
Abstract
The effects of lifestyle interventions (LSIs) on cardiometabolic risk factors in women with polycystic ovary syndrome (PCOS) are controversial. We conducted a systematic review and meta-analysis to assess the effectiveness of LSI on cardiometabolic risk in women with PCOS. We reviewed five databases for randomized controlled trials (RCTs) published between 2012 and December 2016, evaluating the effect of LSI among adult, reproductive age group, overweight, and obese women with PCOS. Outcome measures included weight change, homeostatic model assessment-insulin resistance index (HOMA-IR), total cholesterol (TC), triglyceride (TG), low-density lipoprotein (LDL), and high-density lipoprotein (HDL). A total of 564 studies were screened; 35 full text studies assessed for eligibility, 20 excluded with reasons, 15 included in the systematic review, and 9 studies from 8 RCTs included in a meta-analysis. LSI resulted in significant reduction in weight in sensitivity analyses [study 5 dietary arm as intervention: standardized mean difference (SMD) = −0.81 (95% confidence interval {CI} = −1.24 to −0.39); study 5 combination arm as intervention: SMD = −0.85 (95% CI = −1.26 to −0.45)], HOMA-IR overall [study 5 dietary arm: SMD = −1.46 (95% CI = −2.72 to −0.20); study 5 combination arm SMD = −1.50 (95% CI = −2.76 to −0.23)], and LDL overall [SMD = −1.06 (95% CI = −2.00 to −0.12)]. LSI was more beneficial than Metformin in decreasing LDL [SMD = −2.60 (95% CI = −5.15 to −0.05)] but similar to comparator group in terms of TC, TG, and HDL (P > 0.05). Short-term LSI can effectively improve weight, insulin resistance, and lipid profile and could be recommended as first-line therapy in overweight and obese PCOS women to reduce cardiometabolic risk.
Introduction
Polycystic ovary syndrome (PCOS), a common reproductive endocrinopathy, affects 6%–20% reproductive age women worldwide and 5 million women in the United States. 1,2 Women with PCOS have hyperandrogenism (e.g., hirsutism and acne), menstrual irregularities, reproductive abnormalities (e.g., anovulation and infertility), and metabolic derangements (e.g., insulin resistance and dyslipidemia). 2 They have higher risk for type II diabetes mellitus, hypertension, obesity, and cardiovascular disease. 3,4
Obesity coexists in up to 80% of women with PCOS. 5,6 Hyperinsulinemia, hyperandrogenism, and anovulatory infertility associated with PCOS could be partly attributed to centripetal obesity. 7 In fact obesity aggravates the clinical manifestations of PCOS, including cardiometabolic and reproductive features. 8 It creates a pro-inflammatory environment by increasing cytokine levels and activity, which interfere with insulin action, resulting in compensatory hyperinsulinemia. Obesity also promotes hyperandrogenism through insulin resistance while favoring low-grade chronic inflammation and coagulation disruption, leading to increased cardiovascular risk. 7,9
Primary prevention of cardiovascular disease in women with PCOS is the key. Growing evidence supports cost-effective strategies, including lifestyle interventions (LSIs), in improving cardiometabolic risk in the general population. 10 –12 The American College of Obstetricians and Gynecologists recommends LSI [dietary modifications and/or increased physical activity (PA)] for PCOS women. 4 These interventions show promise in ameliorating PCOS symptoms. 13,14 However, there are mixed results about the role of LSI in cardiometabolic risk reduction in PCOS populations. 15
A 2011 Cochrane review evaluating the impact of LSI in PCOS women was followed by another meta-analysis of studies until 2013. 15,16 Both report inconsistent LSI effects on insulin resistance—a crucial cardiometabolic risk factor. Haqq et al., 15 in 2015 reported no change in insulin resistance or insulin levels, while the Cochrane review demonstrated beneficial effect on insulin levels with LSI. None of the included studies in these meta-analyses compared the effect of different kinds of diet alone. Epidemiological evidence suggests beneficial effects of dietary modification alone on PCOS and associated cardiometabolic risk. 5,17,18 Therefore, we performed a systematic review and meta-analysis to summarize and update the evidence regarding LSI effects, including diet, on cardiometabolic risk among overweight and obese women with PCOS, as obesity is so prevalent in PCOS and worsens PCOS phenotype, as well as cardiovascular disease risk. 7,8
Methods
Data sources
A systematic search was conducted from April 2013 to December 2016. A comprehensive search of following databases was performed: PubMed, Scopus, Embase, Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library), and CINAHL Plus. Following search terms were used: “Polycystic Ovary Syndrome,” “Polycystic Ovarian Syndrome,” “Stein Leventhal Syndrome,” “Stein-Leventhal Syndrome,” “lifestyle intervention,” “lifestyle therapy,” “lifestyle modification,” “lifestyle changes,” “behavioral/behavioural intervention,” “behavioral/behavioural therapy,” “behavioral/behavioural modification,” “behavioral/behavioural changes,” “diet,” “nutrition,” “meal,” “food,” “dietary intervention,” “dietary therapy,” “energy restriction,” “energy reduction,” “calorie restriction,” “calorie reduction,” “hypocaloric diet,” “nutrition therapy,” “feeding behavior,” “eating behavior,” “exercise,” “physical exercise,” “aerobic exercise,” “physical activity,” “walk,” “jog,” “swim,” “weight lifting,” “dance,” “aerobics,” “physical training,” “resistance training,” “circuit training,” “weight training,” “endurance training,” “structure training,” “physical education,” and “sports” PA. The bibliographies of selected articles were hand searched for additional related references.
Study selection
Eligibility criteria were initially applied by two independent reviewers; any disagreement was resolved through a consensus among all study authors. Based on the population, intervention, comparison, and outcome framework, we established a priori inclusion/exclusion criteria for study identification. 18 We included randomized controlled trials (RCTs) evaluating the role of LSIs on a range of health outcomes of adult (≥18 years) reproductive age group, overweight, and obese women, with PCOS, regardless of their pregnancy status and criteria used to diagnose PCOS. LSI was operationally defined as: dietary intervention alone; combination of diet and PA; or a behavioral intervention to modify either healthy eating alone or combination of healthy eating and PA, irrespective of the duration of the intervention. Studies were considered eligible if the comparison arm received any form of PA alone, any dietary intervention other than the one received by the intervention arm, usual diet, Food and Drug Administration-approved antiobesity medicines (Orlistat, Lorcaserin, Liraglutide, Phentermine/Topiramate, and Naltrexone/Bupropion), and drugs used to manage PCOS symptoms, such as Metformin and Oral Contraceptives. Outcomes of interest included change in weight, insulin resistance marker [homeostatic model assessment-insulin resistance index (HOMA-IR)], and lipid profile, such as total cholesterol (TC), triglycerides (TGs), low-density lipoprotein (LDL), and high-density lipoprotein (HDL). Animal studies, studies comprising of healthy/normal weight/underweight women, with participants receiving supplements/herbal medicines/alternate medicine (e.g., acupuncture)/bariatric surgery, and those without a full text in English language were excluded. We also excluded studies where dietary intervention involved reducing calorie intake to <1200 kcal/day. 19 In addition, conference articles or abstracts and unpublished data were also excluded.
Using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram, two independent reviewers initially identified 850 potential articles by their titles and abstracts 20 (Fig. 1). After removing duplicates, we screened titles or abstracts of 564 articles. Thirty-five full text articles were retrieved for assessment of eligibility where titles and abstracts could not provide relevant information; of these 20 were excluded with reasons. Finally 16 articles (15 RCTs) were included for qualitative synthesis, and 9 studies (8 RCTs) were included in the quantitative synthesis. 21 –29

PRISMA flow diagram of study selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The selected studies provided data on 290 women with PCOS. Four RCTs compared two different diets 22,23,27 –29 ; one intervened with diet versus metformin, 25 while two others used a combination of diet and PA versus metformin/orlistat. 24,26 The duration of interventions ranged from 8 to 24 weeks. Six out of eight RCTs were conducted in low–middle-income countries (Brazil, India, and Iran), one in Denmark, while only one was carried out in the United States. The study participants' age ranged from 18 to 40 years, with body mass index (BMI) from 25 to 55 kg/m2. One study adjusted BMI according to Asian standards and included participants with BMI of 23 kg/m2 and above. 26 Another study did not specify BMI in its selection criteria and reported the average BMI at baseline as 30.6 ± 7.8 and 30.5 ± 8.5 in the intervention and comparator arms, respectively. 29 A comprehensive description of included studies' characteristics is given in Table 1.
Characteristics of Studies Included in the Meta-Analysis
BMI, body mass index; C, control; DASH, dietary approaches to stop hypertension; HDL, high-density lipoprotein; HOMA-IR, homeostatic model assessment-insulin resistance index; I, intervention; LDL, low-density lipoprotein; NS, not significant; PA, physical activity; PCOS, polycystic ovary syndrome; PO, per oral; RCT, randomized controlled trial; TC, total cholesterol; TG, triglyceride; Δ, change.
Data extraction
We used a prior developed data extraction form, based on our selection criteria, for data extraction. Information was retrieved by one reviewer after consultation with all study authors on: (1) study (study design, setting, eligibility criteria, sample size, withdrawal/dropout rate, and risk of bias); (2) participants (baseline characteristics of intervention and comparator groups; (3) intervention versus comparator arm (type, content, frequency, and duration of delivery); and (4) treatment effect on outcome measures. In instances where a trial had multiple publications, we inspected all publications to get comprehensive and accurate information on all aspects of the trial. However, for the sake of outcomes' analysis, we included only those articles that were published after Haqq et al.'s work. 15 Missing data were obtained by contacting study authors of the included studies.
Risk of bias assessment
An assessment of the validity of included studies was carried out in accordance with the Cochrane risk of bias tool (RoB). 30 Bias evaluation was performed using the risk of bias table (Supplementary Table S1). The domains examined for each study included the following: sequence generation (selection bias), allocation concealment (selection bias), blinding of patients, investigators (performance bias) or outcome assessors (detection bias), incomplete outcome data (attrition bias), selective outcome reporting (reporting bias), and other sources of bias. A decision was made for the severity of bias for each of the aforementioned domains and ranked as “low risk” (all or most of the criteria fulfilled, the likelihood of bias affecting effect estimates was small), “high risk” (all or most of the criteria were unfulfilled and bias likely to affect the effect estimates), and “uncertain risk” (insufficient information about any of the criteria to make a clear-cut decision). 18,30 Disagreements about risk of bias were resolved by consensus among the study authors.
Statistical analyses
Statistical analyses were conducted using RevMan Software 5.3. 31 The following data were entered into the RevMan software for both the intervention and the comparator arm of each study: total number of participants and mean changes in outcome measures along with standard deviations (SDs). Where studies reported pre/postintervention outcome measurements, mean changes in outcome measures were first computed for both arms by subtracting the pre- from the postmeasurements. For missing SDs, we either contacted the individual study authors to obtain missing information or calculated SDs using the P values given for the postintervention change in mean for each group. One of the studies included in the meta-analysis—referred to as study 5 or Nyback et al.'s study in our article-had three arms: receiving diet only, combination of diet and PA, and PA only (Table 1). in our article—had three arms: receiving diet only, combination of diet and PA, and PA only. 21 Therefore, we performed two separate meta-analyses for outcomes reported by study 5, that is, weight loss and HOMA-IR—one using study 5 diet-only arm as intervention and the other with combination arm as intervention, while using exercise arm as comparator on both occasions.
The pooled effect sizes were computed using random effect models and reported as standardized mean differences (SMDs) along with 95% confidence intervals (CIs). The effect size was considered significant if the CI of any SMD did not include zero. The SMD is a useful summary statistic in instances where studies use different measurement units or outcome measures, for example, weight loss measured as change in BMI or body weight. It thus makes the results less heterogeneous and more generalizable compared to mean difference. 32 The significance level was set at 5% (P < 0.05). The I 2 test statistic was used to quantify percentage of inconsistency across studies' results not attributed to chance alone. 33
To account for the high variance across studies and given the use of Metformin to treat insulin resistance in PCOS, we performed two different sensitivity analyses 34 : (1) excluding RCTs that used Metformin in the comparison arm and (2) including only those RCTs that used Metformin in the comparison arm.
Results
In this meta-analysis, LSI resulted in significant reduction in weight in sensitivity analysis, insulin resistance index in both main and sensitivity analyses, as well as LDL in both main and sensitivity analyses.
Weight change
Overall LSI, including both dietary and combination interventions, did not have significant impact on weight in overweight and obese women with PCOS. This relationship remained unchanged whether we included study 5 dietary arm as intervention or combination arm (Fig. 2A, B). The change in weight with inclusion of study 5 dietary intervention was at SMD = 0.12 (95% CI = −1.04 to 1.28) and with study 5 combination arm at SMD = 0.10 (95% CI = −1.07 to 1.27).
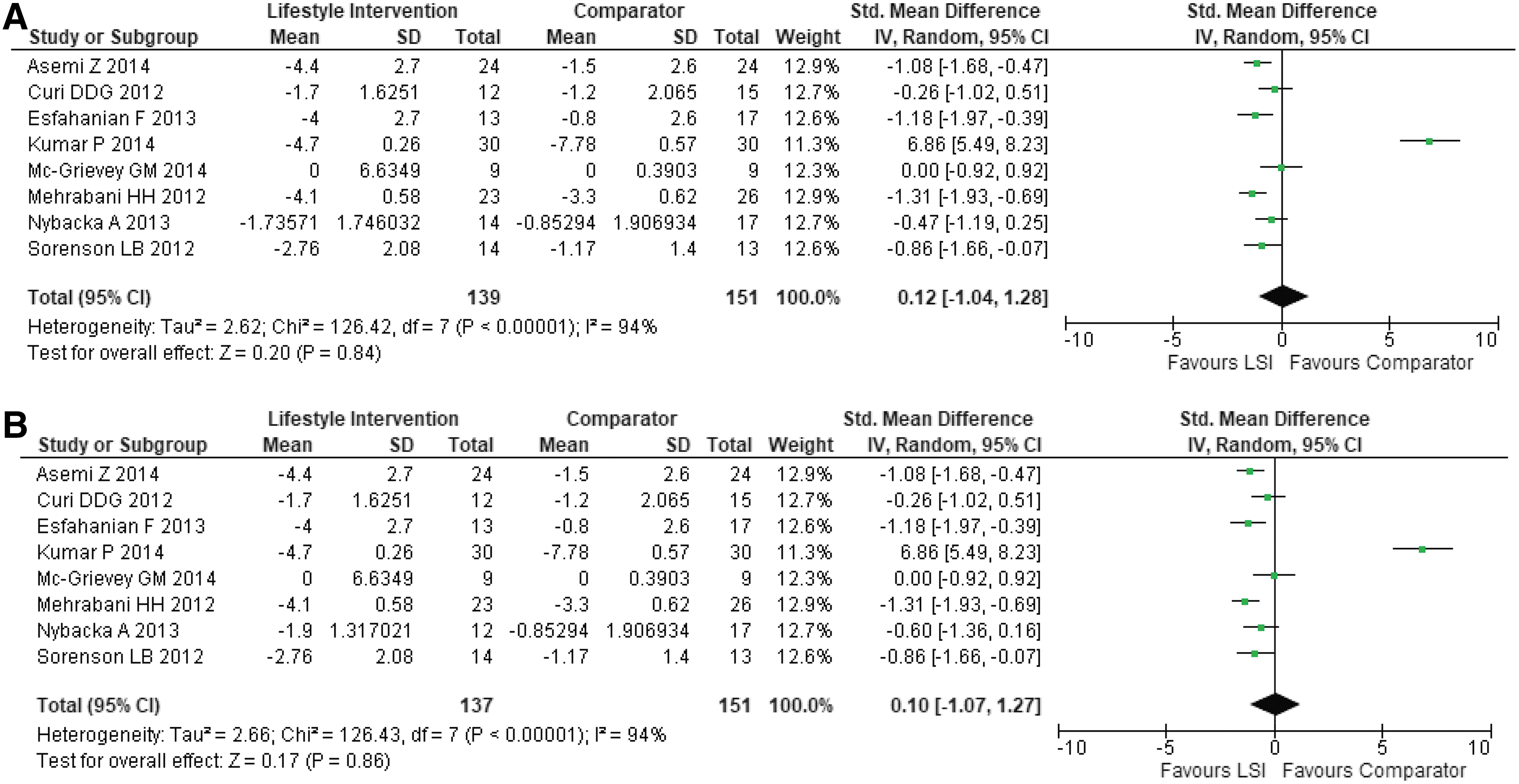
Overall effect of LSI on weight loss.
Sensitivity analyses
After excluding RCTs that used Metformin in the comparison arm (Fig. 3A–C), LSI versus comparator resulted in significant weight loss [using study 5 dietary arm as intervention: SMD = −0.81 (95% CI = −1.24 to −0.39); using study 5 combination arm as intervention: SMD = −0.85 (95% CI = −1.26 to −0.45)]. In contrast, the effect of LSI was not significantly different than Metformin in terms of change in weight with SMD = 1.76 (95% CI = −2.09 to 5.61).
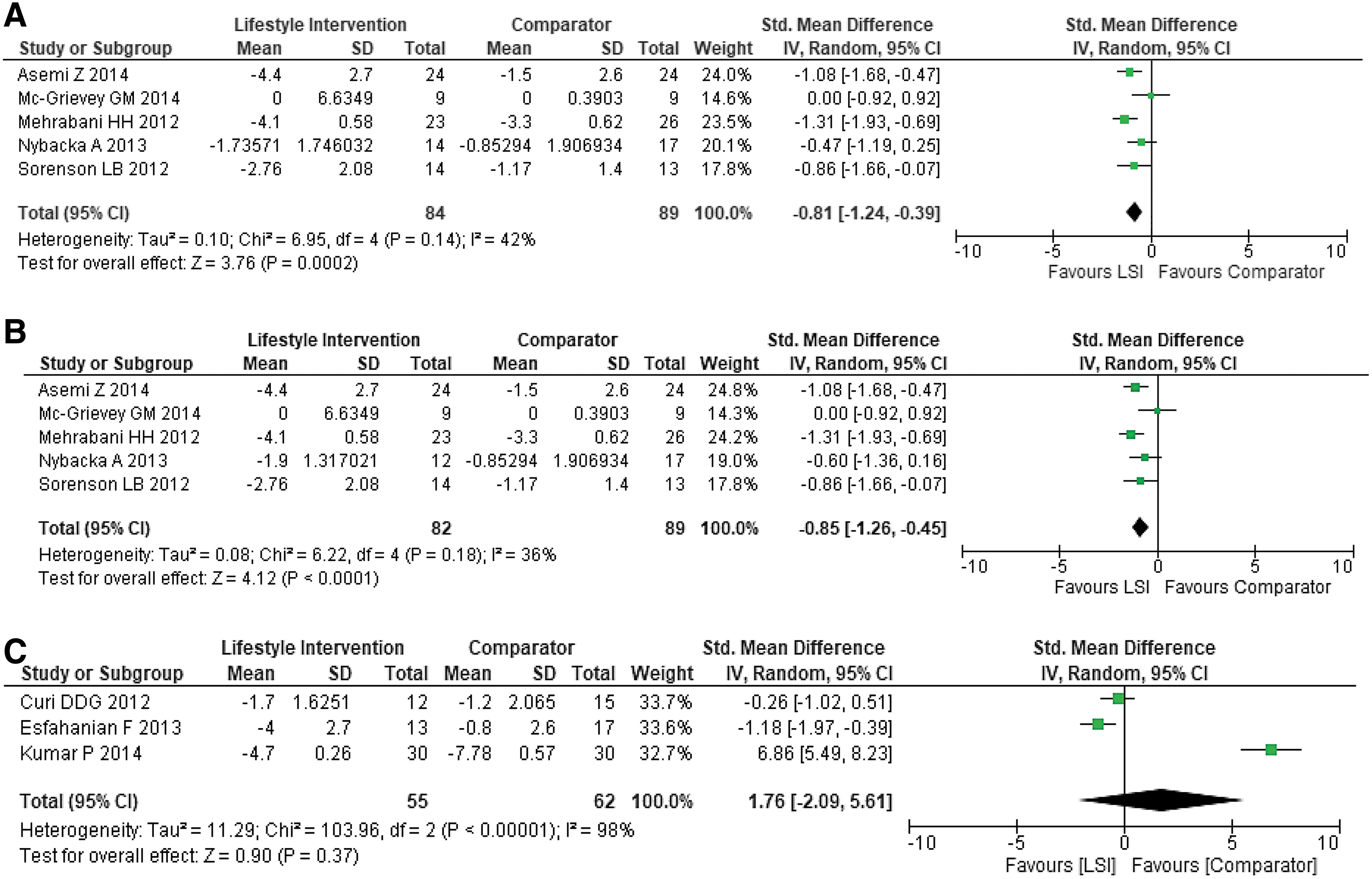
Weight loss sensitivity analyses.
Insulin resistance
Overall LSI, compared with comparator groups, resulted in significant improvement in insulin resistance. The insulin resistance index, HOMA-IR, decreased significantly, with SMD = −1.46 (95% CI = −2.72 to −0.20) after inclusion of study 5 dietary arm as intervention and SMD = −1.50 (95% CI = −2.76 to −0.23) after inclusion of study 5 combination arm as intervention (Fig. 4A, B).
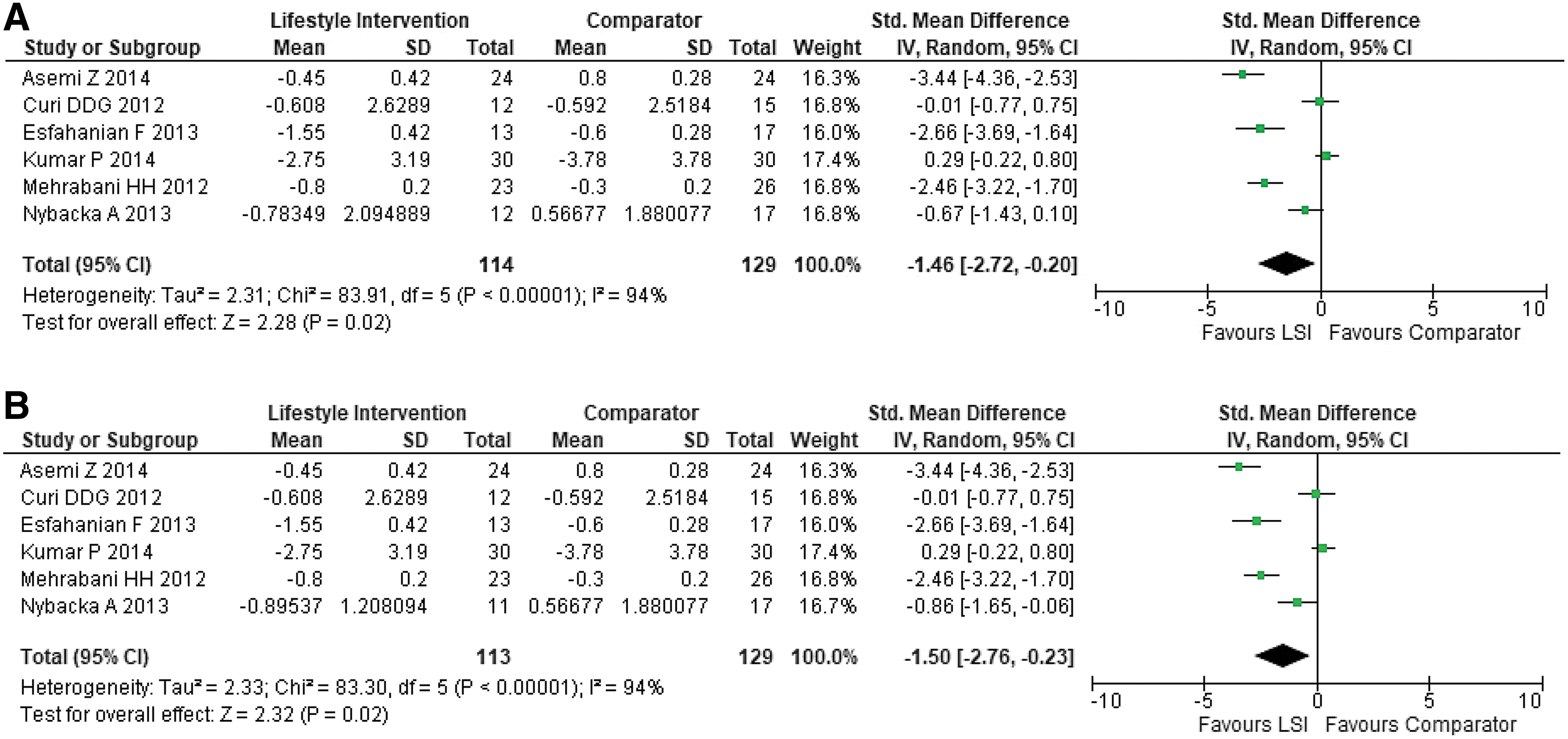
Overall effect of LSI on HOMA-IR.
Sensitivity analyses
When we excluded RCTs that used Metformin in the comparison arm (Fig. 5A–C), the HOMA-IR reduced further with SMD = −2.18 (95% CI = −3.75 to −0.60) and SMD = −2.24 (95% CI = −3.68 to −0.80) using study 5 dietary arm as intervention and study 5 combination arm as intervention, respectively. The effect of LSI on HOMA-IR was not significantly different compared with Metformin with SMD = −0.74 (95% CI = −2.28 to 0.81).

HOMA-IR sensitivity analyses.
Lipid profile
In terms of lipid control, overall LSI versus comparator groups had a beneficial impact. LDL [SMD = −1.06 (95% CI = −2.00 to −0.12)] decreased significantly (Fig. 6A), while there was a downward although insignificant trend in TC [SMD = −1.03 (95% CI = −2.58 to 0.53)], TGs [SMD = −0.81 (95% CI = −2.12 to 0.51)], and HDL [SMD = −0.57 (95% CI = −1.74 to 0.60)] (Fig. 7A–C).
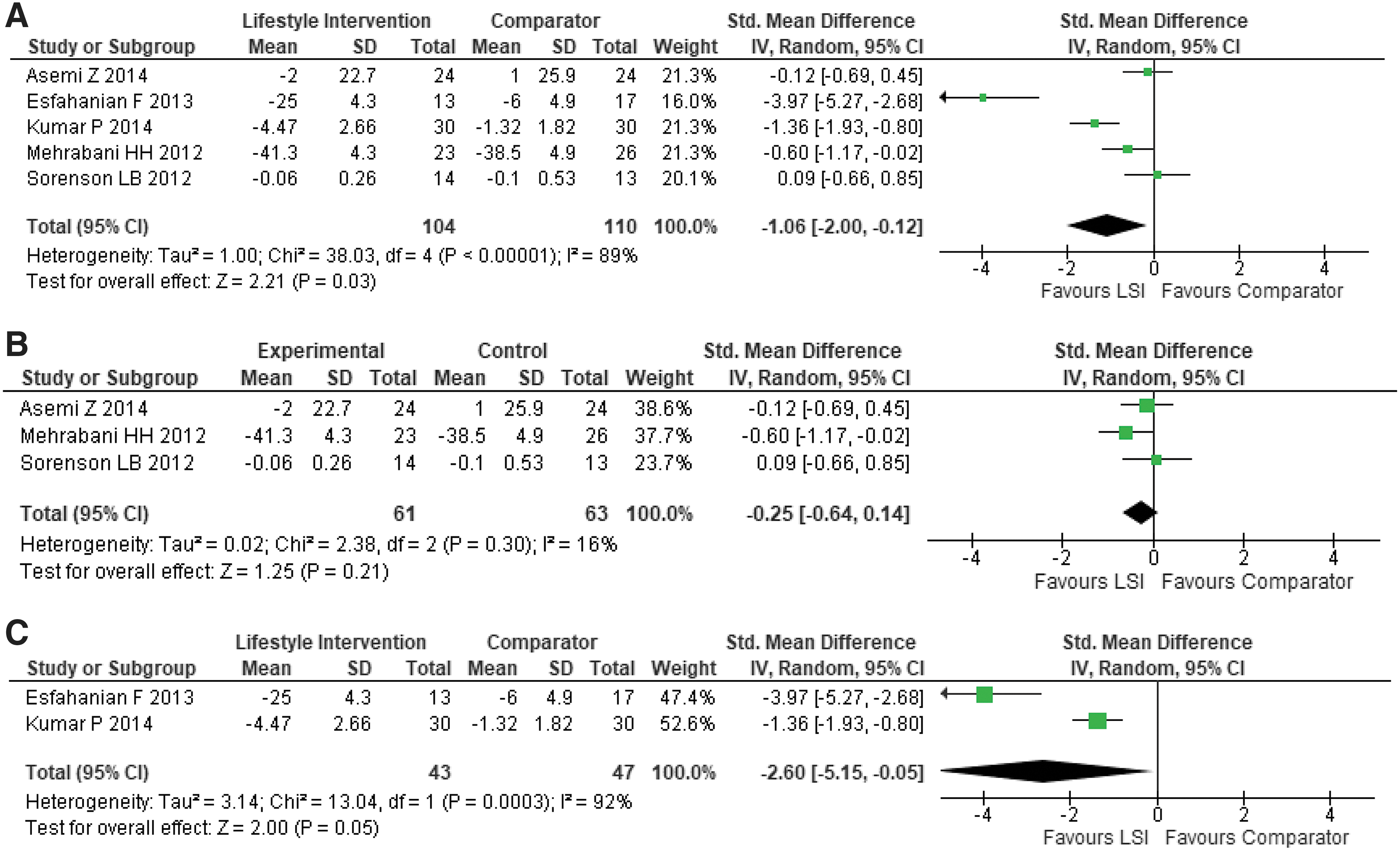
Lipids-LDL:
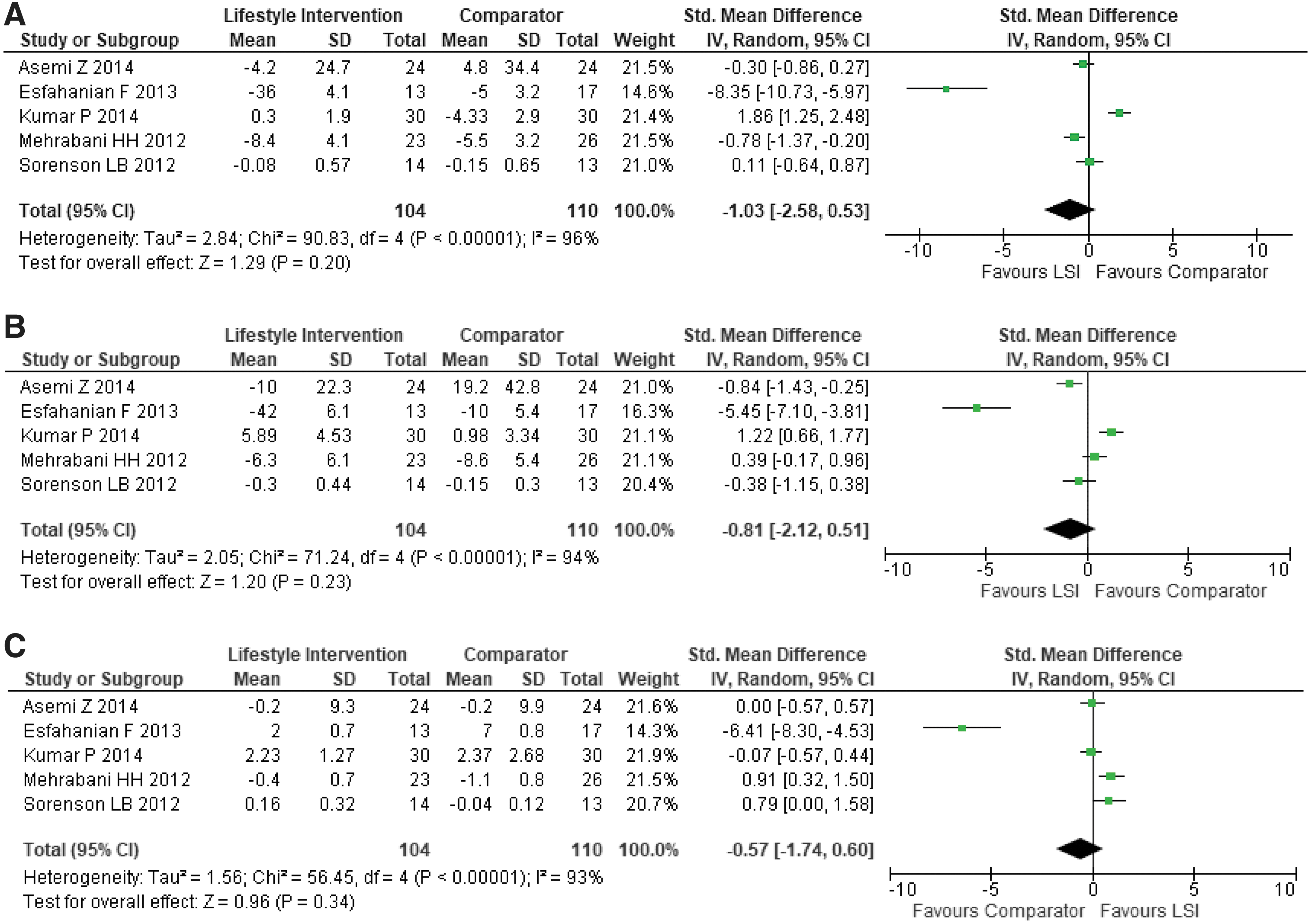
Overall effect of LSI on other lipids.
Sensitivity analyses
Even after excluding RCTs with Metformin as comparator, LSI versus comparator had a nonsignificant effect on TC [SMD = −0.36 (95% CI = −0.85 to 0.12)], TG [SMD = −0.27 (95% CI = −1.04 to 0.51)], and HDL [SMD = 0.55 (95% CI = −0.06 to 1.15)]. Compared with Metformin, LSI had significant improvement in LDL only [SMD = −2.60 (95% CI = −5.15 to −0.05)] (Fig. 6B, C) and nonsignificant effect on TC [SMD = −3.17 (95% CI = −13.18 to 6.83)], TG [SMD = −2.07 (95% CI = −8.61 to 4.47)], and HDL [SMD = −3.17 (95% CI = −9.39 to 3.05)].
Risk of bias analysis
Risk of bias assessment is presented in Fig. 8 and Supplementary Fig. S1. All RCTs described adequate methods of random sequence generation except for one. 24 However, only 2 of 8 studies concealed the allocation assignment. 21,28 Lack of adequate allocation concealment despite random assignment raises concern for selection bias. 30 Except for Asemi et al. 23 and Mehrabani et al., 28 majority of the studies did not blind the participants or the study personnel as it is difficult to perform blinding in most behavioral interventions. This creates potential source of performance bias. However, Sørensen et al.'s 29 and Turner-McGrievy et al.'s 27 studies were regarded at low risk of performance bias as both the arms in both studies received dietary interventions. Only Asemi et al. 23 blinded outcome assessment (by blinding all study personnel, except for the study dietician). Nevertheless, we regarded the objectively assessed outcomes at low risk of detection bias (insulin resistance index and lipid profile) compared to the subjectively assessed weight change. 30 As with behavioral interventions, most of the studies encountered high dropout rates. Three of the seven trials reporting dropouts accounted for the attrition bias by conducting intention-to-treat analysis. 23,27,29 In terms of reporting bias, all studies reported all prespecified outcomes that are of interest in this meta-analysis except for Curi et al., 24 which did not report data on lipid profile. We did not identify any other serious potential sources of bias in the included studies.

Risk of Bias Summary. Review authors' judgments about each risk of bias item for each included study. Green circles with positive symbols represent low risk of bias, red circles with negative symbols represent high risk of bias, and yellow circles with question marks represent uncertain risk of bias.
Discussion
This study presents a systematic review and meta-analysis on the effectiveness of LSI, both dietary and combination of diet and PA, versus comparator groups on cardiometabolic risk factors of overweight and obese women with PCOS. Our work is an update of a prior meta-analysis by Haqq et al. 15 In addition, we evaluated the effect of different forms of diet, independent of PA, on a range of cardiometabolic risk factors, namely weight, insulin resistance, and lipid profile. Our analyses reveal that short-term LSI (both dietary and combination) results in beneficial effect on weight insulin resistance and lipid control. In addition, LSI was not significantly different than Metformin in terms of its effect on weight change and insulin resistance and more effective than Metformin in reducing LDL.
In our study, LSI resulted in significant weight loss only after excluding RCTs comparing LSI versus metformin (sensitivity analysis). However, in the main analysis, weight loss was not statistically significant. The pooled effect estimate in the main analysis was driven predominantly by Kumar and Arora study 26 (Fig. 2). In this study, compared to LSI only arm, the Metformin arm received both Metformin and LSI and subsequently lost significantly more weight probably because the effect of Metformin was potentiated by LSI or vice versa. Nevertheless, the finding of significant weight loss due to LSI in the sensitivity analyses (Fig. 3A, B) corroborates with earlier research and is encouraging, given the high prevalence of obesity among women with PCOS. 6,15,16,35 Moreover, weight loss helps in achieving optimal glycemic and lipid control and is, thus, advantageous to overall cardiovascular health. 36 It is noteworthy here that assessing weight change in terms of BMI could be misleading due to a variety of reasons. BMI doesn't differentiate between loss of lean body mass and body fat—the latter being the most beneficial aspect of weight loss. 37,38 Nonessential body fat poses health risks, such as diabetes mellitus, hypertension, cardiovascular disease, and cerebrovascular accident, and is increasingly being targeted by weight loss/LSIs. 38 Furthermore, BMI has limited sensitivity and specificity and it does not account for other weight influencing factors, namely age, race, sex, and muscle mass. 37 However, both researchers and clinicians continue using BMI and weight to assess an individual's health for ease of measurement and interpretation, as well as inexpensiveness. 38
In terms of insulin resistance in women with PCOS, prior meta-analyses present mixed results. 15,16 Of note, 5 of 8 studies included in our meta-analysis evaluated the effect of dietary modification only versus usual care/Metformin, whereas studies included in prior meta-analyses were assessing PA or combination of PA. We found a beneficial effect of LSI on insulin resistance and LDL, regardless of the dietary composition, in overweight and obese women with PCOS. Visceral adiposity—a common occurrence in women with PCOS—is strongly associated with insulin resistance and hyperlipidemia, both of which are harbingers of cardiovascular disease. 7 However, the relationship between insulin resistance and weight loss is not directly linear. 39 In fact, LSI can positively influence insulin resistance and lipid metabolism, even in the absence of significant weight loss. 40 Consistent with prior studies, we observed a significant decline in LDL and a trend toward improvement in TC and TG. 15,16 Similar to the results of the Diabetes Prevention Program (DPP) research, LSI did not favorably affect HDL in our study. 36 Most of the studies assessing HDL in our meta-analysis focused on the dietary aspect of LSI. It is postulated that reducing total dietary fat intake inevitably decreases HDL level, while exercise tends to increase it. 41 –43 Given that dietary changes tend to cause a decrease in TC, TG, and LDL and increased PA favors increase in HDL, we recommend combining the two approaches as they are likely to have a synergistic effect.
Of particular note is the finding that compared to Metformin, LSI was not significantly different in improving insulin resistance and exhibited superiority in reducing LDL levels in overweight and obese women with PCOS. Perhaps, if the follow-up in the included studies was longer, we could observe a similar decline in insulin resistance also. 35,39 Interestingly, LSI versus Metformin was found to be more effective in preventing diabetes among older participants (>45 years) in the DPP study, 35 whereas our analysis was composed of a relatively younger population. Nevertheless, the above findings and the adverse effects of Metformin justify preferential treatment with LSI while managing women with PCOS having cardiometabolic risk factors. 34
Limitations
Our analyses have several limitations, which warrant further investigation by future studies. Lack of information on blood pressure in the included studies precluded evaluation of this important cardiometabolic risk factor. Based on Cochrane RoB, the evidence presented in the included studies is of low-to-moderate quality. Our study was limited by small sample size. Moreover, the I 2 test statistic, which quantifies the degree of heterogeneity due to variability between studies, was high. Therefore, the results need a cautious interpretation. Possible explanation of high heterogeneity could be variability in terms of duration of intervention, content of intervention, including prescription of diet and PA, study population, as well as the comparator group treatment. In addition, the included studies were conducted in different countries. Therefore, a proportion of heterogeneity in the results could be attributed to different sociocultural trends of the study populations, which shape dietary habits and PA, thereby potentially affecting the outcomes. 44 The comparator group treatment was variable; some followed usual dietary pattern, some received a specific dietary prescription different from that given to the intervention arm, some received an exercise prescription, while others were prescribed metformin. We addressed the variance by performing sensitivity analyses, which decreased the I 2 value for certain outcomes, such as weight loss and LDL. The attrition rate in most of the studies was high as is the case in studies targeting behavioral or lifestyle modification. Selective attrition rate in either group can cause selection bias and compromise external validity of results. 45 This can be efficiently tackled through intention-to-treat analysis, which only few of the included studies performed. Furthermore, the included studies looked at short-term effect of the LSI (≤24 months). It is unclear whether LSI would similarly affect the cardiometabolic profile of overweight and obese women with PCOS in the long term.
Conclusion
Short-term LSI is more effective compared with a comparator group and somewhat comparable with pharmacologic approach, Metformin, in improving weight, insulin resistance, and dyslipidemia. Compared with Metformin, LSI was more effective in reducing LDL in women with PCOS. However, larger studies in diverse populations are warranted to further establish evidence. LSI is a low cost, noninvasive, noninjurious approach that could be used as the first step in the management of overweight and obese women with PCOS, especially those at high risk of developing cardiovascular disease. Our findings could help formulate guidelines for clinicians in the management of overweight and obese women with PCOS. This is crucial given the high prevalence of cardiometabolic risk factors among women with PCOS. 46 Individualized prescription of LSI may result in sustainable benefits and possibly prevent cardiovascular disease, as well as associated complications, in this patient population. 46,47
Footnotes
Acknowledgment
The authors acknowledge Kira Pavlik at Yale School of Medicine who served as the second reviewer and assessed potential articles for study selection.
Ethics Approval and Consent to Participate
Not applicable. The research was conducted in accordance with the Helsinki Declaration as revised in 2013.
Authors' Contributions
K.K. conceived the article; K.K. and V.N. performed the statistical analysis; K.K., V.N., and V.C. interpreted the results; K.K. drafted the initial article; K.K., V.N., and V.C. provided feedback on the content of the article and editorial support; and K.K. modified all subsequent drafts. All authors read and approved the final draft of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS)—HRSA Primary Care Training and Enhancement Grant, Grant Number TOBHP285720100-01-00—as part of an award totaling $1,686,490.00 with 0 percent financed with nongovernmental sources. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the U.S. Government. HRSA has no role in the design of the study, collection, analysis, and interpretation of data, and in writing the article. For more information, please visit HRSA.gov
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.