
Abstract
Background:
Cancer and cardiovascular diseases (CVDs) are leading causes of morbidity and mortality. We analyzed national data to examine the prevalence of CVD risk factors among adult cancer survivors in the United States.
Methods:
Participants included adults ≥18 years of age from the National Health and Nutrition Examination Survey 2001–2002 to 2013–2014. CVD risk factors included hypertension, diabetes, dyslipidemia, obesity, smoking, and physical activity. Prevalence of 1, 2, or ≥3 CVD risk factors was compared between cancer and noncancer participants. All CVD risk factors were adjusted for age and smoking and additionally for sex. Differences in CVD risk factors among cancer and noncancer participants were identified using logistic regression analysis.
Results:
Among 35,379 eligible participants, 2906 (8.4%) had a history of cancer. The proportion of participants having a single CVD risk factor was lower among cancer survivors compared with noncancer participants (25.8% vs. 33.9%, P < 0.001). The proportions of participants having two CVD risk factors (33.5% vs. 24.6%, P < 0.001) and ≥3 CVD risk factors (27.4% vs. 16.4%, P < 0.001) were higher among cancer survivors. However, these associations lost significance upon adjusting for age. The odds of total hypertension (odds ratio [OR] 1.25, 95% confidence interval [CI]: 1.11–1.40) and total diabetes (OR 1.33, 95% CI: 1.08–1.65) were significantly higher among cancer survivors.
Conclusions:
Our study showed that adult cancer survivors in the United States had higher levels of CVD risk factors primarily due to age-related factors, in addition to cancer complications. There is a significant need for improved CVD risk assessment and prevention services for cancer survivors.
Introduction
Cancer and cardiovascular diseases (CVDs) are leading causes of morbidity and mortality worldwide. Approximately 14.1 million new cancer cases were diagnosed in 2012 and projected to increase to 21.7 million by 2030, resulting in 54% increase in global incidence. 1 Global mortality rates due to cancer will also increase by 60% during the same period. 2 Nevertheless, cancer incidence and mortality are declining in the United States. 3 Cancer death rates decreased significantly during the years 1991 to 2015, resulting in overall increase in prevalence of cancer survivors. 3 Moreover, aging population and rising metabolic co-morbidities increase the risk for CVDs in cancer survivors.
Both CVD and cancer pathophysiology involve inflammation and oxidative stress. 4 Metabolic syndrome, an important predisposing factor for CVDs, includes a cluster of co-morbidities such as obesity (principal component), dyslipidemia, hypertension, and diabetes mellitus, which create a pan-systemic inflammatory milieu. 5 Metabolic syndrome is also associated with increased risks for colorectal, hepatic, pancreatic, endometrial, breast, and bladder cancers. 6,7 As survival rates following cancer treatments improve, patients are exposed to a diverse set of physical, emotional, and psychosocial stressors, thus increasing their risks for CVDs. 8 The risk factors associated with CVDs and cancers work in tandem, influencing and increasing the risks for one another. For example, risk factors for CVDs such as diabetes mellitus, hypertension, obesity, and smoking increase the overall risks for cancers. 9 Similarly, cardiotoxic chemotherapies, mediastinal radiotherapy, advancing age, and increasing survival rates progressively increase the risk for CVDs in cancer survivors. 10 Thus, cancer survivors should be regularly monitored for CVD risk factors to decrease additional morbidity and mortality associated with CVDs in these patients. However, studies that looked for CVD risk factors among cancer patients are scarce. Therefore, we analyzed National Health and Nutrition Examination Survey (NHANES) data from 2001 through 2014 to examine the prevalence of CVD risk factors among adult cancer survivors in the United States.
Methods
Study design
We used the NHANES 2001–2002 to 2013–2014 data for our analyses. The NHANES constitutes a nationwide survey of health and nutritional status of the US civilian noninstitutionalized population done by the National Center for Health Statistics (NCHS), Centers for Disease Control and Prevention (CDC). 11 Complex, multistage, cluster sampling probability designs are used for randomly selecting participants for the survey. Data are collected through interviewing participants in their homes as well as through medical examinations and laboratory evaluations conducted in mobile examination centers (MECs). The NCHS institutional review board approved the survey protocol for NHANES data collection.
Study population
For this study, we used data gathered from participants ≥18 years (n = 35,379). All participants who were ≥18 years of age signed written informed consents after a detailed explanation about the interview and data collection procedures. NHANES has developed and published extensive literature on methods and protocols for the questionnaires, laboratory, and examination accessible through its Website. 11
Variables
Demographic variables
Demographic variables such as age, sex, and race/ethnicity; family poverty–income ratio (PIR); and insurance status were used for this study. We categorized age into three categories: 18–44 years; 45–64 years; and 65 years and older. Race/ethnicity was self-reported and included non-Hispanic white, non-Hispanic black, Mexican American, and non-Hispanic other. Family income was assessed by NHANES as a percentage of PIR, calculated by dividing the family's income by established federal poverty levels for the corresponding years. For our study, PIR was divided into four categories, which included <1 (lowest income); 1 to <2; 2 to <4; and ≥4 (highest income). Insurance status included two categories: yes and no.
Cancer survivors
The survey questionnaire included a section for medical conditions, including cancers. Participants who answered yes to the question, “Have you ever been told you have a cancer or malignancy?” were categorized as cancer survivors, while those who answered no were categorized as noncancer participants. Subsequently, participants who answered yes were given a list of 32 cancers to identify their cancer type(s). Previous studies have shown that self-reporting of cancer has high accuracy. 12,13
CVD risk factors
For our study, we used CVD risk factors such as diabetes, hypertension, dyslipidemia, obesity, smoking, and physical activity, which were collected during the NHANES interview and examination.
Diabetes
Fasting blood glucose levels were measured in the morning from randomly selected participants who reported 8–24 hr of fasting. Diabetes status was ascertained only in this subgroup of participants (n = 15,624). Total diabetes included participants with self-reports of diabetes diagnosed by a health care professional, glycated hemoglobin (HbA1c) level ≥6.5%, or fasting blood glucose level ≥126 mg/dL. 14 Undiagnosed diabetes included participants not self-reporting a diabetes diagnosis by a health care professional, but having an HbA1c level ≥6.5% or fasting blood glucose level ≥126 mg/dL.
Hypertension
Blood pressure (BP) measurements were done in MECs using standardized protocols. A total of three measurements were collected by a physician with 5 min of rest in between the readings. These three measurements were averaged for our analysis. Participants who self-reported using antihypertensive medications or whose systolic BP measurements were ≥140 mmHg or diastolic BP measurements were ≥90 mmHg were considered hypertensive. Untreated hypertension included participants lacking self-reports of using antihypertensive medications, but having systolic BP measurements ≥140 mmHg or diastolic BP measurements ≥90 mmHg. 15
Dyslipidemia
Total dyslipidemia was defined as self-reports of medication use for lowering cholesterol or non-HDL (high-density lipoprotein) cholesterol ≥160 mg/dL. Non-HDL cholesterol was calculated as total cholesterol minus HDL cholesterol. Among adults with no self-reports of cholesterol-lowering medications, untreated dyslipidemia was defined as non-HDL cholesterol ≥160 mg/dL. 16,17
Obesity
Participants were categorized based on body mass index groups as underweight (<18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2), and obese (≥30 kg/m2).
Smoking
Among participants 20 years and older, self-reported smoking was defined as having smoked at least 100 cigarettes in a lifetime and reports of current smoking. Among participants 18 and 19 years old, self-reported smoking was defined as reports of use of nicotine or tobacco products in the last 5 days. 18 Moderate to heavy smoking exposure was defined based on cotinine levels ≥10 ng/mL regardless of self-reported smoking. 19
Physical activity
Optimum levels of recommended physical activity included 150 min of moderate intensity or 75 min of vigorous activity per week. 18
Statistical analyses
Statistical analysis was performed using SAS 9.4 (SAS Institute, Cary, NC), which accounted for the complex survey design of NHEANS through adjustments made by weights, strata, and clusters. Demographic characteristics and prevalence of CVD risk factors were compared between cancer survivors and noncancer participants. We also estimated the proportion of untreated or undiagnosed risk factors among patients with CVD risk factors. In addition, we calculated and compared the prevalence of 1, 2, or ≥3 CVD risk factors among cancer survivors and noncancer participants. We used self-reported smoking as a CVD risk factor because there were no differences between self-reported smoking and moderate to heavy smoking exposure based on cotinine. We adjusted for age for all CVD risk factors, whereas for smoking, we adjusted for both age and sex when calculating estimates. In the final analyses, we investigated differences in cardiovascular risk factors among cancer survivors versus noncancer participants using logistic regression analysis while adjusting for covariates such as age, sex, race/ethnicity, education, and family PIR. We reported weighted prevalence, standard errors (SEs), odds ratios (ORs), and confidence intervals (CIs). Statistical significance was set at P < 0.05, and CIs were estimated with 95% certainty.
Results
Demographic characteristics
This study included data from 35,379 participants, of which 2906 (8.4%) were having cancers. The mean (SE) age of the sample was 45.4 (0.20) years and 50.9% of participants were in the age group 18–44 years, 35.9% were in the age group 45–64 years, and 14.3% were in the age group 65 years and older (Table 1). About 47.5% of participants were men, 68.5% were non-Hispanic white, 11.4% were non-Hispanic black, 8.4% were Mexican American, and 11.7% were other non-Hispanics. About 14.2% of participants were below national poverty levels and 19.6% did not have any form of health insurance.
Demographic Characteristics of Participants by Cancer Diagnosis, National Health and Nutrition Examination Survey 2001–2002 Through 2013–2014 (n = 35,379)
P < 0.001.
FPIR, family poverty–income ratio; SE, standard error.
CVD risk factors among cancer survivors
Nonage-adjusted estimates showed that the proportions of participants with CVD risk factors such as hypertension (P < 0.001), diabetes (P < 0.001), and dyslipidemia (P < 0.001) were significantly higher among cancer survivors compared with noncancer participants (Table 2). Similarly, the proportion of participants who did not follow recommended levels of physical activity was significantly higher among cancer survivors compared with noncancer participants (P < 0.001). However, this association lost significance upon adjusting for age. The proportion of participants self-reporting smoking (P < 0.001) and the proportion of participants having moderate to heavy smoking exposure (P < 0.001) were significantly lower among cancer survivors. These associations also lost significance upon adjusting for age and sex. The proportion of participants having obesity did not differ significantly between the two groups.
Prevalence of Cardiovascular Disease Risk Factors in Participants by Cancer Diagnosis, National Health and Nutrition Examination Survey 2001–2013 Through 2009–2014 (n = 35,379)
P < 0.001.
n = 15,624.
Adjusted for both age and sex.
CI, confidence interval.
Figure 1 presents the proportions of adults with untreated hypertension among total hypertension, undiagnosed diabetes among total diabetes, and untreated dyslipidemia among total dyslipidemia cases by cancer diagnosis. The proportion of untreated hypertension among adults with hypertension was significantly lower among cancer survivors (19.6% vs. 28.7%, P < 0.001) when nonage-adjusted estimates were compared. However, the proportion of undiagnosed diabetes among adults with diabetes (25.3% vs. 30.0%, P = 0.189) and proportion of untreated dyslipidemia among adults with dyslipidemia (36.8% vs. 32.4%, P = 0.265) were not significantly different between cancer survivors and noncancer participants. Age-adjusted prevalence of untreated hypertension, undiagnosed diabetes, and untreated dyslipidemia did not show significant differences between cancer survivors and noncancer participants (Fig. 1).
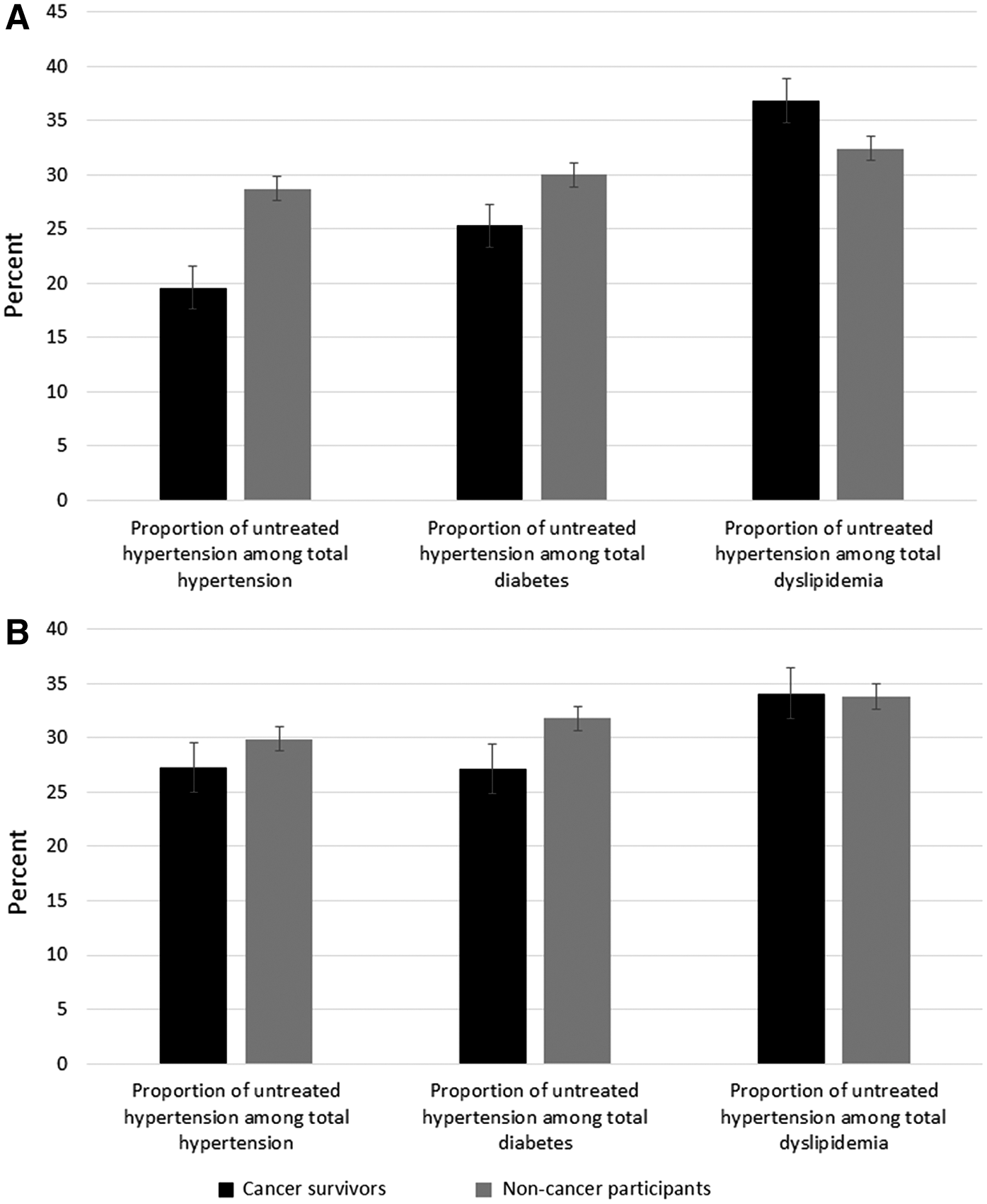
Table 3 shows the proportions of participants having 1, 2, and ≥3 CVD risk factors between cancer survivors and noncancer participants. The proportion of participants having a single CVD risk factor was significantly lower among cancer survivors compared with noncancer participants (25.8% vs. 33.9%, P < 0.001). The proportions of participants having two CVD risk factors (33.5% vs. 24.6%, P < 0.001) and three or more CVD risk factors (27.4% vs. 16.4%, P < 0.001) were significantly higher among cancer survivors. However, these associations lost significance upon adjusting for age.
Prevalence of Number of Cardiovascular Disease Risk Factors in Participants by Cancer Diagnosis, National Health and Nutrition Examination Survey 2001–2002 Through 2013–2014 (n = 35,379)
P < 0.001.
CVD, cardiovascular disease.
Cardiovascular risk factors and cancer survivor status
The odds of total hypertension (OR 1.25, 95% CI: 1.11–1.40) and total diabetes (OR 1.33, 95% CI: 1.08–1.65) were significantly higher among cancer survivors compared with noncancer participants (Table 4). However, other risk factors did not differ significantly between the two groups.
Relationships Between Patient Characteristics and Cardiovascular Disease Risk Factors, National Health and Nutrition Examination Survey 2001–2002 Through 2013–2014 (n = 35,379)
Values highlighted in bold indicate statistically significant results.
Discussion
In this study, CVD risk factors such as hypertension, diabetes, dyslipidemia, and lack of physical activity were more prevalent, whereas self-reported smoking and moderate to heavy smoking exposures were less prevalent among cancer survivors when compared with noncancer participants. However, the prevalence of obesity did not differ significantly between the two groups. We also found that the number of CVD risk factors was significantly higher among cancer survivors. Majority of the cancer survivors were elderly, which additionally complicated existing adverse health conditions among them.
In our study, hypertension was more prevalent among cancer survivors. Similar to our findings, many other studies have reported higher rates of hypertension among cancer survivors. 20 Some studies have reported hypertension prevalence as high as 37% among cancer survivors 21 when compared with 29.0% prevalence in the general population. 22 This observation could probably be explained by the greater number of patients in the age groups 45–64 years and 65 years and older, thereby increasing prevalence of hypertension due to older age, as observed in our study. Prevalence of diabetes was higher among cancer survivors compared with noncancer participants. Our findings are supported by studies that reported that nearly 8%–18% of all cancer patients had pre-existing diabetes. 23 Similar to hypertension, this could be due to the greater number of patients in older age groups and racial distribution with higher diabetes prevalence. 24
We found that cancer survivors had significantly lower levels of physical activity compared with noncancer participants, which could also be explained by higher prevalence of cancer among the elderly. According to the American Cancer Society, nearly 20%–25% of cancers have a direct association with modifiable risk factors such as body weight status and physical inactivity. 25 In our study, smoking levels were estimated using both self-reports and serum cotinine levels. Many studies have shown that self-reports were highly correlated with serum cotinine levels and thus represented general smoking characteristics. 26 In our study, the prevalence of smoking measured by both methods was lower among cancer survivors compared with noncancer participants. Even after adjusting for age and sex, these associations persisted, although not significant. During the recent years, smoking cessation programs have focused on cancer survivors 27 and could be responsible for decreased smoking rates among cancer survivors, in addition to generally lower levels of smoking among the elderly and female US population. 28 Many studies have shown that cancer survivors exhibit greater motivation and resolution to quit smoking when compared with the general population. 29,30 Smoking cessation campaigns by CDC have recommended that greater levels of motivation among cancer survivors should be seized as an opportunity for smoking cessation in this population. 31
Although the rates of untreated hypertension and undiagnosed diabetes appeared to be higher among cancer survivors, it is important to note that total hypertension and total diabetes rates were also higher in this group. Thus, we looked for proportions of untreated hypertension among total hypertension and undiagnosed diabetes among total diabetes cases in both cancer survivors and noncancer participants and found that both these measures were lower in cancer survivors (Fig. 1). Thus, we could infer that cancer survivors were more routinely screened and treated for hypertension and diabetes, as reflected by the lower proportion of untreated and undiagnosed cases observed in this group. However, untreated dyslipidemia was higher among cancer survivors. This could be explained by lower levels of serum lipid screenings compared with hypertension and diabetes due to lack of easier screening tools such as a digital sphygmomanometer and dipstick test for blood sugar levels. However, further studies should focus on these associations to better understand the underlying associations. Irrespective of these findings, it is also worth noting that these associations lost significance after adjusting for age. This showed that awareness about health screenings was not significantly higher among cancer survivors when compared with younger adults or other elderly populations.
Global Burden of Disease, 2010, sponsored by the World Health Organization, identified 25 risk factors contributing to the general burden of diseases, of which hypertension ranked the first, fasting hyperglycemia ranked 7th, physical inactivity ranked 10th, and dyslipidemia ranked 15th. 32 CDC estimates in 2009–2010 showed that nearly 47% of all US adults had at least one uncontrolled CVD risk factor. 33 In comparison, our study found that nearly 86.7% of cancer survivors had at least one CVD risk factor. In addition, 27.4% of all cancer survivors had three or more CVD risk factors. CVD risk factors are substitute measures of disease burden 32 and thus with increasing number of CVD risk factors, there could also be corresponding increase in disease burden among cancer survivors.
We used recent recommendations to define hypertension, diabetes, and dyslipidemia. 14 –17 However, recommendations and guidelines are susceptible to rapid changes within a few years. For example, the Eighth Joint National Committee on High Blood Pressure (JNC 8) in 2014 recommends that treatment should be initiated in patients ≥60 years only if their BP is ≥150/90 mmHg. 34 However, the dataset we used was collected when JNC 7 recommendations were being followed, which recommended that treatment should be initiated only if BP is ≥140/90 mmHg. 15 Thus, we did not consider JNC 8 recommendations because we would have overestimated the number of participants reporting untreated hypertension. Likewise, the Third Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Cholesterol in Adults (ATP III) recommended that total cholesterol should be considered as the primary risk factor and non-HDL cholesterol as a secondary risk factor. However, many recent studies have shown that non-HDL cholesterol levels predicted CVD risk more accurately. 17,35 We did not consider ATP III criteria because we would have inaccurately estimated the number of participants having dyslipidemia. Instead, we used non-HDL cholesterol as the primary risk factor, as recommended by recent evidences. 17,35
One of the main strengths of this study was that we used a nationally representative survey such as NHANES for assessing CVD risk factors among cancer survivors. However, there were some limitations. NHANES does not have data on cancer staging and treatment and hence we could not understand the effects of different cancer stages and treatments on cardiovascular risk factors. NHANES collects data only from noninstitutionalized civilian individuals who were healthy enough to attend MECs and does not include hospitalized or institutionalized individuals. Hence, our findings are not applicable to cancer survivors who are frequently hospitalized or institutionalized.
Our study showed that adult cancer survivors in the United States had significantly higher levels of CVD risk factors, which was primarily due to age-related factors, in addition to cancer complications. There is a significant need for improved CVD risk assessment and prevention services for cancer survivors. Although significant direct evidences that specific interventions could prevent CVDs in cancer survivors are currently lacking, modifying CVD risk factors could be effective as a primary prevention, as observed in many other moderate- to high-risk noncancer populations. 36,37 Cancer survivors constitute a unique patient population who will significantly benefit from primary prevention initiatives because both prevalence of CVDs and contact with health care providers are higher in this population when compared with the general population. 38 Efforts should be directed toward maintaining and improving cardiovascular health, and appropriate interventions should be initiated at the earliest evidence of detectable CVD risk factors. Specialties such as oncology and cardiology and primary care should jointly work on developing and implementing evidence-based guidelines for prevention and control of CVD risk factors. This could significantly improve quality of life as well as survival rates among cancer survivors.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.