
Abstract
Background:
Different studies have indicated that thiazide diuretics can increase the risk of developing type 2 diabetes (T2D). Therefore, in this study, we investigated whether switching from hydrochlorothiazide (HCTZ) to amlodipine resulted in ameliorating different cardiovascular and metabolic measures in hypertensive patients with or without T2D.
Methods:
This study [Diuretics and Diabetes Control (DiaDiC)] was a 6-week, single-blind, single-center randomized controlled trial. The first 20 normal glucose-tolerant, 20 prediabetic, and 20 T2D consecutive patients were randomized to continue the previous antihypertensive treatment with HCTZ (12.5–25 mg/day) or to switch from HCTZ to amlodipine (2.5–10 mg/day). The primary endpoints were the absolute change in 7-day continuous subcutaneous glucose monitoring (CSGM) glycemia, serum uric acid concentrations, and endothelial function [measured as flow-mediated dilation (FMD)]. Other secondary endpoints were investigated, including changes in glycated hemoglobin (HbA1c), glycemic variability from 7-day CSGM, and the estimated glomerular filtration rate (eGFR).
Results:
Amlodipine treatment was associated with a significant reduction in HbA1c (P = 0.03) for both 7-day CSGM glycemia (P = 0.01) and glycemic variability (coefficient of variability %: HCTZ +3%, amlodipine −2.8%), and a reduction in uric acid concentrations (P < 0.001), especially in participants with T2D or prediabetes. Following amlodipine treatment, a significant increase in both eGFR (P = 0.01) and FMD (P = 0.02) was also observed.
Conclusions:
This study demonstrates that the replacement of HCTZ with amlodipine has several metabolic and cardiovascular beneficial effects. However, further intervention studies are necessary to confirm the clinical effects of thiazides, especially in diabetic people and in those at risk of diabetes.
Introduction
Hypertension is a widespread condition that is frequently associated with insulin resistance, metabolic syndrome, and type 2 diabetes (T2D); overall, patients with hypertension are twofold more likely to develop T2D than those who are normotensive. 1 In addition, the antihypertensive medications may have a large impact on the risk of T2D. 2,3 Thiazide diuretics, in particular, are among the most used and effective antihypertensive drugs 4 and, even recently, they have been included among the first-line medications to be used for hypertension. 5 However, different studies indicated that thiazide and thiazide-like diuretics can increase the risk of developing T2D. 6,7 We previously demonstrated 8 in the cohort of about 1000 adults without previously known diabetes or atherosclerotic cardiovascular disease of the ABCD study that treatment with diuretics [hydrochlorothiazide (HCTZ) in more than 80% of cases], even at low doses, was associated with both insulin resistance and increased serum uric acid levels, the latter being a well-established metabolic factor contributing to the cardiovascular risk. 9,10 We also found evidence that the use of diuretics was associated with abnormal glucose tolerance. 8 On the contrary, other classes of antihypertensive drugs as renin-angiotensin system blockers, namely angiotensin-converting enzyme inhibitors (ACEI) and angiotensin receptor blockers (ARBs), have been indicated to reduce the risk of developing T2D compared with placebo, or to have a neutral effect as in the case of calcium channel blockers (CCB). 11 Despite the importance of addressing the global cardiovascular risk, 5 especially in hypertensive patients with concomitant conditions as central obesity, prediabetes, or T2D, there are no sufficient data concerning the potential metabolic risk associated with thiazide diuretics or showing unfavorable cardiovascular outcomes in patients treated with these drugs. We hypothesized that thiazide-treated hypertensive patients might benefit from substituting this medication with a metabolically neutral CCB. Therefore, in this study, we investigated if switching from HCTZ to amlodipine resulted in ameliorating different cardiovascular and metabolic measures in hypertensive patients with or without T2D.
Research Design and Methods
The Diuretics and Diabetes Control (DiaDiC) was a 6week, single blind, single-center randomized controlled trial (ISRCTN03504931) that examined the cardiovascular and metabolic effects of two different treatments of hypertension: (i) continuation of the previous antihypertensive treatment that included the diuretic HCTZ versus (ii) switch from the treatment with HCTZ to the CCB amlodipine. The study was carried out at the Diabetes, Obesity, Hypertension and Clinical Nutrition center of the university hospital Policlinico “P. Giaccone” of Palermo (Italy). The study protocol was approved by the ethical committee of the University Hospital Policlinico “P. Giaccone” of Palermo (I) (approval number 06/2013); each participant signed an approved informed consent form.
Participants
Adult Caucasian patients with hypertension, including normal glucose tolerant (NGT), prediabetic (PD), or T2D people, were recruited among those attending the outpatient clinic (September 2013–March 2014). Glucose tolerance (PD and T2D) was defined according to the American Diabetes Association diagnostic criteria. 12 Inclusion criteria were age 30–80 years, hypertension for <15 years with basal blood pressure <140/90 mmHg, nondiabetics or having diabetes for <15 years, and using HCTZ for at least the last 6 months. Exclusion criteria were average 24-hr blood pressure from ambulatory blood pressure monitoring (ABPM) >160/90 mmHg, concomitant use of ≥3 antihypertensive drugs, habitual use of CCB or other classes of diuretics different from thiazides, habitual use of nonsteroidal anti-inflammatory drugs, corticosteroids, lithium salts, or other medications that are known to impact glucose metabolism, allergy or intolerance versus CCB, self-monitoring mean glycemia >250 mg/dL, glycated hemoglobin (HbA1c) >10%, smoking of >10 cigarette/day, habitual use of distilled spirits or wine more than one glass/day, secondary hypertension, congestive heart failure, liver cirrhosis, chronic renal failure Chronic Kidney Disease Epidemiology Collaboration formula [CKD-EPI estimated glomerular filtration rate (eGFR) <40 mL/min/1.73 m2], connective diseases, severe gastroesophageal reflux (Barrett's esophagus), atrium-ventricular conduction defects, pregnancy or lactation in the last 6 months, and postmenopausal hormonal replacement therapy.
Study design and procedures
The first 20 NGT, 20 PD, and 20 T2D consecutive patients, who following the run-in were still eligible for the 6 ± 1 weeks study, were randomized (1:1) to continue the previous antihypertensive treatment with HCTZ (12.5–25 mg per day) or to switch from HCTZ to amlodipine (2.5–10 mg orally, once a day) according to a prespecified flowchart of dose regulation based on 1-week steps (Fig. 1) and designed to obtain the same blood pressure control in both groups of treatment. The treatment dose changes were determined by physicians who were not in direct contact with the participants and all measurements and procedures were performed by personnel blinded to the treatment allocation (single blinded). Therefore, this was a parallel-group, prospective, randomized, open-label, single-blinded end-point design. Compliance was assessed by returned pill counts and tolerance by questionnaire.
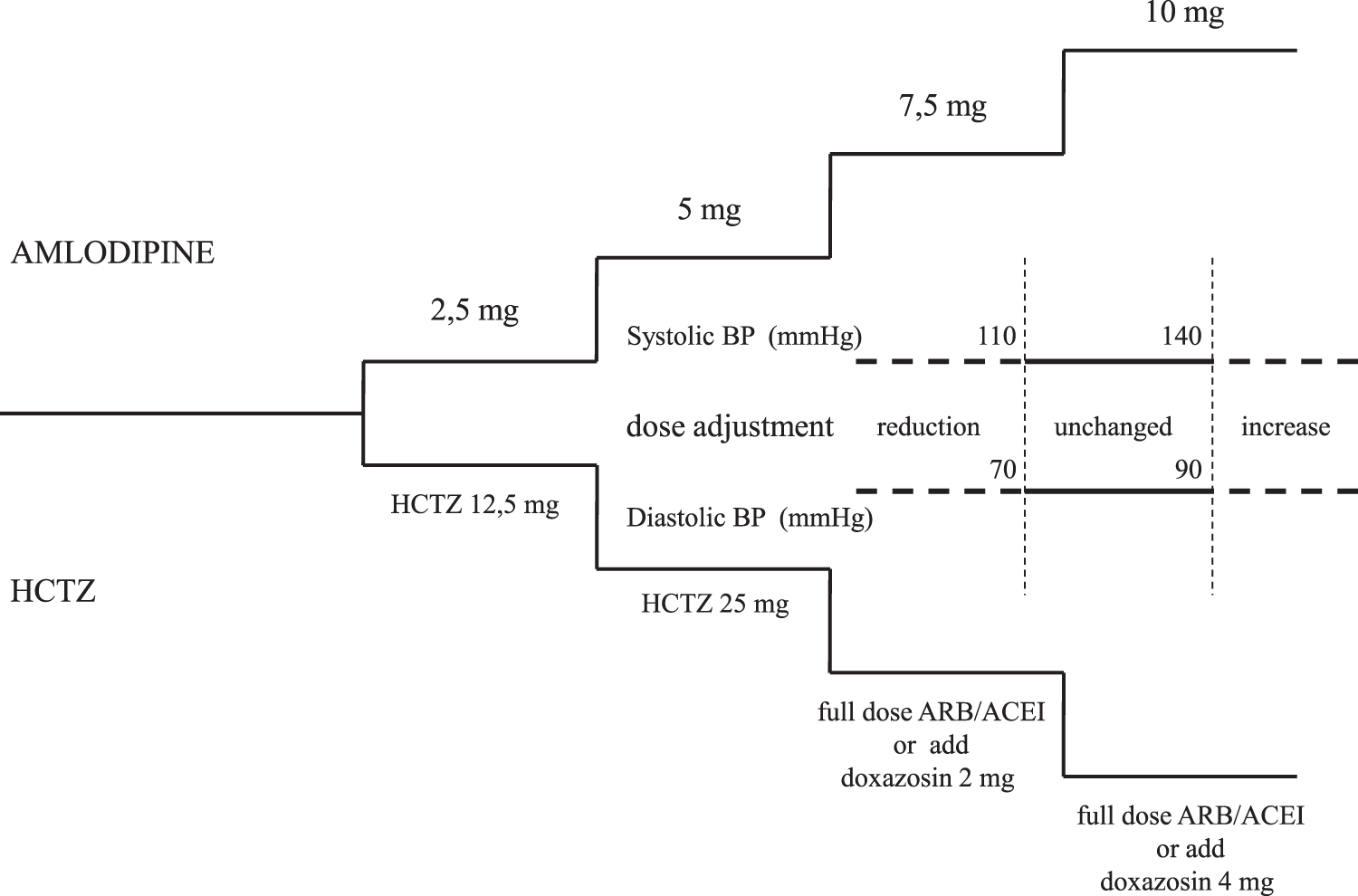
Flow chart of single-step dose regulation of amlodipine and HCTZ groups. ACEI, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; HCTZ, hydrochlorothiazide.
Endpoints were measured at baseline and 6 weeks after randomization; in both occasions, a venous blood sample was drawn in the morning in postabsorptive fasting conditions; oral glucose tolerance test (OGTT, g 75 oral load) was performed only in nondiabetic patients. The primary endpoints were the absolute change of 7-day continuous subcutaneous glucose monitoring (CSGM) glycemia, serum uric acid, and endothelial function [measured as flow-mediated dilation (FMD)]. Secondary endpoints were as follows: the changes of HbA1c, fasting plasma glucose (FPG), 2-hr OGTT glycemia, glycemic variability from 7-day CSGM, basal insulinemia, homeostasis model assessment of insulin resistance (HOMA-IR), total cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, and triglyceride (Tg) concentrations. Other exploratory endpoints concerned cardiovascular and renal function and included the following: intrarenal resistances measuring the echo-Doppler resistance index (RI) and pulsatility index (PI), carotid intima-media thickness (c-IMT), and the eGFR (CKD-EPI, Kidney Disease Outcomes Quality Initiative). Following randomization, participants were requested to register their home blood pressure values (at least one measurement per day; Omron M6; Omron Healthcare Co.; Matsusaka, Mie, Japan) and their blood glucose concentrations (at least five measurements per day once a week; Glucocard SM Meter; Menarini Diagnostics, Florence, Italy) as reported at telephone visits (week 1, 3, and 5) or exhibited on occasion of visits at the center (week 2, 4, and 6). Height and body weight were measured with participants lightly dressed and without shoes (SECA); the body mass index was calculated as body weight (kg)/height2 (m2). Body circumferences were measured at the umbilicus (waist circumference) and at the most prominent buttock level (hip circumference). Basal systolic and diastolic arterial blood pressure (two measurements obtained at 5-min intervals in seated position) and heart rate (Omron M6; Omron Healthcare Co.) were measured by physicians or dietitians according to standardized procedures. Body composition in terms of fat mass and fat-free mass was estimated using the bioelectrical impedance analysis (BIA; BIA-103, RJL, Detroit/Akern, Florence, Italy) as previously described. 13 Images of the right and left extracranial carotid artery walls were obtained in several projections with a high-resolution ultrasonographic 10-MHz linear array probe (Sonoline G50; Siemens, Germany). The end-diastolic c-IMT of the far wall of both common carotid arteries was measured as described elsewhere 14 ; the maximum value between right and left carotid c-IMT was considered for calculations. The endothelium-dependent reactivity was measured by brachial artery FMD using a high-resolution vascular ultrasound (Sonoline G50; Siemens) with a 10-MHz linear array transducer. 15 A video processing system computed the brachial artery diameter in real time by analyzing B-mode ultrasound images (FMD Studio; Institute of Physiology CNR, Pisa, Italy). The FMD was calculated as the maximum percentage of increase of brachial artery diameter over baseline. Endothelium-independent dilation was assessed after the administration of 300 mg sublingual glyceryl trinitrate. All FMD and glyceryl-trinitrate dilation assessments were performed by the same operator; ultrasound images were video recorded and analyzed by a trained reader. A portable, noninvasive SpaceLabs 90207 recorder (Redmond, WA) performed the 24-hr ABPM. Blood pressure readings were performed automatically at 20-min intervals during the day (from 7 a.m. to 10 p.m.) and at 30-min intervals during night-time resting (from 10 p.m. to 7 a.m.). Only records with more than 80% of valid data were accepted. The M-mode echocardiography, guided by a two-dimensional echocardiography, was performed using an Acuson Sequoia 512 (Siemens, Mountain View, CA). 16 In each of both kidneys, renal doppler flow was obtained (3.5 MHz probe) of the interlobar arteries 17 ; the mean of both kidneys RI [(peak systolic velocity − end diastolic velocity)/peak systolic velocity] and PI [(peak systolic velocity − end diastolic velocity)/mean velocity] were obtained as measures of intrarenal resistances.
The 7-day CSGM (ENLITE Glucose Sensor; Medtronic Minimed, Northridge, CA) was performed and average 7-day glycemia, standard deviation, coefficient of variability (standard deviation/mean, CV%), and number of hypoglycemic (glycemia <70 mg/dL) or hyperglycemic (glycemia >140 mg/dL) events were calculated. 18
FPG, total cholesterol, HDL-cholesterol, Tg, uric acid, and creatinine concentrations were measured using standard clinical chemistry methods (Roche Diagnostics, Monza, Italy). Basal insulin concentrations (Elecsys insulina; Roche Diagnostics), high-sensitivity C-reactive protein (hs-CRP; B-analyst hsCRP; Menarini Diagnostics, Florence, Italy), and HbA1c (B-analyst HbA1c; Menarini Diagnostics) were also measured. LDL cholesterol serum concentration was calculated with Friedewald's formula and eGFR was estimated based on the CKD-EPI equation. The insulin resistance was estimated according to the HOMA-IR formula: fasting plasma insulin (mUI/L) × fasting plasma glucose (mmol/L)/22.5. 19
Statistical methods
The sample size was calculated to detect a 5% reduction of the mean 24-hr glycemia from 7-day CSGM considering a baseline value of 130 ± 10 mg/dL; with a parallel group design, an α of 0.05, and power of 80%, 22 subjects per group were needed. Furthermore, in the case of endothelial function, to detect a 30% increase of FMD from a baseline value of 5 ± 3%, we computed that 25 subjects per group would provide 80% power at α < 0.05. To account for dropouts and to increase the power to find smaller changes, we included 30 participants per group. Data are presented as mean ± standard deviation for continuous variables, and as percentages for categorical variables. Baseline characteristics of participants of both groups were compared using the Student's t-test for unpaired data; categorical variables were compared using the χ 2. Changes in continuous variables from baseline to week 6 were analyzed by analysis of covariance, with treatment (HCTZ and amlodipine) as fixed effect and age, gender, baseline HbA1c, and body weight change (%) as covariates. Student's paired t-test was applied to evaluate changes in the subgroups of participants according to glucose tolerance. Pearson correlation coefficients were calculated to explore the associations among variables. A two-tailed P value <0.05 was considered significant. All analyses were done with Systat (Windows version 13.0; San Jose, CA).
Results
Participants were allocated in two groups, the HCTZ and the amlodipine group, respectively, each composed of 10 NGT, 10 PD, and 10 T2D people. Two NGT patients on amlodipine abandoned the study due to side effects (flushing and peripheral edema) and two participants (one NGT and one PD patient) on HCTZ retired from the study due to personal reasons. Anthropometric, clinical, and laboratory data of study groups are presented in Tables 1 and 2. Blood pressure control was comparable between the two groups also on the basis of ABPM 24-hr systolic and diastolic blood pressure (Table 2). The final average amlodipine dose was 5 mg (range 2.5–10 mg), and in this group, the number of participants treated with ACEI/ARBs or beta-blockers significantly decreased, while that of people on doxazosin increased (P < 0.001; Table 1). The antihypertensive treatment of the HCTZ group did not significantly change during the study. No patient was on HCTZ monotherapy. The use of concomitant antidiabetic medications remained substantially unchanged in both groups throughout the study (Table 1). Body weight was comparable between the two groups and remained unchanged throughout the study (HCTZ group: −1.0 ± 2.2 vs. amlodipine group 0.3 ± 2.6 kg; P = 0.07; Table 1). The metabolic and cardiovascular effects induced by the switch from HCTZ to amlodipine are reported in Tables 1 and 2. In particular, amlodipine was associated with a significant reduction of HbA1c (P = 0.03), of both 7-day CSGM glycemia (P = 0.01) and glycemic variability (CV%: HCTZ group +3%, amlodipine group −2.8%), and of uric acid concentrations (P < 0.001). Following amlodipine treatment, a significant reduction of bioelectrical phase angle (P = 0.04) and an increase of both eGFR (P = 0.01) and FMD (P = 0.02) were observed. Concerning each subgroup of glucose tolerance, the 7-day CSGM was significantly reduced from baseline to 6-week evaluation in the amlodipine-treated patients with T2D (141 ± 12 vs. 128 ± 13 mg/dL; P < 0.001); furthermore, in this subgroup, uric acid serum concentrations were reduced (6.5 ± 1.2 vs. 5.1 ± 1.2 mg/dL; P < 0.01), while FMD improved (2.8 ± 2.2 vs. 5.2 ± 1.8%; P < 0.05). Uric acid serum concentrations were significantly reduced also in the amlodipine-treated patients with PD (6.4 ± 1.1 vs. 4.9 ± 1.9 mg/dL; P < 0.05). The FMD change was uniquely inversely correlated with the serum uric acid change (r = −0.30; P = 0.02) and serum uric change was inversely correlated with the absolute change of eGFR (r = −0.52; P = 0.001) (Fig. 2).
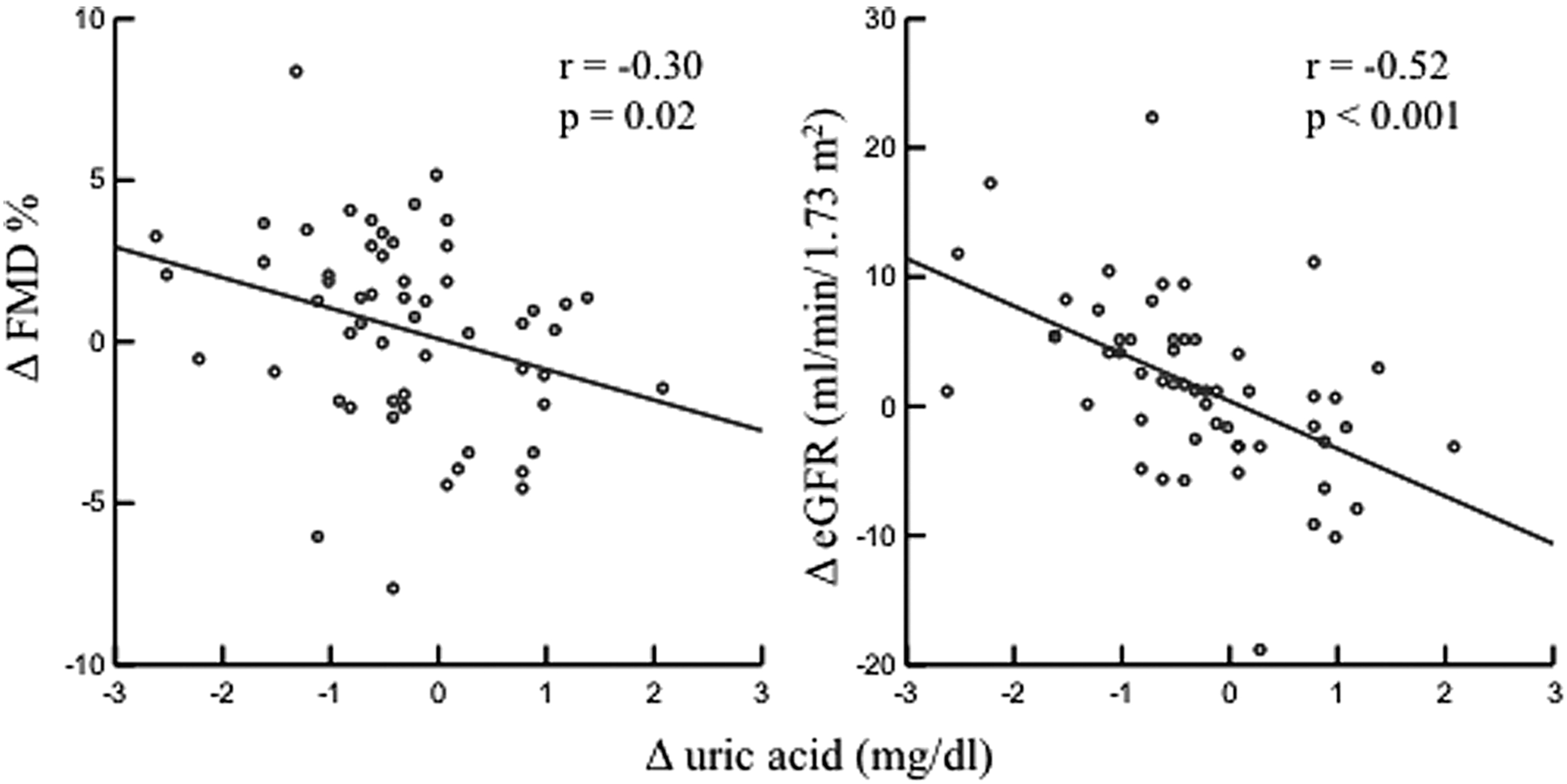
Correlations between change (Δ, 6 weeks after HCTZ or amlodipine treatment—baseline values) in serum uric acid concentrations, FMD and eGFR. eGFR, estimated glomerular filtration rate; FMD, flow-mediated dilation.
Clinical Characteristics of All Participants by Hydrochlorothiazide or Amlodipine Use at Baseline and Following Six Weeks of Treatment
Mean values ± SD or percentages if appropriate.
ANCOVA with treatment (amlodipine and hydrochlorothiazide) as fixed effect and baseline HbA1c, age, gender, and percentage of body weight change (from baseline to week 6) as covariates. Basal values of variables are not significantly different between groups by Student's t-test for independent samples. Differences of prevalence analyzed by χ 2 test.
ACEI, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blocker; At, atenolol; BIA, bioelectrical impedance analysis; BMI, body mass index; Ca, carvedilol; DPP4-I, dipeptidyl peptidase-4 inhibitors; eGFR, estimated glomerular filtration rate; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; HOMA-IR, homeostasis model assessment of insulin resistance; LDL, low-density lipoproteins; LV, left ventricle; Ne, nebivolol; NGT, normal glucose tolerance; OGTT, oral glucose tolerance test; PD, prediabetes; T2D, type 2 diabetes; SD, standard deviation; ANCOVA, analysis of covariance; HbA1c, glycated hemoglobin.
Metabolic and Cardiovascular Characteristics of All Participants by Hydrochlorothiazide or Amlodipine Use at Baseline and Following Six Weeks of Treatment
Mean values ± SD or median and CI if appropriate.
ANCOVA with treatment (amlodipine and hydrochlorothiazide) as fixed effect and baseline HbA1c, age, gender, and percentage of body weight change (from baseline to week 6) as covariates.
ABPM, ambulatory blood pressure monitoring; BP, blood pressure; CSGM, continuous subcutaneous glucose monitoring; ECG, electrocardiogram; FMD, flow-mediated dilation; GTN, glyceryl-trinitrate dilation; HbA1c, glycated hemoglobin; IMT, maximum intima-media thickness; CI, confidence interval; CV, coefficient of variability.
Discussion
The notion that hypertension is a condition of insulin resistance has been known for a long time. 20 Likewise, it has long been recognized that HCTZ, although at higher doses than those currently used, adversely affects insulin sensitivity. 21 Our study confirms these notions and provides further evidence that HCTZ has an unfavorable metabolic effect even at doses lower than those used in the past. In fact, we demonstrate that switching from HCTZ (12.5–25 mg per day) to amlodipine (2.5–10 mg per day) provides a wide range of advantageous metabolic and cardiovascular effects in hypertensive patients with or without T2D. In particular, discontinuing HCTZ in favor of amlodipine was associated with improvement of HbA1c, mean 7-day CSGM glycemia, glycemic variability, and uric acid concentrations. Furthermore, we observed a significant improvement of endothelial function, measured as FMD, in the group on amlodipine. These effects were more evident in diabetic and PD subgroups. Both the HCTZ and the amlodipine group exhibited similar blood pressure control throughout the study. It should be noted that, before randomization, HCTZ was used in combination with ACEI/ARBs in almost all (>80%) participants of both groups; however, when switched to amlodipine, the use of ACEI/ARBs was suspended in about 60% of patients. The ACEI/ARBs are acknowledged to improve insulin sensitivity and reduce the risk of developing T2D 22 ; therefore, the benefits observed in the amlodipine group were evident, despite this favorable category of medication being suspended in many cases. Due to the study design, we cannot discriminate if the favorable effects observed in the amlodipine group were exclusively due to the HCTZ treatment cessation or to direct advantageous metabolic and cardiovascular effects of amlodipine, or to both conditions. In fact, CCB have also been attributed favorable metabolic effects. In the ALLHAT study, 4 an increased incidence of new onset of T2D cases in those participants on diuretics compared with groups treated with ACEI or amlodipine was observed. Our results are also in agreement with other studies that demonstrated unfavorable metabolic effects of HCTZ when compared to CCB. 23 –25 Despite the hypothesis that the unfavorable effects of HCTZ on glucose metabolism are due to potassium depletion, 6 however, in this study, we do not observe any significant change in serum potassium concentrations in both groups of treatment. Concerning beta-blockers used by patients included in this study, differently from modern beta-blockers as carvedilol and nebivolol, old-generation beta-blockers as atenolol are known to adversely influence glucose metabolism. 7 Only three patients in the amlodipine group suspended the treatment with beta-blockers (Table 1), and in no case, the drug suspended was atenolol. Furthermore, the three participants who suspended the use of beta-blockers did not show a different pattern of change of the measurements obtained in this study, in comparison with the general trend of their group (data not showed). Therefore, changes in concomitant beta-blocker treatment are unlikely to have influenced the favorable metabolic effects observed in the amlodipine group.
About one of four patients with hypertension has hyperuricemia 26 and HCTZ is known to unfavorably influence uricemia. 27,28 In agreement with other reports, 29 our study confirms that switching from HCTZ to amlodipine significantly reduces serum uric acid concentrations. This result is of particular interest since uric acid has been demonstrated to activate the renin-angiotensin system and to favor the oxidant system, thus reducing the availability of nitric oxide at the endothelial level. These mechanisms may induce as endothelial dysfunction and insulin resistance, as increase in blood pressure. 30,31 In fact, it was demonstrated that serum uric acid was associated with endothelial dysfunction measured by FMD. 32 Interestingly, at the end of the study, we observed an inverse correlation between the change of FMD and that of uric acid concentrations (Fig. 2). We hypothesize that switching from HCTZ to amlodipine through the favorable effects on factors as serum uric acid concentrations, average glycemia, and glycemic variability might produce a cardiovascular risk reduction. In agreement with this hypothesis, we observed in the amlodipine group a significant improvement of the endothelial function as measured by the FMD of the brachial artery, a condition that is known to be associated with lower cardiovascular events. 33 –37 Vinereanu et al. 38 demonstrated that HCTZ has a neutral effect on endothelial function; therefore, we cannot exclude that the improvement of FMD in the amlodipine group was due to a direct favorable effect of amlodipine rather than the removal of a possible adverse effect of the HCTZ. Notably, the OLAS study 23 observed that amlodipine treatment had significant anti-inflammatory effects compared with HCTZ. Furthermore, HCTZ had unfavorable effects on the 2-hr OGTT glycemia as demonstrated by the STAR-LET 24 and the PATHWAYS-327 study. Interestingly, as inflammation as post-prandial glycemia are known to influence the endothelial function 18,39 and the cardiovascular risk as well. 40 To our knowledge, only one clinical trial, the ACCOMPLISH, 41 compared the association CCB/ACEI versus ACEI/HCTZ, demonstrating a significant reduction of 21% of cardiovascular events; therefore, our study gives evidence of potential mechanism that may explain the outcomes seen in the ACCOMPLISH study.
Our study also demonstrates that significant hemodynamic and renal changes with possible clinical implications are induced by switching from HCTZ to amlodipine. The BIA phase angle is a well-known bioelectrical body measure that is inversely correlated with the extracellular/intracellular body water ratio. 42 Interestingly, replacing HCTZ with amlodipine was associated with a reduction of BIA phase angle (in the normal range of values), thus suggesting a relative expansion of the extracellular water compartment after discontinuation of the diuretic treatment. Probably, the relative volume expansion was counterbalanced by the vasodilator effect of amlodipine so that blood pressure remained unchanged. We observed in this study that the use of amlodipine was followed by improvement of the GFR, an effect that was already detected by other studies. 43,44 However, this possibility is controversial since other studies failed to demonstrate an improvement of GFR following CCB treatment 45 or to demonstrate that the decline of GFR in hypertensive patients with or without renal failure is slowed by amlodipine treatment. 46 Interestingly, at the end of the study, we observed an inverse correlation (Fig. 2) between the change in serum uric acid concentrations and that of eGFR. It is not definitely established whether elevated uric acid levels are in consequence of impaired kidney function or have a pathogenic role in kidney function. 47 However, recent studies in humans 48 and in animal models 49 suggest that through different mechanisms, hyperuricemia may reduce the eGFR. Therefore, we cannot exclude that HCTZ increases uric acid levels with unfavorable influence on both endothelial and renal function.
Our study is burdened by some limitations. We acknowledge that the sample of patients investigated is rather small and that our results should be replicated, yet the effect size was considerable and very comparable to that found in a similar independently conducted study. 50 As we could not achieve a large sample size, our study is statistically underpowered for the assessment of clinical effects of HCTZ or amlodipine in subgroups of hypertensive patients categorized according to the degree of glucose tolerance. The duration of the study (6 weeks) was inadequate to detect a complete effect on HbA1c; however, we could observe a significant reducing trend; on the other side, a more prolonged duration of the study might have introduced other confounding factors linked to seasonal and nutritional, or less adherence of participants due to trial fatigue. Despite reporting that HOMA-IR (an indirect measure of fasting insulin resistance) did not change following switching from HCTZ to CCB, we did not directly investigate insulin resistance using suitable dynamic techniques as the clamp or the measurement of steady-state plasma glucose and insulin concentrations; therefore, we cannot give a definite answer to this, a relevant aspect that might contribute to explain the unfavorable action of HCTZ. This study has also some points of strength. In fact, this is one of the very few randomized controlled trials that assessed the effects of low-dose thiazide diuretics on different metabolic and cardiovascular endpoints in a group of patients that included the entire spectrum of glucose tolerance. In particular, no other study investigated the effects of HCTZ versus amlodipine on glycemic variability and FMD.
Conclusions
In summary, although thiazide diuretics effectively reduce blood pressure, they may have unfavorable metabolic effects affecting glucose metabolism, increasing serum concentrations of uric acid, and adversely influencing endothelial function. Since control of blood pressure has important benefits and is a priority especially in diabetic patients, further investigations are needed to clarify whether thiazide-induced metabolic changes are of clinical significance and may be prevented with prescription of alternative medications.
Footnotes
Acknowledgments
The results of this article were presented, in part, as a conference abstract in 119th national congress of the Italian Society of Internal Medicine (Rome, Italy, 2018).
Author Contributions
S.B. contributed to the conception and design of the study, acquisition, and analysis and interpretation of data, and wrote the article. C.B. and A.M.B. contributed to the design of the study and analysis and interpretation of data, performed the research. L.C., G.R., and C.R. performed the research and recruited participants, contributed to the acquisition of data. D.C. and D.D.R. contributed to the acquisition of data. F.R.P. contributed to the interpretation of data. G.P. contributed to the conception and design of the study and analysis and interpretation of data. All authors critically revised the article and approved the final version. S.B. is the guarantor of this work and, as such, had full access to all data in the study, and takes responsibility for the integrity of data and the accuracy of data analysis.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.