
Abstract
Background:
Understanding the metabolic syndrome (MetS) prevalence at the national level is important to develop effective programs and strategies to prevent and control MetS. This study aimed to analyze the prevalence of MetS according to gender and aging stage, and its association with potential factors in older individuals ≥60 years of age in Colombia.
Methods:
The data for this study came from a secondary cross-sectional, nationally representative SABE study Survey on Health, Well-Being, and Aging in Colombia, 2015. A total of 1637 participants (60.7% women, 70.5 ± 7.9 years) from 86 Colombian municipalities participated. A structured questionnaire was used to collect data on socio-demography, lifestyle, and self-report medical conditions. Measurements included anthropometric (weight, waist circumference, body mass index), sarcopenia “proxy” status (calf circumference) handgrip strength levels, high-density lipoprotein cholesterol, triglycerides, fasting glucose, and blood pressure. Univariate and multiple regression models were established as part of the main analysis.
Results:
Using the harmonized Joint Scientific Statement criteria, MetS was present in 54.9% of the study population, with a higher prevalence among females than males (59.8% vs. 47.3%). Individuals who were cigarette smokers (odds ratio [OR] = 1.5; 95% confidence interval [CI] = 1.0–2.4; P = 0.034), female gender (OR = 1.3; 95% CI = 1.0–1.8; P = 0.020), and sarcopenia “proxy” (OR = 1.6; 95% CI = 1.0–2.5; P = 0.026) were more likely to have a higher prevalence estimate of MetS, after controlling for relevant covariates.
Conclusions:
Overall prevalence of MetS among older adults in Colombia is high. Smoking, female gender, and sarcopenia “proxy” status are associated with MetS. These results suggested that MetS is still a serious public burden in Colombia, and screening for promotion of healthy lifestyle and nutrition counseling should be offered routinely in old age.
Introduction
The number of elderly people worldwide is expected to double over the next 50 years. 1 –3 Older (>60 years old) in Latin America and the Caribbean will reach ∼101 million (15% of the population). 4 For Colombia, the population of older people is projected to quadruple in the next 35 years, and the mean life expectancy will rise to 77.6 years for women and 69.8 years for men in 2025. 5 Due to this, the Pan American Health Organization (PAHO) and the Merck Institute of Aging and Health advocate for multisectoral action for healthy aging and maintaining the functional ability that enables wellbeing in older age, with special attention to prevention over the causes of morbidity and mortality in older adults, as fundamental key in the health agenda of the Latin Region over the next decade. 5,6
The metabolic syndrome (MetS) is a complex cluster of cardiovascular risk factors that are associated with a sedentary lifestyle, poor nutrition, and consequent obesity, and is strongly associated with cardiovascular diseases (CVD), which include glucose intolerance (type 2 diabetes, impaired glucose tolerance, or impaired fasting glycemia), insulin resistance, abdominal obesity, dyslipidemia, and hypertension. 7,8 Accordingly, MetS increases the risk of developing diseases of cardiovascular origin, such as acute myocardial infarction, 9 ischemic stroke, or coronary heart disease. 10,11 Indeed, having MetS significantly increased the hazard of incident CVD, independent of the presence of subclinical disease (OR = 2.02 95% confidence interval [CI] = 1.45–2.80, P < 0.001). 12
Several studies have deepened in the analysis of the presence of MetS in Latin America reporting its associated factors such as increasing age, Hispanic or indigenous heritage, physical inactivity, high alcohol intake, smoking, history of hypertension or type 2 diabetes (first-degree family members), and belonging to a low socioeconomic status. 13 Likewise, the general prevalence of MetS in Latin American countries has been established in 24.9% (range: 18.8%–43.3%) and is slightly more frequent in women (25.3%) than in men (23.2%). On the other hand, several risk factors for MetS have been suggested, such as alcohol/cigarette smoking intake, residence (urban/rural) and inflammatory markers, 14 dietary factors, such as intake of total fat or saturated fat, 15 physical inactivity, and poor physical fitness. 16
We previously demonstrated in Colombian collegiate students 18–30 years of age that those with the sex (male), age (over 23 years old), weight status (overweight or obese), and having an unhealthy waist to height ratio were more likely to have a prevalence of MetS. 17 In elderly Colombian population, some anthropometric index, such as, body roundness index, and waist-to-height ratio, were proposed as useful screening tools in detecting MetS. 18 Additionally, other studies that included diverse Hispanic/Latino populations, such as Brazilian Eastern Amazon and Ecuadorian older from Quito suggested a marked heterogeneity in risk factor prevalence within this population. 19,20
Latin America has undergone a well-documented epidemiologic transition fuelling a noncommunicable disease epidemic 21 and makeable changes in people's lifestyles that may contribute to greatly increased burden on cluster of cardiometabolic disease as MetS. 13 However, only a few studies have analyzed MetS prevalence specifically in older adults, in whom important changes could still be made to their lifestyles to improve independence and quality of life, as well as preventing other lethal diseases. Therefore, the aim of this study was to analyze the prevalence of MetS according to gender and aging stage, and its association with potential factors in older individuals ≥60 years of age from a sample of the SABE Colombia study. Understanding the MetS prevalence in the national level is important to develop the effective programs and strategies to prevent and control MetS.
Materials and Methods
Study design and sample population
This study is part of the 2015 SABE study Survey on Health, Wellbeing, and Aging in Latin America and the Caribbean, which is a multicenter project conducted by the PAHO and supported by the Epidemiological Office of the National Health Ministry in Bogotá, Colombia (
Institutional Review Boards involved in developing the SABE-Colombia study (University of Caldas, ID protocol CBCS-021-14, and University of Valle, ID protocol 09-014 and O11-015) reviewed and approved the study protocol. Written informed consent was obtained from each individual before inclusion and completion of the first examination. Permission and details available in
The survey included elderly Colombians (≥60 years) using purposive, randomized sampling (urban and rural areas). In this subsample (N = 4,525), 86 municipalities were defined for blood sampling, and 2 out of every 5 people were called to participate. For this analysis we use data from 1637 participants included as a subsample with MetS components.
Measurements
Data collection staff was trained by the research teams of the coordinating centers (Universities of Caldas and Valle) for face-to-face interviews and physical measurements. Body mass index (BMI) was estimated in kg/m2 from the measured weight and height and the sample was categorized by underweight (BMI <18.5), normal weight (BMI = 18.5–24.9), overweight (BMI = 25–29.9), and obesity (BMI >30). 24 Sarcopenia was defined according to calf circumference (CC) as a “proxy” measure for assessing early identification of sarcopenia in clinical practice, due to the low cost and ease of obtaining. 25 A CC smaller than 31 cm is considered to be indicative of sarcopenia in older population as has been previously reported in several studies. 26,27
Blood pressure, diastolic blood pressure (DBP), and systolic blood pressure (SBP), was measured with subjects in rest (5-min) with an automated procedure using the OMRON HEM–705 monitor (Omron® Healthcare Europe BV, Hoofddorp, The Netherlands).
Blood samples were taken by puncturing the capillary vein under standardized conditions, with the participant having fasted at least 10–12 hr beforehand. The biochemical profile included: (i) high-density lipoprotein cholesterol (HDL-C); (ii) triglycerides; (iii) low-density lipoprotein cholesterol (LDL-C); (iv) total cholesterol; and (v) glucose fasting. Samples were analyzed by standard enzymatic colorimetric methods.
Handgrip strength was assessed on a Takei dynamometer (Grip Strength Dynamometer Model T.K.K. 5001®; Takei Scientific Instruments Co., Ltd., Niigata, Japan), including the highest value (kg) from two attempts (both hands). Handgrip strength was categorized into three levels by gender (low, moderate, and high) according to the KORA-age study. 28
For the lifestyle, personal habits regarding alcohol intake and smoking were measured. Regarding alcohol intake, participants were categorized as a current have alcoholic intake or not and regarding smoking status, as smokes or not. A “proxy physical activity” report was conducted by the following questions: (i) “Have you regularly exercised, such as jogging or dancing, or performed rigorous physical activity at least three times a week for the past year?” (ii) “Do you walk at least three times a week between 9 and 20 blocks (0.6 to 1.2 km) without resting?” and (iii) “Do you walk at least three times a week 8 blocks (0.5 km) without resting?” Participants were considered physically active if they responded affirmatively two of the three questions. Self-reported medical conditions (hypertension, diabetes, respiratory diseases, cardiovascular diseases, stroke, osteoporosis, cancer) were assessed by asking the participants if they had a diagnosis made by a physician. To identify the socioeconomic status, the classification of strata of the public utilities was used (level 1 to level >5).
Definitions of MetS
MetS was defined according to the most recent Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention 29 by adopting the Ethnic Central and South American criteria for waist circumference. Participants were classified as having MetS if they had at least three of following metabolic risk factors or components (MetS components): abdominal obesity by high waist circumference (HWC) (waist circumference ≥90 cm for Latin American men and ≥80 cm for Latin American women; high levels of fasting triglycerides (HLFTg) (fasting serum triglycerides ≥150 mg/dL or taking medication for abnormal lipid levels); low levels of HDL-C (LLHDL) (fasting serum HDL-C <40 mg/dL in males; <50 mg/dL in females or specific treatment for this lipid abnormality); elevated arterial blood pressure (EABP) (SBP ≥130 mmHg or DBP ≥85 mmHg or taking hypertension medication); high levels of fasting glucose (serum glucose level ≥100 mg/dL or taking diabetes medication).
Potential associated factors
Potential associated factors included, aging state (from stage I to stage IV), socioeconomic status (from level 1 to >5), geographical area (urban or rural), ethnic group (indigenous, black, white, and others), nutritional status (from underweight to obese categories), gender (male/female), sarcopenia status (≤31 cm sarcopenia/yes or >31 cm no sarcopenia), handgrip strength categorized into 3 score by gender (high, moderate, and low), alcohol intake (never or no/current or yes), smoking habits (never or no/current or yes), and physical activity “proxy” levels (active, yes/physical inactivity, no).
Statistical analysis
General characteristics from the study sample are presented as frequency and percentage or as the mean and standard deviation (SD) for overall sample and according to have MetS or not. Statistical differences between participants with MetS and No-MetS have been analyzed by chi-squared test for categorical variables, and by Student's t-test (variables with normal distribution) or Mann–Whitney U for continuous variables. Descriptive analysis of the prevalence of the MetS by gender and age stages, as well as, a descriptive analysis of the MetS components have been presented in figures using percentages. Differences by gender in the prevalence of MetS condition have been analyzed by chi-squared test. McNemar test was used to analyze the differences in the prevalence of MetS by aging stage.
Simple logistic regressions were performed individually for each MetS potential associated factors to analyze the association with MetS, whereas a multiple logistic regression was used to identify the main predictor or factors associated with MetS, including only factors with significant association in the univariate analysis. For both analysis, MetS was included as the dependent variable (reference: to have MetS). Multiple logistic regression was adjusted by the following confounders: age, ethnicity, socioeconomic status (level 1 to level >5), geographical area (urban or rural), BMI, and self-reported medical conditions (presence or absence of hypertension, diabetes, respiratory diseases, cardiovascular diseases, stroke, osteoporosis, or cancer). Gender with males as an indicator, sarcopenia (reference: no sarcopenia), handgrip strength with the high level of strength as an indicator, smoking habits (reference: no smoke), alcohol habits (reference: no alcoholic intake), and physical activity habits (reference: yes), were included as fixed factors. The covariates included in the adjusted analyses were based on conceptual model according to the literature. 14 –17 The analysis of the data was performed with the SPSS statistical software package, version 24.0 (IBM, Chicago, IL) for Windows.
Results
Sociodemographic and clinical characteristics of the sample study
The general characteristics of the participants are presented according to the overall sample, and MetS condition in Table 1. Most of the participants (n = 525) belonged to the aging group III (70–80 years). Level 2 of socioeconomic status (42.6%), urban area (83.3%), and other ethnic groups (45.8%) were the most prevalent sociodemographic characteristics. The waist circumference and BMI mean in the overall sample were 92.5 cm and 27.3 kg/m2, respectively. Most of the sample had abdominal obesity (78.6%), and an overweight status (41.3%), but a healthy sarcopenia status (86%). MetS components for the overall sample were systolic blood pressure (132.6 ± 23.5 mmHg), triglycerides (160.9 ± 83.3 mg/dL), and LDL-C (126.8 ± 35.3 mg/dL) levels. The handgrip strength mean for the overall sample was 32.4 kg, with prevalence at high levels category (59.4%).
General Characteristics of the Population According to Metabolic Syndrome Status
Data are presented as frequency and percentage.
Continuous variable are expressed as mean ± SD. Missing data: Abdominal obesity = 2; sarcopenia = 18; handgrip strength = 92; smoking habits = 1; alcoholic habits = 1; physical activity habits = 3; glycemia = 15; triglycerides = 5; HDL-C = 8; hypertension = 5; diabetes = 4; respiratory diseases = 1; osteoporosis = 4.
Others (mestizo, gypsy, etc.).
Low: men ≤30 kg; women ≤18 kg. Moderate: men >30 and ≤38 kg; women >18 and ≤24 kg. High: men >38 kg; women >24 kg. P value in bold.
ADBP, arterial diastolic blood pressure; ASBP, arterial systolic blood pressure; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; MetS, metabolic syndrome; SD, standard deviation; WHO, World Health Organization.
Regarding lifestyle habits, the majority of the sample does not smoke and does not take alcohol (90.8%) and (87.9%), respectively. Most of the participants were not physically active according to the “proxy” recommendations (82.9%). Related to the analyzed medical conditions, hypertension was the most common (44.2%), followed by diabetes (16.4%), cardiovascular diseases (14.3%), and osteoporosis (12.7%).
The overall prevalence of MetS in the study sample was 54.9% (95% CI = 52.4–57.3). Significant differences between participants with MetS condition and participants without MetS condition were observed related to several variables. According to sociodemographic characteristics, there were significant differences in ethnic categories. Related anthropometric characteristics of the sample, participants with MetS presented significantly higher values of waist circumference, and all blood parameters, except HDL-C concentration and handgrip strength, the values were lower compared with participants with No-MetS. In addition, participants with MetS showed significantly higher prevalence compared with No-Mets participants in overweight and obesity nutritional status, abdominal obesity, and the following medical conditions, such as hypertension, diabetes, and cardiovascular diseases.
According to Fig. 1, MetS was significantly more prevalent in females than in males (59.8% vs. 47.3%); P < 0.001. Prevalence of MetS was significantly highest in females for aging group II and III compared with males (63.6% vs. 45.9% P = 0.001 and 64.6% vs. 47.2% P < 0.001, respectively). Males did not present differences in the prevalence of MetS among the different age stages (P = 0.936), whereas females presented the significantly highest prevalence of MetS in group III (70–80 years) compared with the rest of the aging stage (P = 0.021).
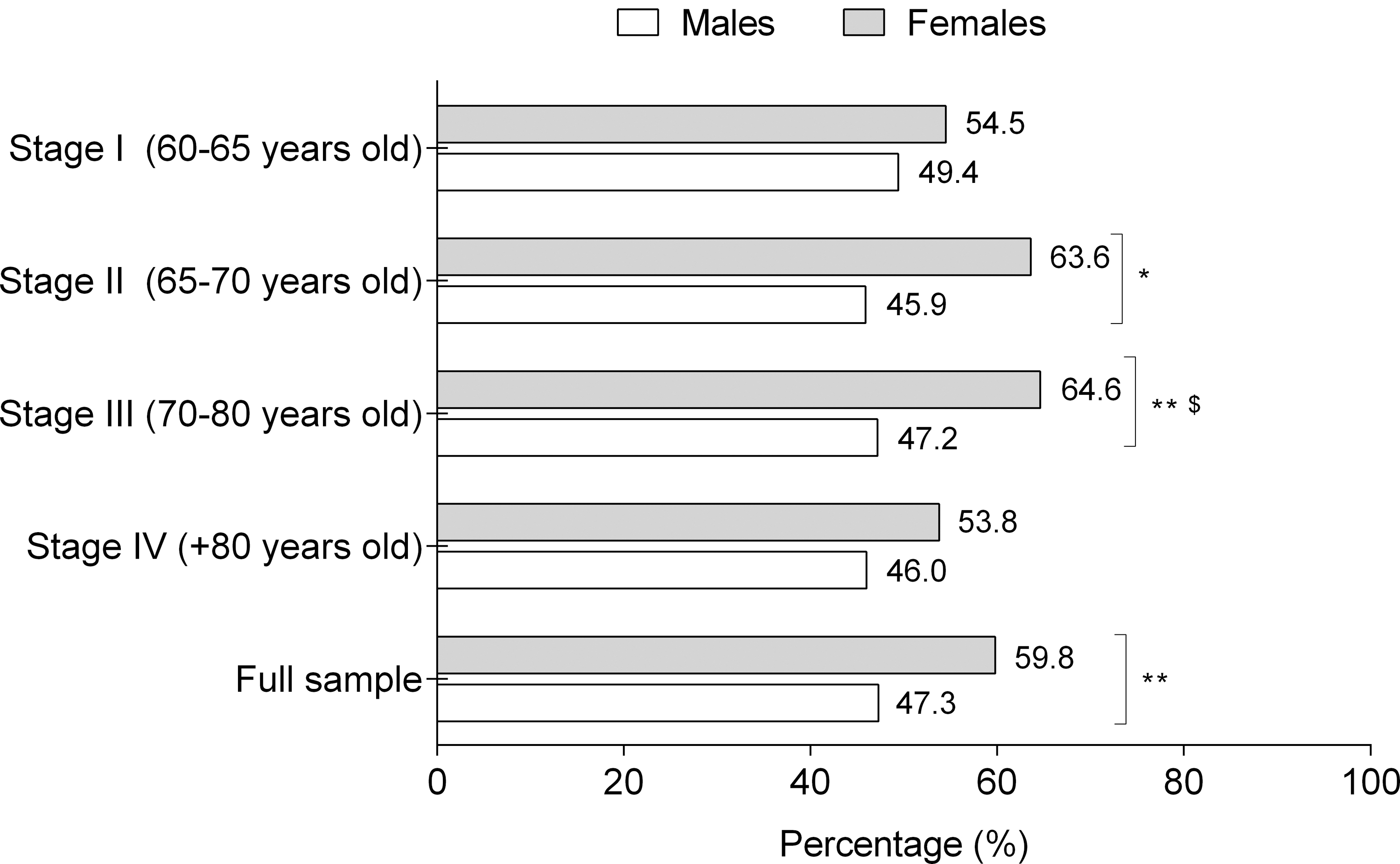
Prevalence of MetS according aging stage and gender. Statistical differences *P = 0.001, **P < 0.001. $Significant differences compared with the rest of the groups.
Distribution of MetS components
The distribution of MetS components for the overall sample and for the participants with syndrome is presented in Fig. 2. For the overall sample (Fig. 2A), the most prevalent MetS components were HWC (78.6%), LLHDL (57.2%), EABP (53.3%), and high levels of fasting blood triglycerides (HLFBTg) (45.7%). Elevated fasting blood glucose was the least common component of MetS (31.1%). The most prevalent MetS components in participants with syndrome were HWC (95.2%), following of LLHDL (84.1%) and HLFBTg (71.3%), Fig. 2B. Related to the MetS components by gender in the overall sample (Fig. 2C), the greatest differences were observed for HWC and LLHDL, with a higher prevalence in females compared with males (HWC: females = 88% vs. males 64%, P < 0.001 and LLHDL: females = 60.7% vs. males = 51.7%, P < 0.001). The prevalence of HLFBTg was also significantly higher in females than in males (females = 48.8% vs. males = 40.8%, P = 0.001). However, males presented a higher prevalence of EABP than females (57.2% vs. 50.8%, P = 0.001). Finally, in participants with MetS the most prevalent MetS components were also HWC (female = 98%; male = 89%), LLHDL (female = 85.2%; male = 82.1%), and EABP (males = 75.4% vs. females = 60.2%; P < 0.001, Fig. 2D).

Factors associated with MetS
Previous univariate analysis (Table 2) showed the odds ratios (ORs) for the potential factors associated with MetS among the Colombian older adults. Female gender (OR = 1.6, 95% CI = 1.3–2.0; P < 0.001), to have abdominal obesity (OR = 14.0, 95% CI = 10.0–19.7; P < 0.001, overweight and obese nutritional status (OR = 12.0, 95% CI = 3.5–41.1; P < 0.001 and OR = 14.7, 95% CI = 4.2–50.6; P < 0.001, respectively), a sarcopenia “proxy” status (OR = 2.5, 95% CI = 1.9–3.4; P < 0.001), and a low handgrip strength level (OR = 0.7, 95% CI = 0.6–0.9; P = 0.011) were the potential factors that presented a significant association with the condition of MetS (independent regression analysis for each factor). Obese or overweight nutritional status, abdominal obesity, and sarcopenia “proxy” status were the potential factors with the highest values in the risk of occurrence of the MetS.
Univariate Analysis of Metabolic Syndrome Potential Associated Factors
P value in bold = significant association.
CI, confidence interval; OR, odds ratio.
Subsequently, a multiple regression model adjusted by the main confounders (see Statistical Analysis section) was performed, where all potential factors with a significant association in the previous univariate analysis were included (Fig. 3). The female gender (OR = 1.3; 95% CI = 1.0–1.8; P = 0.020) and a sarcopenia “proxy” status (OR = 1.6; 95% CI = 1.0–2.5; P = 0.026) remained significantly associated with MetS. In addition, being a smoker was positively associated with MetS (OR = 1.5; 95% CI = 1.0–2.4; P = 0.034).
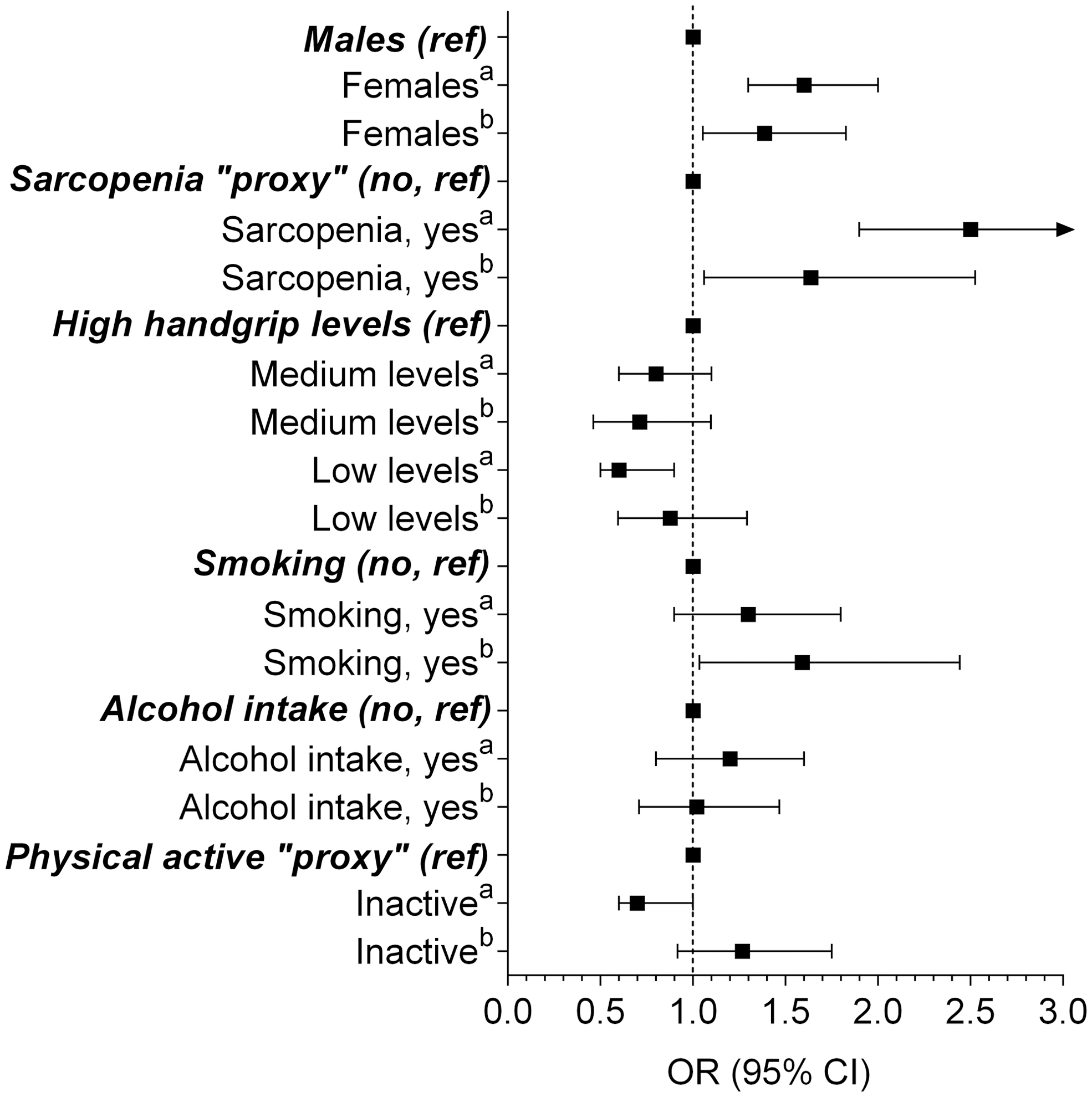
Multiple regression model of potential factors for the prevalence of MetS. Analysis was adjusted by age, ethnicity, socioeconomic status, urbanicity, BMI, and medical conditions (presence or absence of osteoporosis, cardiovascular diseases, hypertension, diabetes, stroke, cancer, or respiratory diseases). aUnivariate analysis; bmultiple regression analysis. BMI, body mass index.
Discussion
The main findings of the present study were the considerably high prevalence of MetS in the sample (54.9%) being more prevalent in females than in males especially during the ages of 65 to 80 years. According to Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention criteria, a high waist circumference, LLHDL, and EABP were the MetS components more prevalent for the overall sample, whereas a high waist circumference, LLHDL, and HLFTg were the most common in participants with the MetS. Several gender differences were observed regarding MetS component prevalence. In addition, female gender, a presence of sarcopenia, and smoking were identified as the main predictors or factors significantly associated with the probability of suffering MetS.
It should be noted that while the prevalence of MetS in the present sample is high (54.9%), it is similar to other Latin American studies in older people, such as Ecuador 59.9%, 30 Brazil with 51.5.%, 19 Southern Cone of Latin America with 53%, 31 in Ecuador elders (≥65 years) with 40%, 20 Colombia with 52.2%, 32 and in the CARMELA study with 35.5%. 33 A reasonable explanation for the high prevalence of MetS in the present study could be that most of the sample belonged to an urban area (83.3%), where people have a higher risk of MetS. 34,35 This might be due to several lifestyle aspects, such as dietary patterns or low physical activity levels, as was found in our study, where most of the sample (82.9%) was insufficiently active.
According to our results regarding gender, in the six Latin American studies previously mentioned, 19,20,30 –33 females also had a higher prevalence of MetS than males in general, and particularly in the older adult groups (when it applied). As previously reported, MetS is more common in females in an older North American population of Mexican origin. 36 Many of the typical aspects of MetS, such as increased abdominal adiposity and dyslipidemia, hyperglycemia, and hyperinsulinism, are experienced in females along the menopausal transition. 37 The cessation of estrogen secretion at the beginning of menopause accentuates these aspects, decreasing the quality of life. 38 Additionally, it seems that the onset of menopause begins earlier in Latin American countries than in Europe and USA, what may be associated with higher altitude residency, and lower education/economical income. 39,40 In the present study, the overall sample belonged to social status 1–2 (72.7%), and with a residency at high altitude (Bogota, 2680 m), but without significant differences between participants with MetS and no-MetS.
Consequently, scientific investigations on Latin American postmenopausal women related to the MetS prevalence and its associated factors have increased, 41 although little is known about older adult populations. In addition, males presented the highest MetS prevalence (49.4%) in the aging group I (60–65 years), but not in the later ones. In agreement with our results, in a cross-sectional analysis of 4289 Taiwanese individuals, 42 the male:female MetS ratio reversed after the age of 60 (men 30.4% vs. women 40.3%). Similarly, in a large population-based project enrolling 36 cohorts from 10 European countries, 43 there was an increase in the prevalence of MetS from age groups 19–39 to 60–78 years and was nearly twofold in males, and fivefold in females, resulting in a higher prevalence of MetS in women after the age of 50. Again, the typical changes in the hormonal status during and after menopause could explain the significant influence of gender in the age-related increase of MetS. 44,45 Other explanation could be due to fluctuations in individual and social behavior, such as modifications in socioeconomic status or adoption of an unhealthy lifestyle. 46
Overall, the most prevalent MetS components were abdominal obesity (78.6%), LLHDL (57.2%), and high levels of triglycerides (45.7%). Likewise, in the study of Davila et al., 32 where 312 (34.7% of the whole sample) older adults (55–64 years) from Medellin (Colombia) were evaluated, the major MetS metabolic risk factor was increased waist circumference with a prevalence of 87.4%, followed by LLHDL (59.1%), high levels of triglycerides (52.0%), and blood pressure (44.8%). Concerning MetS components analyzed by gender in the whole sample, several statistical differences were observed. For instance, females presented a higher prevalence of increased waist circumference and LLHDL than males. Moreover, females displayed significantly higher triglycerides levels than males, but males presented a higher prevalence of high blood pressure. Accordingly, in a French study conducted in 3508 participants, females presented a higher prevalence of abdominal obesity and LLHDL, whereas high blood pressure was the most commonly found metabolic disorder in males similar as our result in both, for overall sample and for the participants with MetS condition; however, the age range only covered 35–64 years. 47 Alike, a Taiwanese study found a high prevalence of blood pressure and hypertriglyceridemia in males below 60 years, although without differences in MetS components between genders in the age group above 60 years. 48 Additionally, a large Korean study, including 103,763 participants 66 years of age or older revealed that females had a significantly higher percentage of abdominal obesity (+12%) and lower HDL-C levels (−47%) than men, whereas men presented higher rates of high blood pressure levels (+6%). However, contrary to our results, the Korean study indicated that men had usually high levels of triglycerides (+5%), compared with woman, 49 whereas in our study, females presented higher levels of fasting triglycerides in both, overall sample (+8%) and in participants with MetS condition (+4.4%). Unfortunately, gender-related differences are sensitive to several factors related to social and cultural conducts, dietary behaviors, and psychosocial aspects. 44
Finally, the multiple regression model (after adjustment) indicated that the potential factors that were associated with MetS were female gender, to have a sarcopenia status and smoking. The two last were the main risk factors associated with MetS in this sample of Colombian older adults, with more than 1.5 times the approximate risk of occurrence of MetS. In accordance with our results of univariate and multiple regression analysis, the prevalence of the MetS is growing higher in women than in men in the last decades, which could be due to the constant rise in obesity in women. 50,51
Additionally, numerous studies have shown the high prevalence of MetS and associated risk in people with a nutritional status of normal weight near the upper range or slightly overweight. 52 Moreover, sarcopenia has been linked to several metabolic disorders, and a recent meta-analysis revealed that it is positively associated with MetS in middle-aged and older nonobese people. 53 In our study, sarcopenia status was high (14% for the overall sample) compared with a previous study carried out in the same region, 54 where 6.96% of the participants (≥60 years old) presented sarcopenia. Also, our sarcopenia prevalence is higher than most of the studies conducted in older adults in other countries, going from Belgium with 12% to the United States with 5%, but not Japan (24.2%). 53 However, stratification cutoff values for community-dwelling populations could vary between studies, as well as age range included.
Lastly, regarding the significant association between MetS and smoking status, a previous review presented several studies, where smoking is associated with metabolic abnormalities and increases the risk of MetS. 55 In a Latin American context, specifically in Venezuela, smoking represents a related factor with MetS, being associated with low HDL-C, elevated abdominal circumference, and triglycerides. 56 Additionally, a previous Chinese study showed that active smoking in men was strongly associated with increased CVD risk, 57 independent of the presence of MetS. Moreover, tobacco smoke exposure (including active and passive smoking) increased the prevalence of coronary heart disease, stroke, and CVD in older of both genders with or without MetS. 57
In conclusion, the prevalence of MetS is 54.3% among Colombian older adults and females and presented the highest prevalence of MetS irrespective of the aging stage. High abdominal obesity was the main prevalent MetS component (78.5%). Female gender, sarcopenia status, and being a smoker were found to be significantly associated with the probability of suffering MetS. New health policies and prevention strategies focused on the elderly Latin American population should be implemented based on these findings.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This study is part of a larger project that has been funded by a Colciencias y Ministerio de Salud y la Protección Social de Colombia (The SABE Study ID 2013, no. 764). The funder had no role in the study design, data collection, data analysis and interpretation, the preparation of the article, or the decision to publish. Mikel Izquierdo is funded in part by a research grant PI17/01814 from the Ministerio de Economía, Industria, y Competitividad (ISCIII, FEDER). Robinson Ramírez-Vélez is funded in part by a Postdoctotal fellowship grant ID 420/2019 of the Universidad Pública de Navarra, Spain.