assess strength of associations between housing types and phenotype IV according to individual confounding factors. Complex sample logistic regression analysis was applied to test the association of phenotype IV (vs. phenotype I) with housing types according to strata of confounding factors after adjusting for other confounding factors, except for the subgroup factor. Data were analyzed using an IBM Statistical Package for the Social Sciences, software version 24 (IBM Corp., Armonk, NY).
Results
In this Korean population-based study, 16.1% of participants had the phenotype IV. The participants with the phenotype IV were more likely to be older, men, married, less educated, have a lower income level, live in a rural area, live in a nonapartment, consume more alcohol, be a current smoker, be engaged in irregular aerobic physical activity, walk less frequently, and be unaware of nutritional information (Table 1).
Distribution of Metabolic and Weight Phenotypes According to Sociodemographic Characteristics and Residence Status and Health Behavior (n = 9586)
Values were number (estimated % ± standard error) of subpopulation.
Nonapartment housing type was townhouse, multiplex house, and independent house.
Using complex sample cross-tabs analysis.
Phenotype I, metabolically healthy and normal weight; phenotype II, metabolically healthy and overweight; phenotype III, metabolically unhealthy and normal weight; phenotype IV, metabolically unhealthy and overweight; PA, physical activity.
The characteristics of participants according to housing types are presented in Table 2. Compared to apartment residents, nonapartment residents were more likely to be older, have a lower educational attainment, have lower income levels, live in an urban area, be nondrinkers or heavy drinkers, be current smokers, walk less frequently, and be unaware of nutritional information.
Distribution of Sociodemographic Characteristics and Health Behavior According to Housing Type (n = 9586)
Nonapartment housing type was townhouse, multiplex house, and independent house.
Values were number (estimated % ± standard error) of subpopulation.
Using complex sample cross-tabs analysis.
Using multinomial logistic regression analysis, nonapartment residents had a 1.23 increased risk of the phenotype IV compared to apartment residents after adjusting for other sociodemographic characteristics and health-related behaviors. In addition, the phenotype IV was associated with older age, lower education level, heavy alcohol consumption, irregular aerobic physical activity, and lower walk frequency (Table 3).
The Associations of Metabolic and Weight Phenotypes with Sociodemographic Characteristics, Residency Status, and Health Behavior
Reference group was individuals with Phenotype I.
Values were odds ratio (95% confidence interval) using multinomial logistic regression analysis.
Phenotype I, metabolically healthy and normal weight; phenotype II, metabolically healthy and overweight; phenotype III, metabolically unhealthy and normal weight; phenotype IV, metabolically unhealthy and overweight.
As shown in Fig. 1, the prevalence of the phenotype IV was consistently higher in nonapartment residents than apartment residents across categories of sociodemographic characteristics and health behavior. In a subgroup analysis after adjusting for other confounding factors, the prevalence of the phenotype IV was higher in nonapartment residents than apartment residents in individuals with the following characteristics: age <60 years, education attainment of college graduation or higher level, second and third quartile income levels, married, living in an urban area, alcohol consumption <16 drinks/week, noncurrent smokers, and awareness of nutritional information (Table 4).
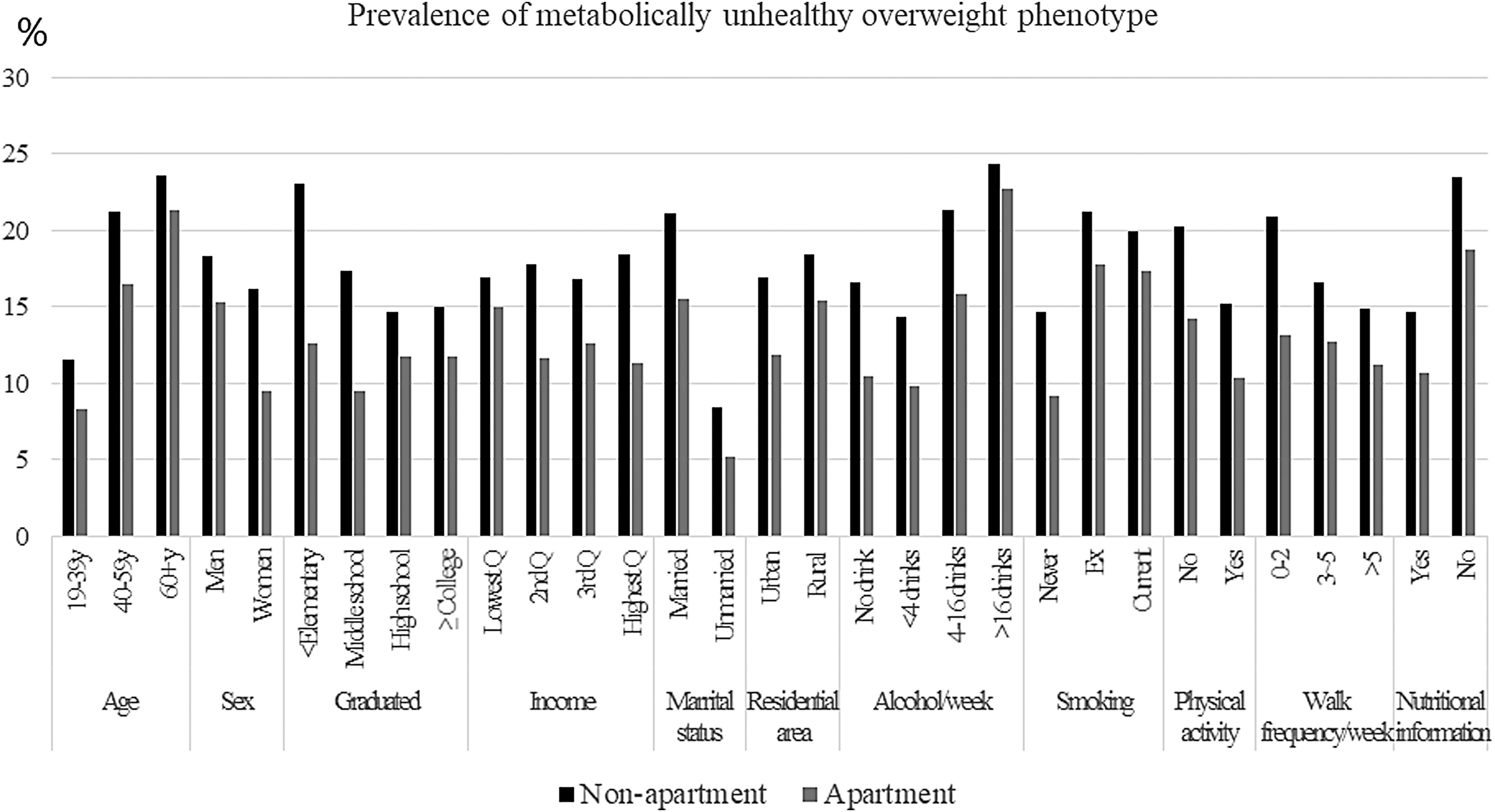
The prevalence of a metabolically unhealthy and overweight phenotype in individuals living in apartments or nonapartments according to sociodemographic and health behavior characteristics.
The Odds Ratio (95% Confidence Interval) for Phenotype IV in Nonapartment Residents According to Subgroups of Sociodemographic Characteristics and Health-Related Behaviors
Bold values represent significant odds ratios and 95% CI.
In nonapartment residents compared to apartment residents after adjusting for other sociodemographic characteristics and health-related behavior using complex sample logistic regression analysis.
Phenotype I, metabolically healthy and normal weight; phenotype IV, metabolically unhealthy and overweight; CI, confidence interval.
Discussion
In this representative Korean population-based study, nonapartment living was associated with an increased risk for the phenotype IV compared to living in an apartment. Although nonapartment residents were more likely to have suboptimal sociodemographic characteristics and health-related behaviors, adjustment for these factors did not affect this finding. More specifically, the risk of having the phenotype IV was increased by 1.23 in participants living in nonapartments, such as a townhouse, multiplex house, and independent house, compared to those living in an apartment after adjusting for age, sex, educational attainment, income level, marital status, residence area, alcohol consumption, smoking status, physical activity, walk frequency, and nutritional information awareness.
This association was observed in individuals with the following characteristics: age <60 years, graduated college or higher level, second and third quartile income, married, living in an urban area, consumed alcohol <16 drinks/week, noncurrent smokers, and aware of nutritional information. Therefore, the observed associations are different by age group, education and income levels, marital status, alcohol consumption level, smoking status, and nutritional information awareness status.
Based on these results, the associations of housing types with metabolic and weight phenotypes appear to be independent of studied sociodemographic characteristics and health-related behaviors. These findings suggest that other mechanisms may play a role and thereby explain these associations. Potential explanations may be house type-related factors, such as home/neighborhood environmental attributes and unassessed personal factors. In previous studies, suboptimal housing conditions were associated with the development of diabetes 11 and living in a house with an appropriate size for the householders and affordability to heat the house was linked to improved health 18
Therefore, housing types may reflect housing conditions. In a recent systematic review, a variety of neighborhood environmental attributes, such as density of fast food restaurants, supermarkets/grocery stores, and walkability of neighborhood environments were associated with body mass index, BP, diabetes, and metabolic syndrome. 7 This might be explained by the fact that housing types reflect neighborhood environmental condition, such as safety and suitability to promote walking and physical activity, accessibility to grocery stores and restaurants to promote better eating, and accessibility to health care systems to better manage metabolic and weight problems.
On the other hand, eating behavior, level of health concerns, frequency of health checkups, and using a health care system are personal factors. Housing types indicate residential property wealth, thereby reflecting the socioeconomic status of participants with those characteristics. Since socioeconomic status has been an established factor associated with metabolic syndrome 19 and obesity, 20 current findings can be explained by economic differences in residents living in apartments or nonapartments.
The economic inequality between nonapartment residents and apartment residents and health inequality according to house conditions in Koreans may support those possibilities. According to the 2017 Korea welfare panel study data, higher number of low-income households were living in nonapartment houses compared to nonlow-income households (68.5% vs. 48.7%). 21 A study using the Korean welfare panel data reveals positive associations of suboptimal residential environmental conditions and lack of proper amenities with self-reported chronic illness and poor health status. 22 Taking these factors into account, the higher risk for the phenotype IV in nonapartment residents may be explained by less optimal home conditions and neighborhood environment, less healthy personal characteristics, and lower economic levels.
Although the proportion of those having phenotype IV was consistently higher in those living in nonapartments across sociodemographic and health behavior characteristics compared to those living in apartments, subgroup analysis showed stronger associations in those with younger age, middle income and highest education levels, married status, better health behavior, and nutritional consciousness, and in urban residents. Probably, the stronger associations in these subgroups may suggest inequality between individuals living in the two housing types regarding economic status and housing and neighborhood environmental conditions, or health-related personal factors may greater in these subgroups. However, the inequality between subgroups should be examined in further studies through assessment of housing conditions, neighborhood environmental attributes, detailed health-related personal characteristics, and indicators of property.
To our knowledge, this study is the first to assess the association of housing types with metabolic and weight phenotypes. In addition, this study population represented Korean adults; therefore, it is not likely that selection bias would influence these findings. Nevertheless, several limitations of this study should be considered. The property assets value of apartments versus nonapartments may differ across countries. For example, socioeconomic status of apartment residents by floor level was different across countries. 13 Thus, generalization of these findings to other countries may not be appropriate, although generalization to Koreans is possible.
In addition, this cross-sectional study did not ascertain causal relationships. Finally, there are no relevant studies to explain underlying mechanism of this finding regarding differences in environmental attributes such as available playground, green space, and infrastructure for health improvement between apartments and nonapartments in Korea. Then, it is hard to judge what are more important with respect to improving physical housing conditions, social environment of the house, or physical environmental conditions to mitigate higher prevalence of metabolically unhealthy and overweight phenotypes found in this study. Based on epidemiological studies for housing and health, both of housing environment and housing conditions would be obviously main settings affecting health. 23
In conclusion, housing types may be an indicator for increased risk of metabolic and weight phenotypes in Korean adults and used to select high risk individuals. Uncontrolled confounding factors related to housing types, including property assets and environmental attributes, may contribute to the findings. Further studies extending the investigation to housing conditions, neighborhood environment, and property factors are needed to determine causal associations between housing types and metabolic and weight phenotypes.
Footnotes
Acknowledgment
This work was funded by the National Research Foundation of Korea Grant funded by the Korean Government (NRF-2017S1A5B8066096).
Author Disclosure Statement
No conflicting financial interests exist.